
Geographical and Temporal Variations in Female Breast Cancer Mortality in the Municipalities of Andalusia (Southern Spain)

Abstract
:1. Introduction
2. Materials and Methods
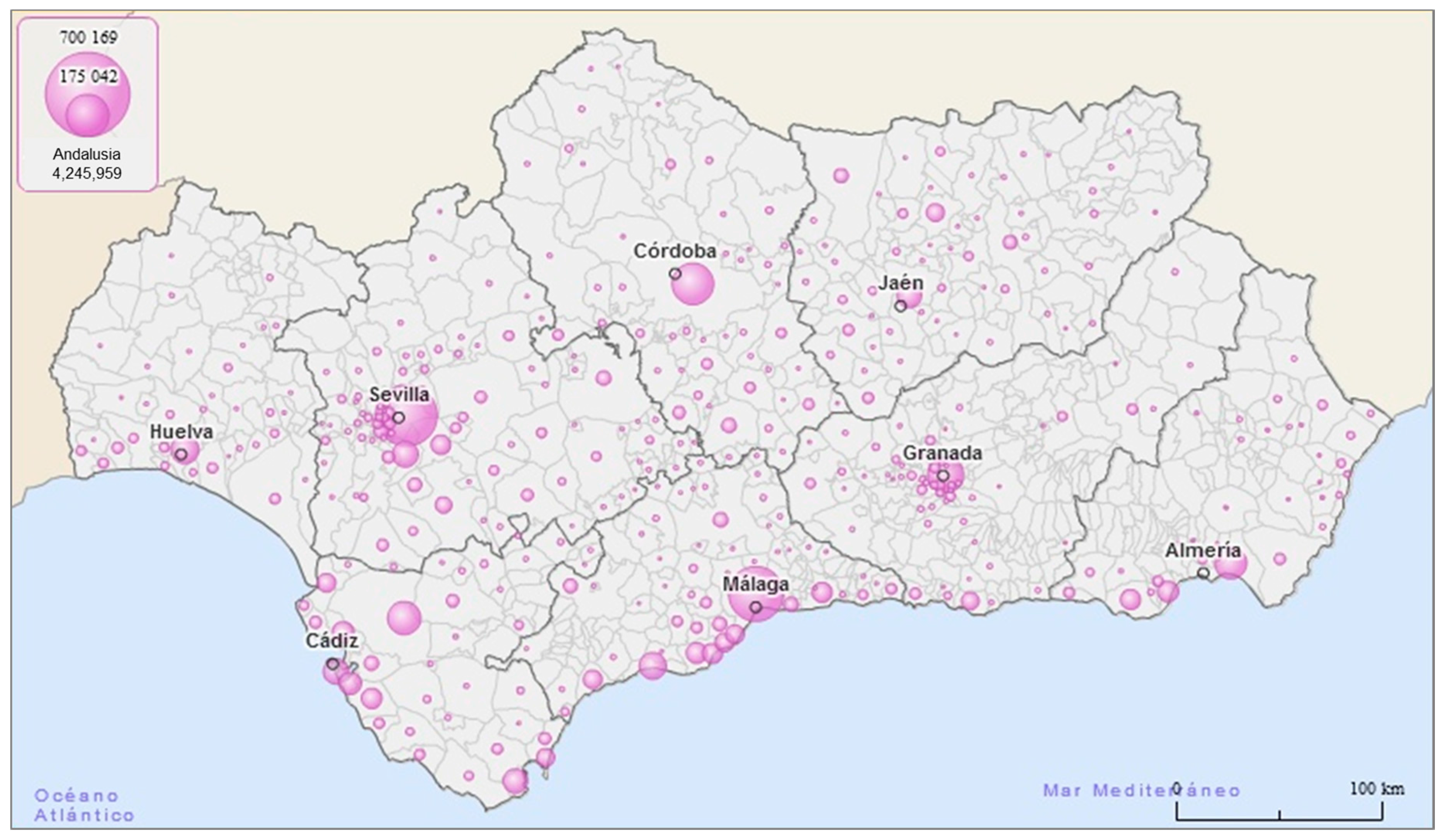
2.1. Epidemiological Design and Scope
2.2. Variables
- Mortality: Number of deaths from female breast cancer recorded in each municipality for each year and age group (International Classification of Diseases (ICD)-9 174 and ICD-10 C50).
- Population: Number of women living in each municipality for each year and age group.
- Spanish mortality rate: Number of deaths from female breast cancer per 10,000 women in Spain for each year and age group.
2.3. Sources of Information
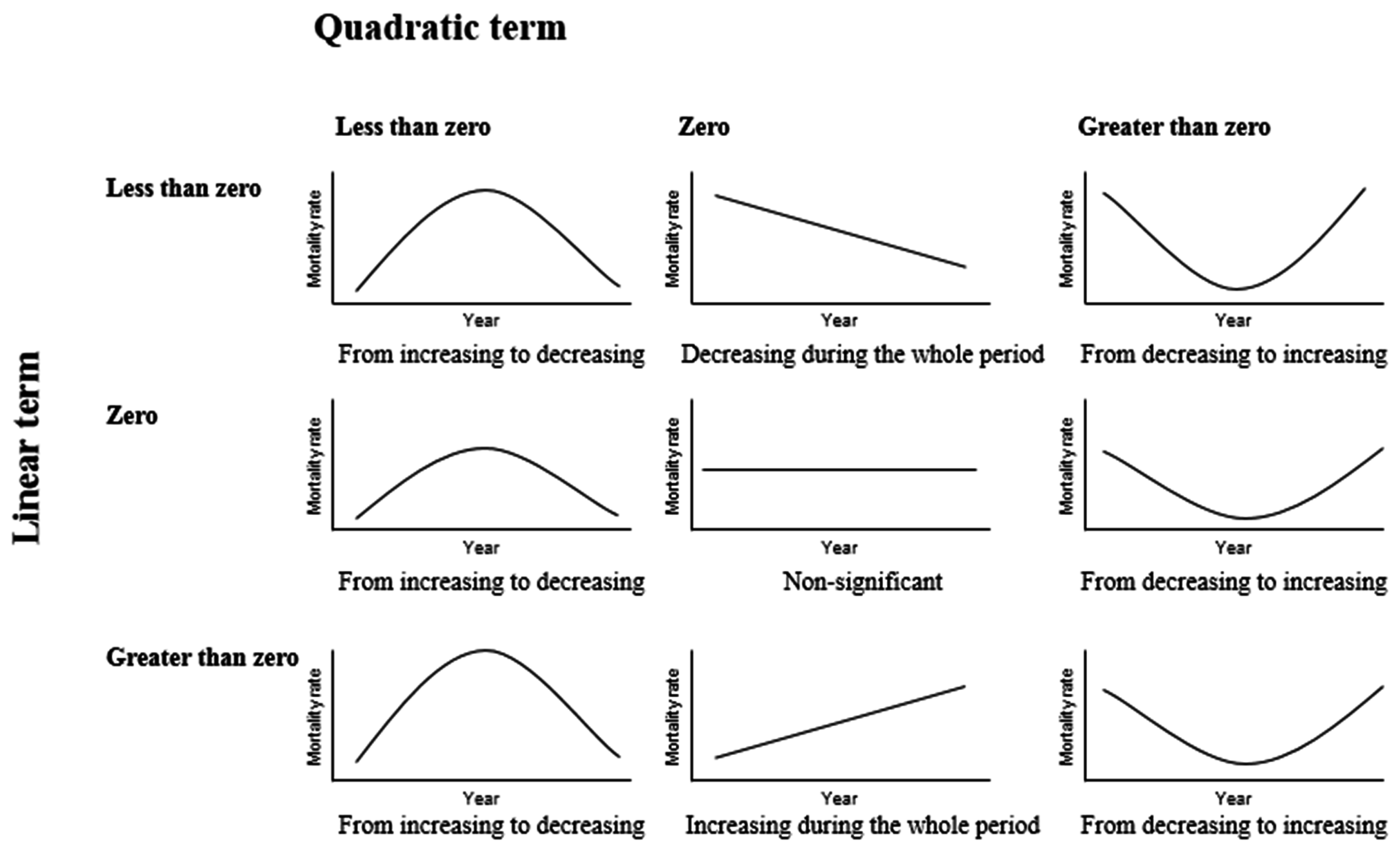
2.4. Statistical Data Analysis
3. Results
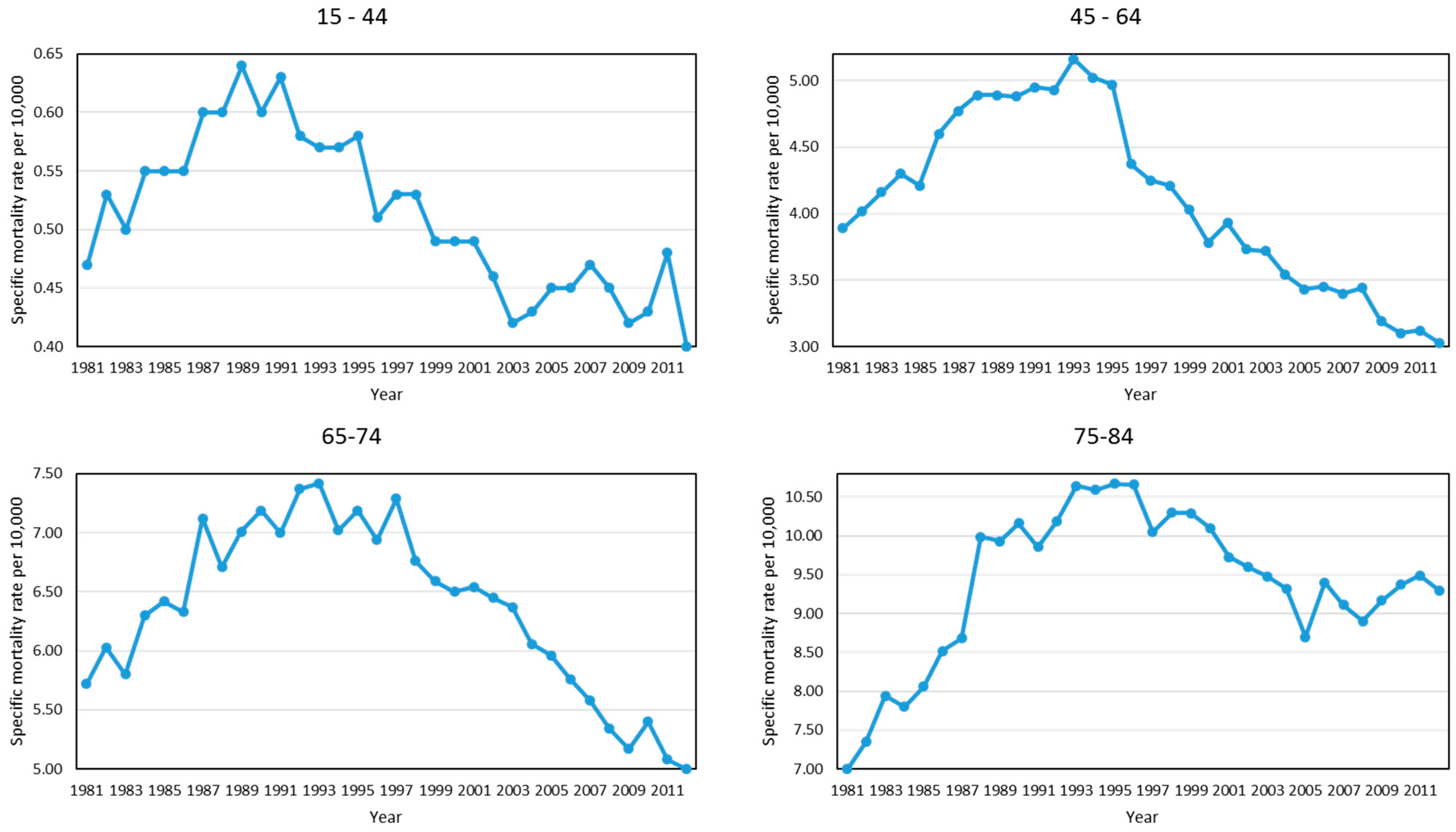
3.1. Trend of the Age-Specific Mortality Rate in the Municipalities of Andalusia, 1981–2012
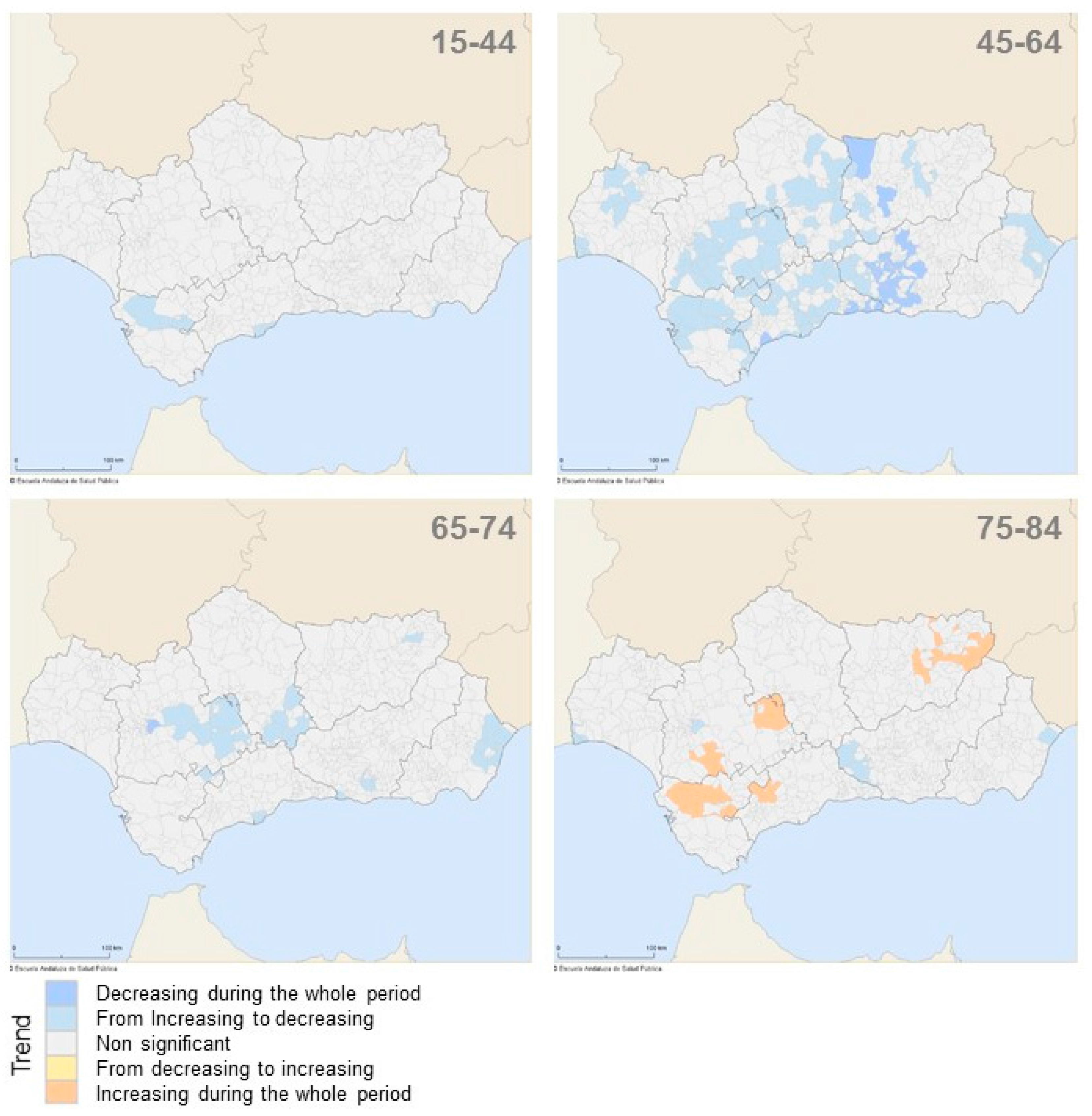
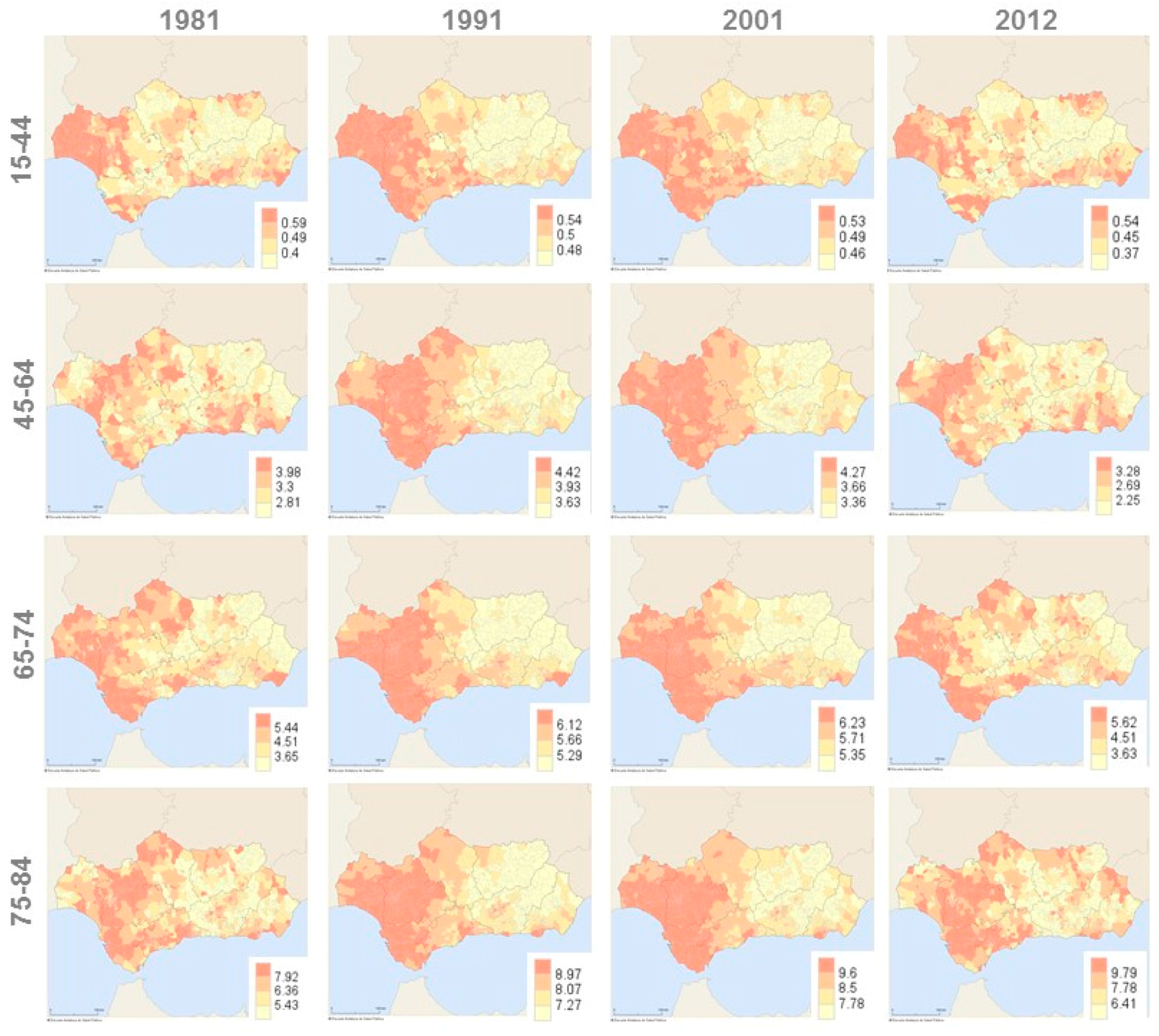
3.2. Geographical Variation of the Age-Specific Mortality Rate in the Municipalities of Andalusia, 1981–2012
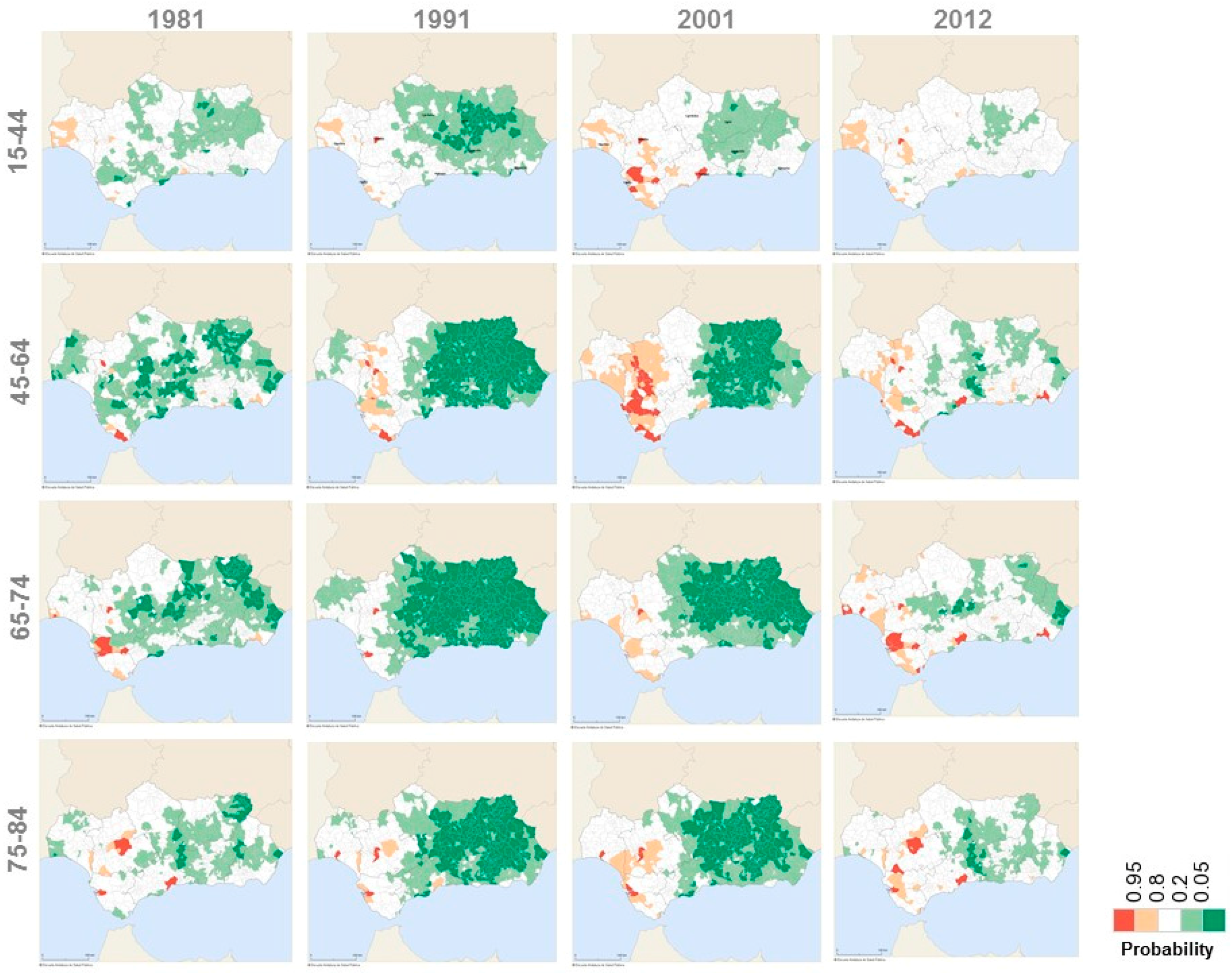
3.3. Geographical Variation of the Age-Specific Mortality Rate Ratio in the Municipalities of Andalusia, 1981–2012
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.W.; Comber, H.; Forman, D.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer 2013, 49, 1374–1403. [Google Scholar] [CrossRef] [PubMed]
- Malvezzi, M.; Bertuccio, P.; Levi, F.; La Vecchia, C.; Negri, E. European cancer mortality predictions for the year 2012. Ann. Oncol. 2012, 23, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Estadistica (INE). Spain in Figures 2016; INE: Madrid, Spain, 2016. [Google Scholar]
- Ugarte, M.D.; Goicoa, T.; Etxeberria, J.; Militino, A.F.; Pollán, M. Age-specific spatio-temporal patterns of female breast cancer mortality in Spain (1975–2005). Ann. Epidemiol. 2010, 20, 906–916. [Google Scholar] [CrossRef] [PubMed]
- Kanaroglou, P.; Delmelle, E.; Páez, A. Spatial Analysis in Health Geography; Routledge: New York, NY, USA, 2015. [Google Scholar]
- Banerjee, S.; Carlin, B.P.; Gelfand, A.E. Hierarchical Modeling and Analysis for Spatial Data, 2nd ed.; Chapman & Hall/CRC: Boca Raton, FL, USA, 2014. [Google Scholar]
- Ocaña-Riola, R. Common errors in disease mapping. Geospat. Health 2010, 4, 139–154. [Google Scholar] [CrossRef] [PubMed]
- Gelman, A.; Carlin, J.B.; Stern, H.S.; Dunson, D.B.; Vehtari, A.; Rubin, D.B. Bayesian Data Analysis, 3th ed.; Chapman & Hall/CRC: Boca Raton, FL, USA, 2013. [Google Scholar]
- La Vecchia, C.; Levi, F.; Lucchini, F.; Negri, E. Trends in mortality from major diseases in Europe, 1980–1993. Eur. J. Epidemiol. 1998, 14, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Spiegelhalter, D.J.; Best, N.G.; Carlin, B.P.; van der Linde, A. Bayesian measures of model complexity and fit (with discussion). J. R. Stat. Soc. B 2002, 64, 583–640. [Google Scholar] [CrossRef]
- Bernardinelli, L.; Clayton, D.G.; Pascutto, C.; Montomoli, C.; Ghislandi, M.; Songini, M. Bayesian analysis of space-time variation in disease risk. Stat. Med. 1995, 14, 2433–2443. [Google Scholar] [CrossRef] [PubMed]
- Bithell, J.F. A classification of disease mapping methods. Stat. Med. 2000, 19, 2203–2215. [Google Scholar] [CrossRef]
- Brooks, S.P.; Gelman, A. Alternative methods for monitoring convergence of iterative simulations. J. Comput. Graph. Stat. 1998, 7, 434–455. [Google Scholar]
- Lawson, A.B.; Browne, W.J.; Vidal Rodeiro, C.L. Disease Mapping with WinBUGS and MlwiN; John Wiley & Sons: Chichester, UK, 2003. [Google Scholar]
- Richardson, S.; Thomson, A.; Best, N.; Elliot, P. Interpreting posterior relative risk estimates in disease mapping studies. Environ. Health Perspect. 2004, 112, 1016–1025. [Google Scholar] [CrossRef] [PubMed]
- Martín-Sánchez, J.C.; Clèries, R.; Lidón, C.; González-de Paz, L.; Lunet, N.; Martínez-Sánchez, J.M. Bayesian prediction of lung and breast cancer mortality among women in Spain (2014–2020). Cancer Epidemiol. 2016, 43, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Salmerón, D.; Cirera, L.; Saez, M.; Navarro, C. Influence of the introduction of the ICD-10 on tendencies of mortality by causes (1980–2004). Gac. Sanit. 2009, 23, 144–146. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, M.C.; Villar, F. Cribado Poblacional de Cáncer de Mama en España; Ministerio de Sanidad y Consumo: Madrid, Spain, 1998. [Google Scholar]
- Escuela Andaluza de Salud Pública (EASP); Servicio Andaluz de Salud (SAS). Resultados y Calidad del Sistema Sanitario Público de Andalucía; EASP: Granada, Spain, 2012. [Google Scholar]
- Lee, S.J.; Boscardin, W.J.; Stijacic-Cenzer, I.; Conell-Price, J.; O’Brien, S.; Walter, L.C. Time lag to benefit after screening for breast and colorectal cancer: Meta-analysis of survival data from the United States, Sweden, United Kingdom, and Denmark. BMJ 2012, 345, e8441. [Google Scholar] [CrossRef] [PubMed]
- Ocaña-Riola, R.; Mayoral-Cortés, J.M.; Navarro-Moreno, E. Age–period–cohort effect on female breast cancer mortality in Southern Spain. Med. Oncol. 2013, 30, 671. [Google Scholar] [CrossRef] [PubMed]
- Instituto de Salud Carlos III (ISCIII). Ariadna: Mortalidad por Cáncer y Otras Causas; ISCIII: Madrid, Spain, 2016; Available online: http://ariadna.cne.isciii.es (accessed on 29 July 2016).
- Mina, L.A.; Storniolo, A.M.; Kipfer, H.D.; Hunter, C.; Ludwig, K.K. Breast Cancer Prevention and Treatment; Springer: Basel, Switzerland, 2016. [Google Scholar]
- National Cancer Institute. PDQ® Breast Cancer Treatment: Health Professional Version; National Cancer Institute: Bethesda, MD, USA, 2013. [Google Scholar]
- Lundqvist, A.; Andersson, E.; Ahlberg, I.; Nilbert, M.; Gerdtham, U. Socioeconomic inequalities in breast cancer incidence and mortality in Europe: A systematic review and meta-analysis. Eur. J. Public Health 2016, 26, 804–813. [Google Scholar] [CrossRef] [PubMed]
- Herrero, C.; Soler, A.; Villar, A. Desarrollo Humano en España 1980–2007; Ivie: Valencia, Spain, 2010. [Google Scholar]
- Wakefield, J.; Shaddick, G. Health-exposure modelling and the ecological fallacy. Biostatistics 2006, 7, 438–455. [Google Scholar] [CrossRef] [PubMed]
- Ocaña-Riola, R.; Fernández, A.; Mayoral, J.M.; Toro, S.; Sánchez-Cantalejo, C. Uncontrolled migrations as a cause of inequality in health and mortality in small area studies. Epidemiology 2009, 20, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Ocaña-Riola, R.; Mayoral-Cortés, J.M. Spatio-temporal trends of mortality in small-areas of Southern Spain. BMC Public Health 2010, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Ocaña-Riola, R.; Mayoral, J.M.; Sánchez-Cantalejo, C.; Toro, S.; Fernández, A.; Méndez, C. Interactive Mortality Atlas in Andalusia, Spain (AIMA). Rev. Esp. Salud Pública 2008, 82, 379–394. [Google Scholar] [CrossRef] [PubMed]
- DEMAP. Available online: www.demap.es (accessed on 18 November 2016).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Specific Mortality Rate | Specific Mortality Rate Ratio | |
|---|---|---|
| Distribution | ~ | ~ |
| Mean | ||
| Model | ||
| Constant terms | ~flat, ~, ~ | |
| Temporal random structure | ||
| Structured effect | ~, , a = 1, 2 | |
| Hyperparameter | ~, a = 1, 2 | |
| Spatial random structure | ||
| Structured effect | ~, | |
| Non-structured effect | ~ | |
| Hyperparameters | ~ ~ | |
| Notation | : deaths within age subgroup i in municipality m at time t | : population within age subgroup i in municipality m at time t |
| : specific mortality rate in municipality m at time t | : specific mortality rate in Spain at time t | |
| : Median year | : specific rate ratio of municipality m compared with Spain at time t | |
| : adjacency matrix ( if m and n are neighbour areas and otherwise) | ||
| Age Group | 15–44 | 45–64 | ||||||||
| Year | 1981 | 1991 | 2001 | 2012 | 1981–2012 | 1981 | 1991 | 2001 | 2012 | 1981–2012 |
| Deaths from female breast cancer | 71 | 106 | 102 | 79 | 2677 | 268 | 348 | 340 | 319 | 9998 |
| Female population | 1,301,212 | 1,552,496 | 1,727,353 | 1,771,291 | 52,076,904 | 673,832 | 716,606 | 761,630 | 1,050,092 | 25,077,188 |
| Age-specific mortality rate per 10,000 | 0.55 | 0.68 | 0.59 | 0.45 | 0.51 | 3.98 | 4.86 | 4.46 | 3.04 | 3.99 |
| Age group | 65–74 | 75–84 | ||||||||
| Year | 1981 | 1991 | 2001 | 2012 | 1981–2012 | 1981 | 1991 | 2001 | 2012 | 1981–2012 |
| Deaths from female breast cancer | 159 | 190 | 262 | 197 | 5900 | 105 | 159 | 205 | 271 | 5625 |
| Female population | 238,227 | 272,957 | 342,834 | 347,981 | 9,672,430 | 124,954 | 162,496 | 200,940 | 281,236 | 6,129,090 |
| Age-specific mortality rate per 10,000 | 6.67 | 6.96 | 7.64 | 5.66 | 6.10 | 8.40 | 9.78 | 10.20 | 9.64 | 9.18 |
| A | 15–44 | 45–64 | 65–74 | 75–84 | ||||||||||||
| Age-specific mortality trend | Municipalities | Percentage | Municipalities | Percentage | Municipalities | Percentage | Municipalities | Percentage | ||||||||
| Decreasing during the whole period | 0 | 0.0% | 39 | 5.0% | 1 | 0.1% | 0 | 0.0% | ||||||||
| From increasing to decreasing | 7 | 0.9% | 93 | 12.1% | 29 | 3.8% | 6 | 0.8% | ||||||||
| Non-significant | 764 | 99.1% | 639 | 82.9% | 741 | 96.1% | 755 | 97.9% | ||||||||
| From decreasing to increasing | 0 | 0.0% | 0 | 0.0% | 0 | 0.0% | 0 | 0.0% | ||||||||
| Increasing during the whole period | 0 | 0.0% | 0 | 0.0% | 0 | 0.0% | 10 | 1.3% | ||||||||
| B | 15–44 | 45–64 | 65–74 | 75–84 | ||||||||||||
| Age-specific mortality rate per 104 | 1981 | 1991 | 2001 | 2012 | 1981 | 1991 | 2001 | 2012 | 1981 | 1991 | 2001 | 2012 | 1981 | 1991 | 2001 | 2012 |
| Maximum | 2.71 | 0.72 | 0.68 | 2.58 | 8.35 | 5.72 | 5.63 | 8.54 | 13.76 | 8.46 | 7.92 | 13.73 | 18.43 | 12.67 | 13.76 | 26.20 |
| Percentile 75 | 0.59 | 0.54 | 0.53 | 0.54 | 3.98 | 4.42 | 4.27 | 3.28 | 5.44 | 6.12 | 6.23 | 5.62 | 7.92 | 8.97 | 9.60 | 9.79 |
| Percentile 50 | 0.49 | 0.50 | 0.49 | 0.45 | 3.30 | 3.93 | 3.66 | 2.69 | 4.51 | 5.66 | 5.71 | 4.51 | 6.36 | 8.07 | 8.50 | 7.78 |
| Percentile 25 | 0.40 | 0.48 | 0.46 | 0.37 | 2.81 | 3.63 | 3.36 | 2.25 | 3.65 | 5.29 | 5.35 | 3.63 | 5.43 | 7.27 | 7.78 | 6.41 |
| Minimum | 0.19 | 0.42 | 0.40 | 0.19 | 1.54 | 2.96 | 2.91 | 1.23 | 1.96 | 4.08 | 4.44 | 1.70 | 3.16 | 5.87 | 6.78 | 3.43 |
| Interquartile range | 0.19 | 0.06 | 0.07 | 0.17 | 1.17 | 0.79 | 0.91 | 1.03 | 1.89 | 0.83 | 0.88 | 1.99 | 2.49 | 1.70 | 1.82 | 3.38 |
| Spanish age-specific mortality rate | 0.47 | 0.63 | 0.49 | 0.40 | 3.89 | 4.95 | 3.93 | 3.03 | 5.72 | 7.00 | 6.54 | 5.00 | 7.00 | 9.86 | 9.73 | 9.30 |
| C | 15–44 | 45–64 | 65–74 | 75–84 | ||||||||||||
| Age-specific mortality rates ratio | 1981 | 1991 | 2001 | 2012 | 1981 | 1991 | 2001 | 2012 | 1981 | 1991 | 2001 | 2012 | 1981 | 1991 | 2001 | 2012 |
| Significantly higher than 1 | ||||||||||||||||
| Number of municipalities | 0 | 1 | 5 | 2 | 2 | 4 | 20 | 9 | 4 | 2 | 1 | 12 | 4 | 5 | 5 | 5 |
| Percentage | 0.0% | 0.1% | 0.6% | 0.3% | 0.3% | 0.5% | 2.6% | 1.2% | 0.5% | 0.3% | 0.1% | 1.6% | 0.5% | 0.6% | 0.6% | 0.6% |
| Not significantly different from 1 | ||||||||||||||||
| Number of municipalities | 760 | 715 | 763 | 768 | 704 | 458 | 632 | 754 | 711 | 392 | 557 | 745 | 750 | 533 | 576 | 758 |
| Percentage | 98.6% | 92.8% | 99.0% | 99.6% | 91.3% | 59.4% | 82.0% | 97.8% | 92.2% | 50.8% | 72.3% | 96.6% | 97.3% | 69.2% | 74.8% | 98.4% |
| Significantly lower than 1 | ||||||||||||||||
| Number of municipalities | 11 | 55 | 3 | 1 | 65 | 309 | 119 | 8 | 56 | 377 | 213 | 14 | 17 | 233 | 190 | 8 |
| Percentage | 1.4% | 7.1% | 0.4% | 0.1% | 8.4% | 40.1% | 15.4% | 1.0% | 7.3% | 48.9% | 27.6% | 1.8% | 2.2% | 30.2% | 24.6% | 1.0% |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ocaña-Riola, R.; Montaño-Remacha, C.; Mayoral-Cortés, J.M. Geographical and Temporal Variations in Female Breast Cancer Mortality in the Municipalities of Andalusia (Southern Spain). Int. J. Environ. Res. Public Health 2016, 13, 1162. https://doi.org/10.3390/ijerph13111162
Ocaña-Riola R, Montaño-Remacha C, Mayoral-Cortés JM. Geographical and Temporal Variations in Female Breast Cancer Mortality in the Municipalities of Andalusia (Southern Spain). International Journal of Environmental Research and Public Health. 2016; 13(11):1162. https://doi.org/10.3390/ijerph13111162
Chicago/Turabian StyleOcaña-Riola, Ricardo, Carmen Montaño-Remacha, and José María Mayoral-Cortés. 2016. "Geographical and Temporal Variations in Female Breast Cancer Mortality in the Municipalities of Andalusia (Southern Spain)" International Journal of Environmental Research and Public Health 13, no. 11: 1162. https://doi.org/10.3390/ijerph13111162
APA StyleOcaña-Riola, R., Montaño-Remacha, C., & Mayoral-Cortés, J. M. (2016). Geographical and Temporal Variations in Female Breast Cancer Mortality in the Municipalities of Andalusia (Southern Spain). International Journal of Environmental Research and Public Health, 13(11), 1162. https://doi.org/10.3390/ijerph13111162