
A Walk in the Park: The Influence of Urban Parks and Community Violence on Physical Activity in Chelsea, MA

 ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Physical Activity
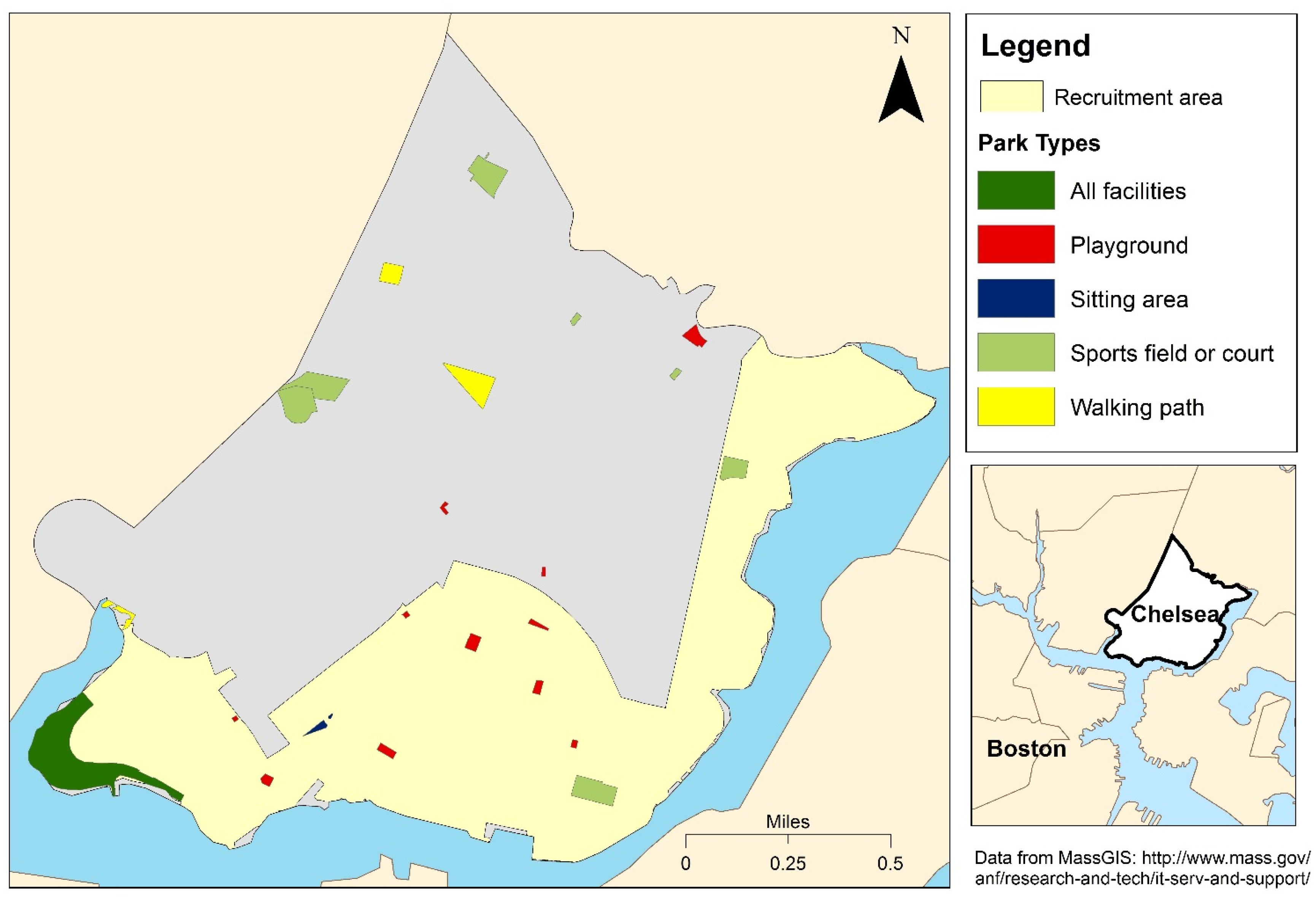
2.2. Park Access
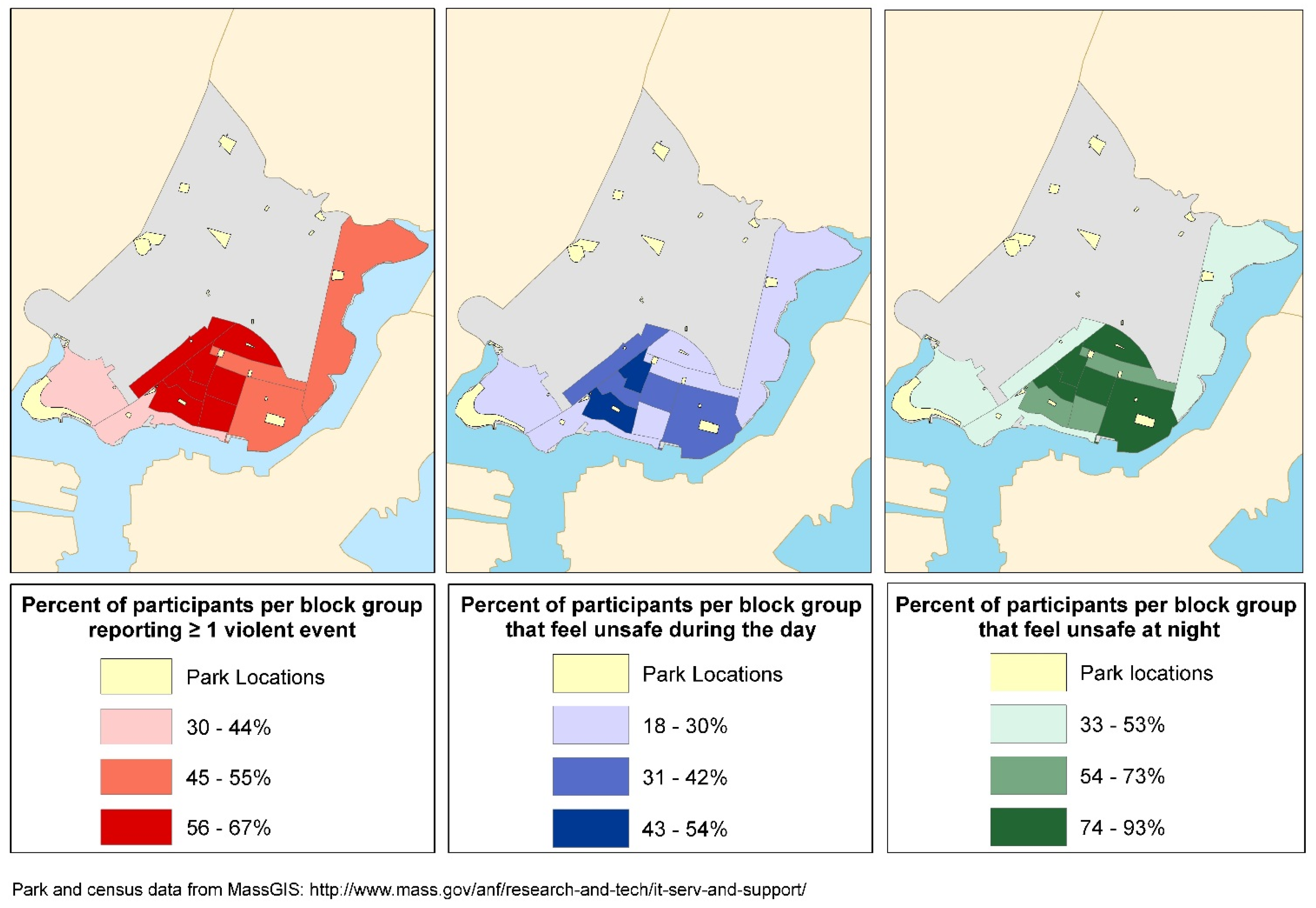
2.3. Knowledge of Community Violence and Feeling Unsafe
2.4. Individual Determinants
2.5. Statistical Analyses
3. Results and Discussion
3.1. Results

{kind=link}
{kind=link}
| Population Characteristics | Category | n | % |
|---|---|---|---|
| Sex | Female | 239 | 68 |
| Male | 113 | 32 | |
| Ethnicity | Not Latino | 137 | 39 |
| Latino | 215 | 61 | |
| Education | ≥High school | 231 | 66 |
| <High school | 121 | 34 | |
| Reported injury or impairment | Yes | 116 | 33 |
| No | 236 | 67 | |
| Children <18 years | Yes | 132 | 37 |
| No | 220 | 63 | |
| Age (years) | 18–44 | 152 | 43 |
| 45–59 | 108 | 31 | |
| 60+ | 92 | 26 |
| Physical Activity, Parks, and Community Violence | n | % |
|---|---|---|
| Any-PA | 249 | 71 |
| Indoor-PA | 98 | 28 |
| Outdoor-PA | 139 | 39 |
| Park-based PA | 61 | 17 |
| Facilities in parks nearest home | ||
| Playground/Tot lot | 256 | 73 |
| Sitting area | 49 | 14 |
| Sports field/court or walking path | 3 | 1 |
| All facility types | 44 | 13 |
| Knowledge of community violence | ||
| Gang fight | 41 | 12 |
| Fight with weapon | 88 | 25 |
| Robbery or mugging | 93 | 26 |
| Rape or sexual assault | 20 | 6 |
| Violent argument | 116 | 33 |
| Personal experience with violence | 94 | 27 |
| ≥1 Reported violent event (community or personal) | 215 | 61 |

| Demographics | Any-PA (n = 352) | Indoor-PA (n = 201) | Outdoor-PA (n = 242) | Park-Based PA (n = 164) | ||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Age | ||||||||
| >60 years | 1.20 | 0.89, 1.63 | 1.43 ** | 1.05, 1.95 | 1.18 | 0.89, 1.56 | 1.14 | 0.70, 1.87 |
| 45–59 years | 1.11 | 0.82, 1.49 | 1.02 | 0.70, 1.48 | 1.19 | 0.93, 1.52 | 1.00 | 0.62, 1.61 |
| 18–44 years | 1 | 1 | 1 | 1 | ||||
| Sex | ||||||||
| Female | 0.79 * | 0.61, 1.03 | 0.68 ** | 0.52, 0.89 | 0.71 ** | 0.58, 0.87 | 0.49 ** | 0.34, 0.71 |
| Male | 1 | 1 | 1 | 1 | ||||
| Education | ||||||||
| <High School | 0.76 * | 0.58, 1.00 | 0.46 ** | 0.31, 0.69 | 0.75 ** | 0.59, 0.96 | 0.37 ** | 0.21, 0.66 |
| ≥High School | 1 | 1 | 1 | 1 | ||||
| Ethnicity | ||||||||
| Latino | 0.75 ** | 0.59, 0.97 | 0.60 ** | 0.46, 0.79 | 0.65 ** | 0.53, 0.80 | 0.55 ** | 0.38, 0.81 |
| Not Latino | 1 | 1 | 1 | 1 | ||||
| Children <18 years | ||||||||
| Yes | 0.83 | 0.64, 1.08 | 0.76 * | 0.56, 1.03 | 0.79 * | 0.62, 1.00 | 0.71 | 0.46, 1.08 |
| No | 1 | 1 | 1 | 1 | ||||
| Injury or impairment | ||||||||
| Yes | 0.76 * | 0.57, 1.01 | 0.43 ** | 0.27, 0.69 | 0.76 ** | 0.59, 0.98 | 0.47 ** | 0.27, 0.81 |
| No | 1 | 1 | 1 | 1 | ||||
| Park Categories | Any-PA (n = 352) | Indoor-PA (n = 201) | Outdoor-PA (n = 242) | Park-Based PA (n = 164) | ||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| All parks | ||||||||
| Quartile 1: 23–85 m | 0.92 | 0.77, 1.11 | 0.94 | 0.66, 1.33 | 0.84 | 0.62, 1.15 | 0.88 | 0.47, 1.62 |
| Quartile 2: 86–153 m | 1.05 | 0.89, 1.24 | 1.19 | 0.85, 1.68 | 1.06 | 0.81, 1.38 | 1.58 * | 0.99, 2.53 |
| Quartile 3: 154–236 m | 0.92 | 0.76, 1.12 | 0.93 | 0.63, 1.36 | 0.87 | 0.65, 1.18 | 0.87 | 0.47, 1.61 |
| Quartile 4: >236 m | 1 | 1 | 1 | 1 | ||||
| Parks with sports/walking facilities | ||||||||
| Quartile 1: 75–461 m | 0.99 | 0.82, 1.21 | 1.07 | 0.70, 1.65 | 0.96 | 0.71, 1.31 | 0.82 | 0.50, 1.34 |
| Quartile 2: 463–638 m | 1.03 | 0.84, 1.25 | 1.03 | 0.65, 1.63 | 1.06 | 0.80, 1.41 | 0.67 | 0.38, 1.19 |
| Quartile 3: 640–835 m | 0.95 | 0.77, 1.18 | 0.99 | 0.63, 1.57 | 0.97 | 0.70, 1.33 | 0.85 | 0.52, 1.38 |
| Quartile 4: >835 m | 1 | 1 | 1 | 1 | ||||
| Resident-preferred park | ||||||||
| Quartile 1: 75–866 m | 1.11 * | 0.94, 1.32 | 1.45 ** | 1.02, 2.05 | 1.07 | 0.79, 1.44 | 2.42 ** | 1.12, 5.24 |
| Quartile 2: 899–1269 m | 1.00 | 0.80, 1.24 | 1.03 | 0.65, 1.63 | 1.00 | 0.72, 1.39 | 2.27 ** | 1.06, 4.87 |
| Quartile 3: 1270–1606 m | 1.10 | 0.90, 1.35 | 1.01 | 0.63, 1.61 | 1.24 * | 0.93, 1.65 | 2.15 * | 0.96, 4.81 |
| Quartile 4: >1606 m | 1 | 1 | 1 | 1 | ||||
| Community Violence | Response | Any-PA (n = 352) | Indoor-PA (n = 201) | Outdoor-PA (n = 242) | Park-Based PA (n = 164) | ||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | ||
| Types of violent events | |||||||||
| Gang fight | Yes | 0.98 | 0.77, 1.24 | 0.95 | 0.61, 1.47 | 1.06 | 0.74, 1.52 | 1.34 | 0.84, 2.15 |
| No | 1 | 1 | 1 | 1 | |||||
| Fight using weapon | Yes | 0.98 | 0.84, 1.16 | 0.92 | 0.67, 1.27 | 0.99 | 0.76, 1.29 | 0.89 | 0.57, 1.4 |
| No | 1 | 1 | 1 | 1 | |||||
| Violent argument | Yes | 1.02 | 0.89, 1.17 | 0.99 | 0.75, 1.31 | 1.07 | 0.86, 1.34 | 1.33 | 0.92, 1.93 |
| No | 1 | 1 | 1 | 1 | |||||
| Sexual assault or rape | Yes | 0.64 * | 0.39, 1.04 | 0.52 | 0.23, 1.20 | 0.46 * | 0.20, 1.05 | 0.35 | 0.10, 1.18 |
| No | 1 | 1 | 1 | 1 | |||||
| Robbery or mugging | Yes | 0.99 | 0.86, 1.15 | 1.03 | 0.79, 1.35 | 0.99 | 0.76, 1.29 | 1.10 | 0.73, 1.64 |
| No | 1 | 1 | 1 | 1 | |||||
| Personal experience with violence | Yes | 0.96 | 0.83, 1.13 | 0.96 | 0.69, 1.34 | 0.95 | 0.74, 1.21 | 1.17 | 0.80, 1.72 |
| No | 1 | 1 | 1 | 1 | |||||
| Knowledge of multiple violent events | 1 event | 1.04 | 0.9, 1.21 | 1.13 | 0.68, 1.86 | 1.11 | 0.87, 1.42 | 1.04 | 0.62, 1.76 |
| 2 events | 0.96 | 0.79, 1.16 | 1.04 | 0.60, 1.82 | 0.90 | 0.66, 1.23 | 1.20 | 0.74, 1.93 | |
| ≥3 events | 0.99 | 0.80, 1.21 | 0.91 | 0.50, 1.67 | 1.04 | 0.74, 1.46 | 1.22 | 0.73, 2.06 | |
| No events | 1 | 1 | 1 | 1 | |||||
| Feeling Unsafe as a Problem | Any-PA (n = 352) | Indoor-PA (n = 201) | Outdoor-PA (n = 242) | Park-Based PA (n = 164) | ||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Feels unsafe during the day | ||||||||
| Minor problem | 0.97 | 0.82, 1.15 | 0.94 | 0.54, 1.63 | 0.97 | 0.74, 1.26 | 1.02 | 0.67, 1.53 |
| Serious problem | 1.10 | 0.88, 1.37 | 1.13 | 0.61, 2.08 | 1.14 | 0.79, 1.66 | 1.41 | 0.79, 2.53 |
| No problem/No opinion | 1 | 1 | 1 | 1 | ||||
| Feels unsafe at night | ||||||||
| Minor problem | 0.99 | 0.84, 1.16 | 0.99 | 0.59, 1.65 | 0.99 | 0.77, 1.29 | 0.82 | 0.51, 1.31 |
| Serious problem | 0.98 | 0.83, 1.16 | 0.96 | 0.58, 1.59 | 0.98 | 0.76, 1.28 | 0.93 | 0.57, 1.50 |
| No problem/No opinion | 1 | 1 | 1 | 1 | ||||

3.2. Discussion
Strengths and Limitations
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix
A.1. Physical Activity
A.2. Park Use
A.3. Community Violence and Feeling Unsafe
A.3.1. Knowledge of Neighborhood Crime
A.3.2. Personal Experience with Violence
A.3.3. Feeling Unsafe [21]
References
- CDC. Facts about Physical Activity. Available online: http://www.cdc.gov/physicalactivity/data/facts.html (accessed on 1 August 2014).
- Cohen, D.A.; McKenzie, T.L.; Sehgal, A.; Williamson, S.; Golinelli, D.; Lurie, N. Contribution of public parks to physical activity. Am. J. Public Health 2007, 97, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Kaczynski, A.T.; Potwarka, L.R.; Saelens, B.E. Association of park size, distance, and features with physical activity in neighborhood parks. Am. J. Public Health 2008, 98, 1451–1456. [Google Scholar] [CrossRef] [PubMed]
- Maslow, A.L.; Reed, J.A.; Price, A.E.; Hooker, S.P. Associations between sociodemographic characteristics and perceptions of the built environment with the frequency, type, and duration of physical activity among trail users. Prev. Chronic Dis. 2012, 9. [Google Scholar] [CrossRef]
- Han, B.; Cohen, D.; McKenzie, T.L. Quantifying the contribution of neighborhood parks to physical activity. Prev. Med. 2013, 57, 483–487. [Google Scholar] [CrossRef] [PubMed]
- Gomez, L.F.; Sarmiento, O.L.; Parra, D.C.; Schmid, T.L.; Pratt, M.; Jacoby, E.; Neiman, A.; Cervero, R.; Mosquera, J.; Rutt, C.; et al. Characteristics of the built environment associated with leisure-time physical activity among adults in Bogota, Colombia: A multilevel study. J. Phys. Act. Health 2010, 7, S196–S203. [Google Scholar] [PubMed]
- Booth, M.L.; Owen, N.; Bauman, A.; Clavisi, O.; Leslie, E. Social-cognitive and perceived environment influences associated with physical activity in older Australians. Prev. Med. 2000, 31, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Beenackers, M.A.; Kamphuis, C.B.M.; Mackenbach, J.P.; Burdorf, A.; van Lenthe, F.J. Why some walk and others don‘t: Exploring interactions of perceived safety and social neighborhood factors with psychosocial cognitions. Health Educ. Res. 2013, 28, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Foster, S.; Giles-Corti, B. The built environment, neighborhood crime and constrained physical activity: An exploration of inconsistent findings. Prev. Med. 2008, 47, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Carnegie, M.A.; Bauman, A.; Marshall, A.L.; Mohsin, M.; Westley-Wise, V.; Booth, M.L. Perceptions of the physical environment, stage of change for physical activity, and walking among Australian adults. Res. Quart. Exerc. Sport 2002, 73, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Block, R.; Roux, A.V.D.; McGinn, A.P.; Wen, F.; Rodríguez, D.A. Associations of adult physical activity with perceived safety and police-recorded crime: The Multi-Ethnic Study of Atherosclerosis. Int. J. Behav. Nutr. Phys. Act. 2012, 9. [Google Scholar] [CrossRef] [PubMed]
- Center for Community Health Improvement. Healthy Chelsea. Available online: http://www.massgeneral.org/cchi/services/treatmentprograms.aspx?id=1501 (accessed on 8 November 2015).
- MassCHIP. Massachusetts Community Health Information Profile. Available online: http://www.mass.gov/eohhs/docs/dph/masschip/healthy-people/a-g/healthypeople2010cdcity-townchelsea.rtf (accessed on 2 November 2013).
- Chelsea. Chelsea Parks. Available online: http://www.ci.chelsea.ma.us/Public_Documents/ChelseaMA_Parks/index (accessed on 15 October 2014).
- WalkScore. Cities in Massachusetts. Available online: https://www.walkscore.com/MA/ (accessed on 9 November 2015).
- Federal Bureau of Investigation. Uniform Crime Reporting Statistics. Available online: http://www.fbi.gov/about-us/cjis/ucr/crime-in-the-u.s/2012/crime-in-the-u.s.2012/tables/5tabledatadecpdf (accessed on 11 December 2013).
- Staff, C.R. About gangs. Chelsesa Record—Chelsea Massachusetts Newspaper, 19 July 2012. [Google Scholar]
- Chelsea STAR. Chelsea STAR: Science to Achieve Results. Available online: http://www.chelseastar.org/ (accessed on 10 March 2015).
- Richters, J.E.; Martinez, P. The NIMH community violence project: I. Children as victims of and witnesses to violence. Psychiatry 1993, 56, 7–21. [Google Scholar] [PubMed]
- Wright, R.J.; Mitchell, H.; Visness, C.M.; Cohen, S.; Stout, J.; Evans, R.; Gold, D.R. Community violence and asthma morbidity: The Inner-City Asthma Study. Am. J. Public Health 2004, 94, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention. Environmental assessments. Available online: http://www.cdc.gov/ncipc/pub-res/pdf/YV/CDC_YV_SecIV.pdf?q=assessments (accessed on 20 February 2012).
- Lovasi, G.S.; Underhill, L.J.; Jack, D.; Richards, C.; Weiss, C.; Rundle, A. At odds: Concerns raised by using odds ratios for continuous or common dichotomous outcomes in research on physical activity and obesity. Open Epidemiol. J. 2012, 5, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Hastie, T.; Tibshirani, R.; Friedman, J. The Elements of Statistical Learning: Data Mining, Inference, and Prediction; Springer: New York, NY, USA, 2009; Volume 2. [Google Scholar]
- Poole, C. Low P-values or narrow confidence intervals: Which are more durable? Epidemiology 2001, 12, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Masschusetts Department of Public Health. BRFSS Special Reports: Risk Factors and Health Behaviors for Boston. Available online: http://www.mass.gov/eohhs/docs/dph/masschip/brfss-rf/brfssrfchnachna19.rtf (accessed on 18 November 2014).
- Coutts, C.; Chapin, T.; Horner, M.; Taylor, C. County-level effects of green space access on physical activity. J. Phys. Act. Health 2013, 10, 232–240. [Google Scholar] [PubMed]
- Coulton, C.J.; Korbin, J.; Chan, T.; Su, M. Mapping residents‘ perceptions of neighborhood boundaries: A methodological note. Am. J. Community Psychol. 2001, 29, 371–383. [Google Scholar] [CrossRef] [PubMed]
- Wilbur, J.; Chandler, P.J.; Dancy, B.; Lee, H. Correlates of physical activity in urban midwestern Latinas. Am. J. Prev. Med. 2003, 25, 69–76. [Google Scholar] [CrossRef]
- De Assis, M.A.; de Mello, M.F.; Scorza, F.A.; Cadrobbi, M.P.; Schooedl, A.F.; da Silva, S.G.; de Albuquerque, M.; da Silva, A.C.; Arida, R.M. Evaluation of physical activity habits in patients with posttraumatic stress disorder. Clinics 2008, 63, 473–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilhelm, S.; Sonja, A.; Schneider, I.E.; Chavez, D.J.; Shinew, K.J. Visitor constraints to physical activity in park and recreation areas: Differences by race and ethnicity. J. Park Recreat. Adm. 2009, 27, 78–95. [Google Scholar]
- Hillsdon, M.; Panter, J.; Foster, C.; Jones, A. The relationship between access and quality of urban green space with population physical activity. Public Health 2006, 120, 1127–1132. [Google Scholar] [CrossRef] [PubMed]
- Dai, D. Racial/ethnic and socioeconomic disparities in urban green space accessibility: Where to intervene? Landsc. Urban Plan. 2011, 102, 234–244. [Google Scholar] [CrossRef]
- Census. State & County Quickfacts, Chelsea (City), Massachusetts. Available online: http://quickfacts.census.gov/qfd/states/25/2513205.html (accessed on 15 January 2014).
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ou, J.Y.; Levy, J.I.; Peters, J.L.; Bongiovanni, R.; Garcia-Soto, J.; Medina, R.; Scammell, M.K. A Walk in the Park: The Influence of Urban Parks and Community Violence on Physical Activity in Chelsea, MA. Int. J. Environ. Res. Public Health 2016, 13, 97. https://doi.org/10.3390/ijerph13010097
Ou JY, Levy JI, Peters JL, Bongiovanni R, Garcia-Soto J, Medina R, Scammell MK. A Walk in the Park: The Influence of Urban Parks and Community Violence on Physical Activity in Chelsea, MA. International Journal of Environmental Research and Public Health. 2016; 13(1):97. https://doi.org/10.3390/ijerph13010097
Chicago/Turabian StyleOu, Judy Y., Jonathan I. Levy, Junenette L. Peters, Roseann Bongiovanni, Jovanna Garcia-Soto, Rafael Medina, and Madeleine K. Scammell. 2016. "A Walk in the Park: The Influence of Urban Parks and Community Violence on Physical Activity in Chelsea, MA" International Journal of Environmental Research and Public Health 13, no. 1: 97. https://doi.org/10.3390/ijerph13010097
APA StyleOu, J. Y., Levy, J. I., Peters, J. L., Bongiovanni, R., Garcia-Soto, J., Medina, R., & Scammell, M. K. (2016). A Walk in the Park: The Influence of Urban Parks and Community Violence on Physical Activity in Chelsea, MA. International Journal of Environmental Research and Public Health, 13(1), 97. https://doi.org/10.3390/ijerph13010097