
The Impact of Heatwaves on Community Morbidity and Healthcare Usage: A Retrospective Observational Study Using Real-Time Syndromic Surveillance

 ,
,  ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Period
2.2. Syndromic Surveillance Systems

{kind=link}
{kind=link}
{kind=link}
| Surveillance System | Approximate Population Coverage (% of England Population) | Syndromic Indicator | ||
|---|---|---|---|---|
| Cardiovascular | Respiratory | Others | ||
| GP in hours (GPIH) | 35 million (64%) | Myocardial infarction * | Asthma, wheeze | Cerebrovascular accident * |
| GP out of hours (GPOOH) | 33 million (60%) | N/A | Asthma, Asthma/Wheeze/Difficulty Breathing | Fever, rash, cerebrovascular accident |
| Emergency department (EDSSS) | 35 sentinel EDs † | Myocardial ischaemia | Asthma, Asthma/Wheeze/Difficulty Breathing | Cerebrovascular accident |
2.3. Syndromic Surveillance Data Analysis
2.4. Meteorological Data Sources
2.5. Trend Analyses
2.6. Incidence Rate Ratios
2.7. GPIH Risk Group Analysis
3. Results and Discussion
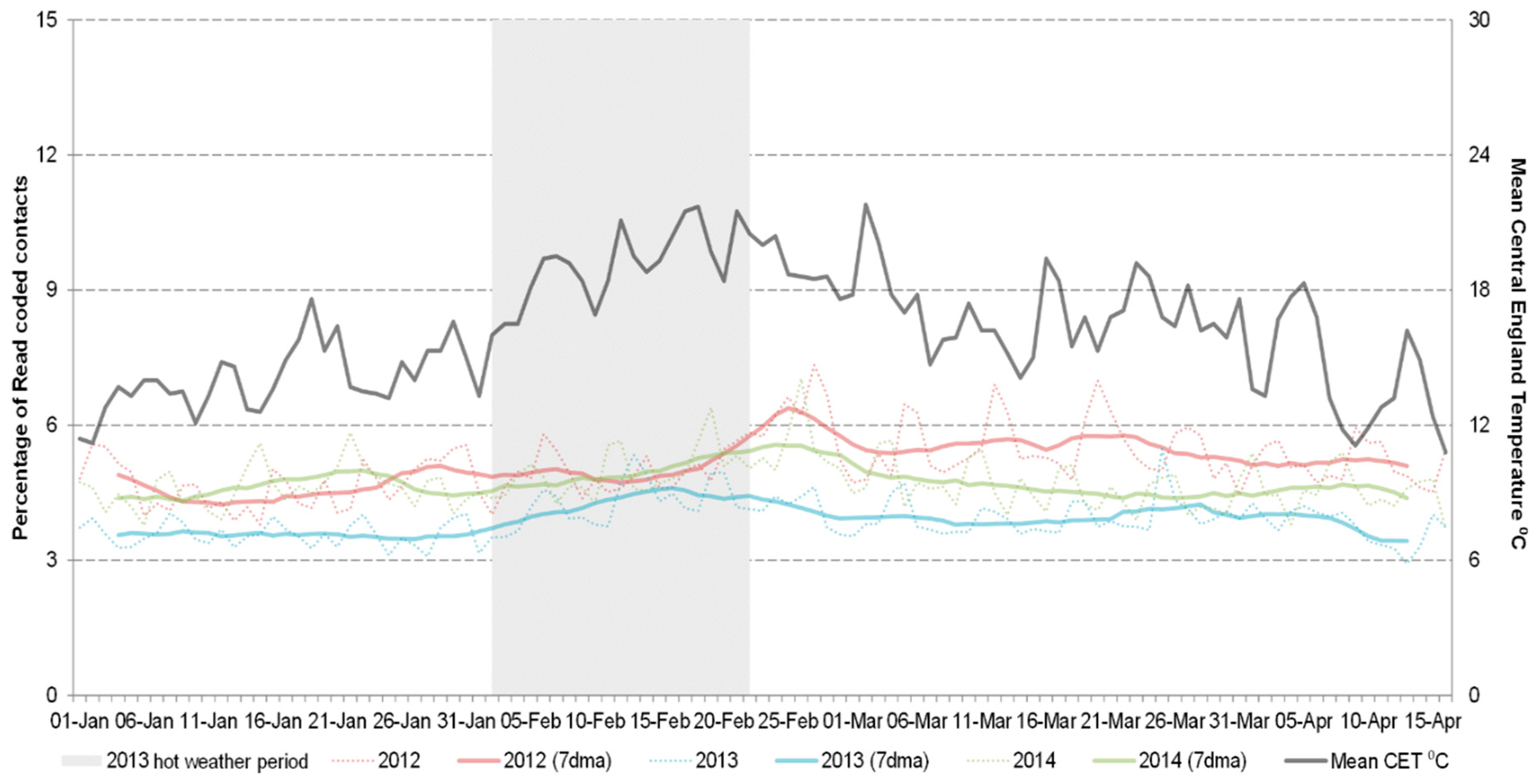
3.1. General Practitioner in Hours Consultations

| Age Group | GPIH Myocardial Infarction Incidence Rate Ratio (95% CI) | EDSSS Myocardial Ischaemia Incidence Rate Ratio (95% CI) | ||
|---|---|---|---|---|
| 0 to 4 | – | – | – | – |
| 5 to 14 | 0.00 | – | – | – |
| 15 to 64 | 0.92 | (0.70–1.14) | 0.88 | (0.50–1.27) |
| 65 to 74 | 0.77 | (0.30–1.23) | 0.88 | (0.46–1.29) |
| 75 plus | 1.07 | (0.80–1.34) | 0.75 | (0.65–0.84) |
| all ages | 0.92 | (0.75–1.09) | 0.84 | (0.57–1.11) |
3.2. General Practitioner in Hours Syndromic Indicators by Risk Group
3.3. General Practitioner Out of Hours Consultations
| Indicator | 2012 | 2013 | 2014 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Risk Group | No Risk | % Cases in Risk Group (95% CI) | Risk Group | No Risk | % Cases in Risk Group (95% CI) | Risk Group | No Risk | % Cases in Risk Group (95% CI) | |
| Asthma | 1939 | 1358 | 59 (57.1–60.5) | 1948 | 1028 | 65 (63.7–67.2) | 2296 | 1089 | 68 (66.2–69.4) |
| Myocardial infarction | 515 | 1128 | 31 (29.2–33.6) | 692 | 1229 | 36 (33.9–38.2) | 675 | 1232 | 35 (33.3–37.6) |
| Cerebrovascular accident | 708 | 885 | 44 (42.0–46.9) | 840 | 1053 | 44 (42.2–46.6) | 868 | 1011 | 46 (44.0–48.5) |
| Wheeze | 3290 | 7025 | 32 (31.0–32.8) | 3564 | 6300 | 36 (35.2–37.1) | 3887 | 6137 | 39 (37.8–39.7) |

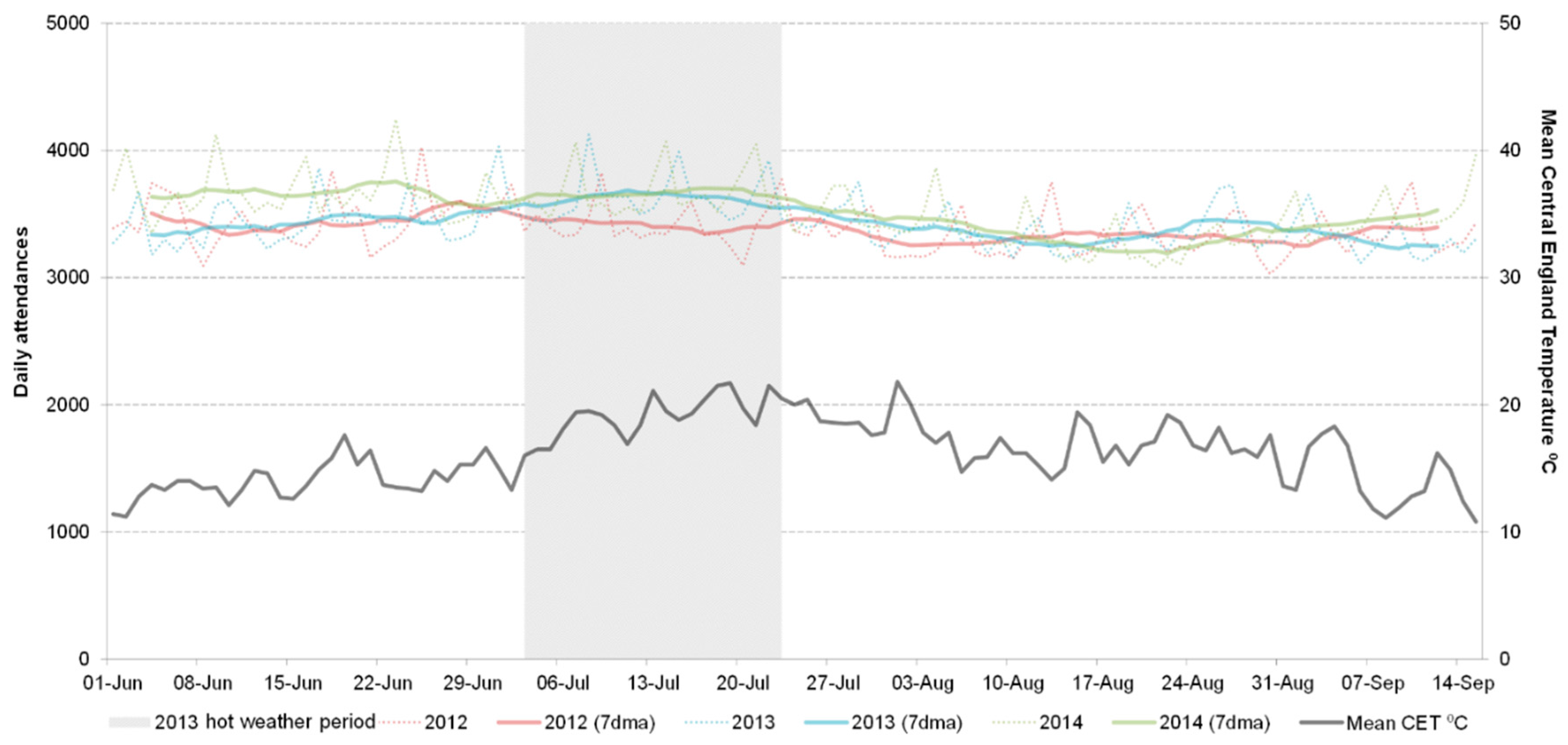
3.4. Emergency Department Attendances

4. Conclusions
4.1. Main Findings
4.2. How does This Work Compare to Others?
4.3. Limitations
4.4. Clinical Implications
4.5. Implications for Heatwave Plans
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Basu, R.; Samet, J.M. Relation between elevated ambient temperature and mortality: A review of the epidemiologic evidence. Epidemiol. Rev. 2002, 24, 190–202. [Google Scholar] [CrossRef]
- D’Ippoliti, D.; Michelozzi, P.; Marino, C.; de’Donato, F.; Menne, B.; Katsouyanni, K.; Kirchmayer, U.; Analitis, A.; Medina-Ramon, M.; Paldy, A.; et al. The Impact of Heat Waves on Mortality in 9 European cities: Results from the EuroHEAT project. Environ. Health 2010. [Google Scholar] [CrossRef] [PubMed]
- Kovats, R.S.; Kristie, L.E. Heatwaves and public health in Europe. Eur. J. Public Health 2006, 16, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Gu, S.; Bi, P.; Yang, J.; Liu, Q. Heat waves and morbidity: Current knowledge and further direction—A comprehensive literature review. Int. J. Environ. Res. Public. Health 2015, 12, 5256–5283. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.; Elliot, A.J.; Hajat, S.; Bone, A.; Smith, G.E.; Kovats, R.S. Estimating the burden of heat/sun stroke in England during the 2013 summer heatwave using syndromic surveillance. J. Epidemiol. Community Health 2015. [Google Scholar] [CrossRef]
- Bagcchi, S. More could be done to protect people from heatwave in India, say campaigners. BMJ 2015. [Google Scholar] [CrossRef] [PubMed]
- Clark, J. Pakistan authorities trade blame as heatwave deaths exceed 800. BMJ 2015. [Google Scholar] [CrossRef] [PubMed]
- Kysely, J.; Kim, J. Mortality during heat waves in South Korea, 1991 to 2005: How exceptional was the 1994 heat wave? Clim. Res. 2009, 38, 105–116. [Google Scholar] [CrossRef]
- Semenza, J.C.; McCullough, J.E.; Flanders, W.D.; McGeehin, M.A.; Lumpkin, J.R. Excess hospital admissions during the July 1995 heat wave in Chicago. Am. J. Prev. Med. 1999, 16, 269–277. [Google Scholar] [CrossRef]
- Whitman, S.; Good, G.; Donoghue, E.R.; Benbow, N.; Shou, W.; Mou, S. Mortality in Chicago attributed to the July 1995 heat wave. Am. J. Public Health 1997, 87, 1515–1518. [Google Scholar] [CrossRef] [PubMed]
- Robine, J.M.; Cheung, S.L.; le Roy, S.; van Oyen, H.; Griffiths, C.; Michel, J.P.; Herrmann, F.R. Death toll exceeded 70,000 in Europe during the summer of 2003. C. R. Biol. 2008, 331, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Johnson, H.; Kovats, R.S.; McGregor, G.; Stedman, J.; Gibbs, M.; Walton, H. The impact of the 2003 heat wave on daily mortality in England and Wales and the use of rapid weekly mortality estimates. Euro. Surveill. 2005, 10, 168–171. [Google Scholar] [PubMed]
- Johnson, H.; Kovats, R.S.; McGregor, G.; Stedman, J.; Gibbs, M.; Walton, H.; Cook, L.; Black, E. The impact of the 2003 Heat Wave on Mortality and Hospital Admissions in England. Health Stat. Q. 2005, 25, 6–11. Available online: http://cedadocs.badc.rl.ac.uk/291/ (accessed on 23 June 2015). [Google Scholar]
- Fouillet, A.; Rey, G.; Laurent, F.; Pavillon, G.; Bellec, S.; Guihenneuc-Jouyaux, C.; Clavel, J.; Jougla, E.; Hemon, D. Excess mortality related to the August 2003 heat wave in France. Int. Arch. Occup. Environ. Health 2006, 80, 16–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandentorren, S.; Suzan, F.; Medina, S.; Pascal, M.; Maulpoix, A.; Cohen, J.C.; Ledrans, M. Mortality in 13 French cities during the August 2003 heat wave. Am. J. Public Health 2004, 94, 1518–1520. [Google Scholar] [CrossRef] [PubMed]
- Doherty, R.M.; Heal, M.R.; Wilkinson, P.; Pattenden, S.; Vieno, M.; Armstrong, B.; Atkinson, R.; Chalabi, Z.; Kovats, S.; Milojevic, A.; et al. Current and future climate- and air pollution-mediated impacts on human health. Environ. Health 2009. [Google Scholar] [CrossRef] [PubMed]
- Watts, N.; Adger, W.N.; Agnolucci, P.; Blackstock, J.; Byass, P.; Cai, W.; Chaytor, S.; Colbourn, T.; Collins, M.; Cooper, A.; et al. Health and climate change: Policy responses to protect public health. Lancet 2015, 386, 1861–1914. [Google Scholar] [CrossRef]
- Hajat, S.; Vardoulakis, S.; Heaviside, C.; Eggen, B. Climate change effects on human health: Projections of temperature-related mortality for the UK during the 2020s, 2050s and 2080s. J. Epidemiol. Community Health 2014, 68, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Heatwave Plan for England. Available online: https://www.gov.uk/government/publications/heatwave-plan-for-england (accessed on 23 June 2015).
- Triple S Project. Assessment of syndromic surveillance in Europe. Lancet 2012, 378, 1833–1834. [Google Scholar]
- Elliot, A.J.; Bone, A.; Morbey, R.; Hughes, H.E.; Harcourt, S.; Smith, S.; Loveridge, P.; Green, H.K.; Pebody, R.; Andrews, N.; et al. Using real-time syndromic surveillance to assess the health impact of the 2013 heatwave in England. Environ. Res. 2014, 135, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Flamand, C.; Larrieu, S.; Couvy, F.; Jouves, B.; Josseran, L.; Filleul, L. Validation of a Syndromic Surveillance System Using a General Practitioner House Calls Network, Bordeaux, France. Euro Surveill. 2008, 13, pii:18905. Available online: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=18905 (accessed on 23 June 2015). [Google Scholar]
- Josseran, L.; Fouillet, A.; Caillere, N.; Brun-Ney, D.; Ilef, D.; Brucker, G.; Medeiros, H.; Astagneau, P. Assessment of a syndromic surveillance system based on morbidity data: Results from the Oscour network during a heat wave. PLoS ONE 2010. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, G.S.; Hajat, S.; Kovats, R.S.; Smith, G.E.; Cooper, D.; Gerard, E. Syndromic surveillance use to detect the early effects of heat-waves: An analysis of NHS Direct data in England. Soz. Praventivmed. 2006, 51, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Perry, A.G.; Korenberg, M.J.; Hall, G.G.; Moore, K.M. Modeling and syndromic surveillance for estimating weather-induced heat-related illness. J. Environ. Public Health 2011. [Google Scholar] [CrossRef] [PubMed]
- Met Office. Heat-Health Watch. Available online: http://www.metoffice.gov.uk/public/weather/heat-health/ (accessed on 23 June 2015).
- Met Office. Hot Dry Spell July 2013. Available online: http://www.metoffice.gov.uk/climate/uk/interesting/2013-heatwave (accessed on 7 Novebmer 2013).
- Elliot, A.J.; Morbey, R.A.; Hughes, H.E.; Harcourt, S.E.; Smith, S.; Loveridge, P.; Edeghere, O.; Ibbotson, S.; McCloskey, B.; Catchpole, M.; et al. Syndromic surveillance—A public health legacy of the London 2012 Olympic and Paralympic Games. Public Health 2013, 127, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Morbey, R.A.; Elliot, A.J.; Charlett, A.; Verlander, N.Q.; Andrews, N.; Smith, G.E. The application of a novel “rising activity, multi-level mixed effects, indicator emphasis” (RAMMIE) method for syndromic surveillance in England. Bioinformatics 2015, 31, 3660–3665. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Kan, H.; Kovats, S. The impact of the 2003 heat wave on mortality in Shanghai, China. Sci. Total Environ. 2010, 408, 2418–2420. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Y.; Barnett, A.G.; Yu, W.; FitzGerald, G.; Tippett, V.; Aitken, P.; Neville, G.; McRae, D.; Verrall, K.; Tong, S. The impact of heatwaves on mortality and emergency hospital admissions from non-external causes in Brisbane, Australia. Occup. Environ. Med. 2012, 69, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Met Office. Hadley Centre Central England Temperature (HadCET) Dataset. Available online: http://www.metoffice.gov.uk/hadobs/hadcet/ (accessed on 16 March 2015).
- Franz, V.H. Ratios: A Short Guide to Confidence Limits and Proper Use. Available online: http://arxiv.org/pdf/0710.2024.pdf (accessed on 19 December 2012).
- Department of Health; Public Health England; NHS England. The National Flu Immunisation Programme 2015/16. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/418428/Annual_flu_letter_24_03_15__FINALv3_para9.pdf (accessed on 8 July 2015).
- Public Health England; Department of Health. Immunisation against Infectious Disease. Available online: https://www.gov.uk/government/publications/immunisation-against-infectious-disease-the-green-book-front-cover-and-contents-page (accessed on 20 November 2015).
- Scottish Clinical Information Management in Practice. PRIMIS+ Codes for Chronic Disease Groups Relating to Influenza Immunisation. Available online: http://www.scimp.scot.nhs.uk/wp-content/uploads/PRIMIS-Risk-Group-codes-2015-16.pdf (accessed on 24 November 2015).
- Bhaskaran, K.; Hajat, S.; Haines, A.; Herrett, E.; Wilkinson, P.; Smeeth, L. Short term effects of temperature on risk of myocardial infarction in England and Wales: Time series regression analysis of the Myocardial Ischaemia National Audit Project (MINAP) registry. BMJ 2010. [Google Scholar] [CrossRef] [PubMed]
- Bhaskaran, K.; Hajat, S.; Haines, A.; Herrett, E.; Wilkinson, P.; Smeeth, L. Effects of ambient temperature on the incidence of myocardial infarction. Heart 2009, 95, 1760–1769. [Google Scholar] [CrossRef] [PubMed]
- Turner, L.R.; Connell, D.; Tong, S. The effect of heat waves on ambulance attendances in Brisbane, Australia. Prehospital Disaster Med. 2013, 28, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.; Talbott, E.O.; Kan, H.; Prins, C.A.; Xu, X. The effects of heat stress and its effect modifiers on stroke hospitalizations in Allegheny County, Pennsylvania. Int. Arch. Occup. Environ. Health 2014, 87, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Kovats, R.S.; Hajat, S.; Wilkinson, P. Contrasting patterns of mortality and hospital admissions during hot weather and heat waves in Greater London, UK. Occup. Environ. Med. 2004, 61, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Michelozzi, P.; Accetta, G.; de Sario, M.; D’Ippoliti, D.; Marino, C.; Baccini, M.; Biggeri, A.; Anderson, H.R.; Katsouyanni, K.; Ballester, F.; et al. High temperature and hospitalizations for cardiovascular and respiratory causes in 12 European cities. Am. J. Respir. Crit. Care Med. 2009, 179, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Empana, J.P.; Sauval, P.; Ducimetiere, P.; Tafflet, M.; Carli, P.; Jouven, X. Increase in out-of-hospital cardiac arrest attended by the medical mobile intensive care units, but not myocardial infarction, during the 2003 heat wave in Paris, France. Crit. Care Med. 2009, 37, 3079–3084. [Google Scholar] [CrossRef] [PubMed]
- Green, H.K.; Andrews, N.; Pebody, R. Mortality during the 2013 heatwave in England. Environ. Res. 2015. (Under Review). [Google Scholar]
- Davidkovova, H.; Plavcova, E.; Kyncl, J.; Kysely, J. Impacts of hot and cold spells differ for acute and chronic ischaemic heart diseases. BMC Public Health 2014. [Google Scholar] [CrossRef] [PubMed]
- Zacharias, S.; Koppe, C.; Mucke, H.G. Influenza of heat waves on ischemic heart disease in Germany. Climate 2014, 2, 133–152. [Google Scholar] [CrossRef]
- Green, H.K.; Andrews, N.J.; Bickler, G.; Pebody, R.G. Rapid estimation of excess mortality: Nowcasting during the heatwave alert in England and Wales in June 2011. J. Epidemiol. Community Health 2012, 66, 866–868. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, S.; Elliot, A.J.; Hajat, S.; Bone, A.; Bates, C.; Smith, G.E.; Kovats, S. The Impact of Heatwaves on Community Morbidity and Healthcare Usage: A Retrospective Observational Study Using Real-Time Syndromic Surveillance. Int. J. Environ. Res. Public Health 2016, 13, 132. https://doi.org/10.3390/ijerph13010132
Smith S, Elliot AJ, Hajat S, Bone A, Bates C, Smith GE, Kovats S. The Impact of Heatwaves on Community Morbidity and Healthcare Usage: A Retrospective Observational Study Using Real-Time Syndromic Surveillance. International Journal of Environmental Research and Public Health. 2016; 13(1):132. https://doi.org/10.3390/ijerph13010132
Chicago/Turabian StyleSmith, Sue, Alex J. Elliot, Shakoor Hajat, Angie Bone, Chris Bates, Gillian E. Smith, and Sari Kovats. 2016. "The Impact of Heatwaves on Community Morbidity and Healthcare Usage: A Retrospective Observational Study Using Real-Time Syndromic Surveillance" International Journal of Environmental Research and Public Health 13, no. 1: 132. https://doi.org/10.3390/ijerph13010132
APA StyleSmith, S., Elliot, A. J., Hajat, S., Bone, A., Bates, C., Smith, G. E., & Kovats, S. (2016). The Impact of Heatwaves on Community Morbidity and Healthcare Usage: A Retrospective Observational Study Using Real-Time Syndromic Surveillance. International Journal of Environmental Research and Public Health, 13(1), 132. https://doi.org/10.3390/ijerph13010132