
Estimation of Saliva Cotinine Cut-Off Points for Active and Passive Smoking during Pregnancy—Polish Mother and Child Cohort (REPRO_PL)

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Questionnaire Data
2.3. Saliva Collection and a Cotinine Concentration Assessment
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Self-Reported Active and Passive Smoking Status
3.3. Cotinine Concentrations
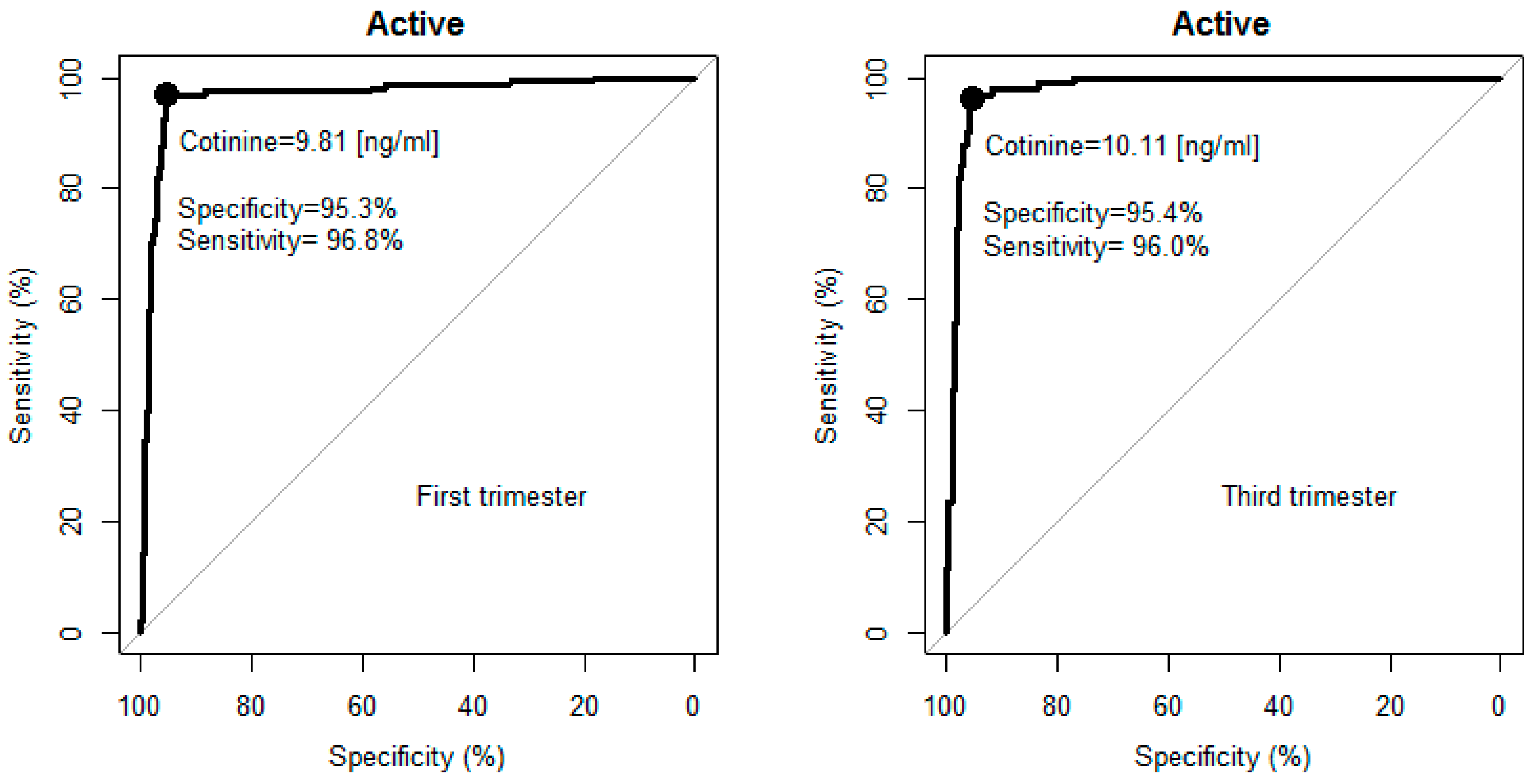
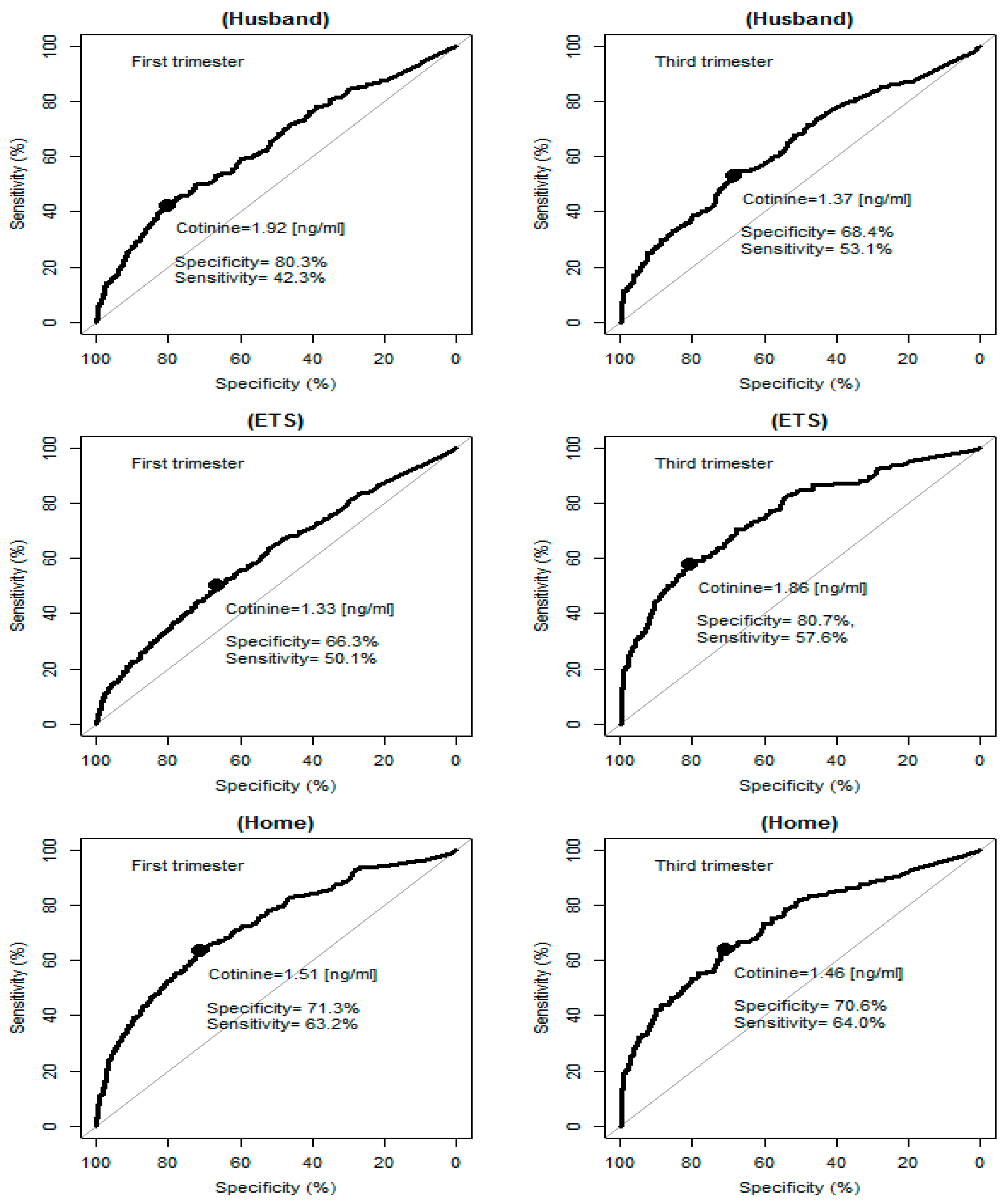
3.4. Determination of Cotinine Cut-Off
3.5. Cotinine Cut-Off and Self-Reported Smoking and Passive Smoking Status
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Surgeon General’s Report: The Health Consequences of Smoking—50 Years of Progress. Available online: http://www.surgeongeneral.gov/library/reports/50-years-of-progress/full-report.pdf (accessed on 1 September 2016).
- SRNT Subcommittee on Biochemical Verification. Biochemical verification of tobacco use and cessation. Nicotine Tob. Res. 2002, 4, 149–159. [Google Scholar]
- Benowitz, N.L. Biomarkers of environmental tobacco smoke exposure. Environ. Health Perspect. 1999, 107, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Kvalvik, L.G.; Nilsen, R.M.; Skjærven, R.; Vollset, S.E.; Midttun, Ø.; Ueland, P.M.; Haug, K. Self-reported smoking status and plasma cotinine concentrations among pregnant women in the Norwegian Mother and Child Cohort Study. Pediatr. Res. 2012, 72, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L.; Bernert, J.T.; Caraballo, R.S.; Holiday, D.B.; Wang, J. Optimal serum cotinine levels for distinguishing cigarette smokers and nonsmokers within different racial/ethnic groups in the United States between 1999 and 2004. Am. J. Epidemiol. 2009, 169, 236–348. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L. Cotinine as a biomarker of environmental tobacco smoke exposure. Epidemiol. Rev. 1996, 18, 188–204. [Google Scholar] [CrossRef] [PubMed]
- Florescu, A.; Ferrence, R.; Einarson, T.; Selby, P.; Soldin, O.; Koren, G. Methods for quantification of exposure to cigarette smoking and environmental tobacco smoke: Focus on developmental toxicology. Ther. Drug Monit. 2009, 31, 14–30. [Google Scholar] [CrossRef] [PubMed]
- Avila-Tang, E.; Al-Delaimy, W.K.; Ashley, D.L.; Benowitz, N.; Bernert, J.T.; Kim, S.; Samet, J.M.; Hecht, S.S. Assessing secondhand smoke using biological markers. Tob. Control 2013, 22, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Stragierowicz, J.; Mikolajewska, K.; Zawadzka-Stolarz, M.; Polanska, K.; Ligocka, D. Estimation of Cutoff Values of Cotinine in Urine and Saliva for Pregnant Women in Poland. BioMed Res. Int. 2013, 2013, 386784. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L.; Jacob, P., 3rd. Metabolism of nicotine to cotinine studied by a dual stable isotope method. Clin. Pharmacol. Ther. 1994, 56, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.J.; Robinson, R.F.; Khan, B.A.; Sosnoff, C.S.; Dillard, D.A. Estimating cotinine associations and a saliva cotinine level to identify active cigarette smoking in Alaska native pregnant women. Matern. Child Health J. 2014, 18, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, M.J.; Tunstall-Pedoe, H.; Feyerabend, C.; Vesey, C.; Salloojee, Y. Comparison of tests used to distinguish smokers from nonsmokers. Am. J. Public Health 1987, 77, 1435–1438. [Google Scholar] [CrossRef] [PubMed]
- Etzel, R.A. A review of the use of saliva cotinine as a marker of tobacco smoke exposure. Prev. Med. 1990, 19, 190–197. [Google Scholar] [CrossRef]
- Boyd, N.R.; Windsor, R.A.; Perkins, L.L.; Lowe, J.B. Quality of measurement of smoking status by self-report and saliva cotinine among pregnant women. Matern. Child Health J. 1998, 2, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Hegaard, H.K.; Kjaergaard, H.; Møller, L.F.; Wachmann, H.; Ottesen, B. Determination of a saliva cotinine cut-off to distinguish pregnant smokers from pregnant non-smokers. Acta Obstet. Gynecol. Scand. 2007, 86, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, M.; Yokoi, T. Interindividual variability in nicotine metabolism: C-oxidation and glucuronidation. Drug Metab. Pharmacokinet. 2005, 20, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, E.; Benowitz, N.; Cargill, A.; Jacob, R.; Hinks, L.; Day, I.; Murphy, M.; Walton, R. Determinants of the rate of nicotine metabolism and effects on smoking behavior. Clin. Pharmacol. Ther. 2006, 80, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, D.; Jacob, P., 3rd; Benowitz, N.L. Accelerated metabolism of nicotine and cotinine in pregnant smokers. J. Pharmacol. Exp. Ther. 2002, 301, 594–598. [Google Scholar] [CrossRef] [PubMed]
- Rebagliato, M.; Bolumar, F.; Florey Cdu, V.; Jarvis, M.J.; Pérez-Hoyos, S.; Hernández-Aguado, I.; Aviñó, M.J. Variations in cotinine levels in smokers during and after pregnancy. Am. J. Obstet. Gynecol. 1998, 178, 568–571. [Google Scholar] [CrossRef]
- Sasaki, S.; Braimoh, T.S.; Yila, T.A.; Yoshioka, E.; Kishi, R. Self-reported tobacco smoke exposure and plasma cotinine levels during pregnancy—A validation study in Northern Japan. Sci. Total Environ. 2011, 412–413, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Zielińska-Danch, W.; Wardas, W.; Sobczak, A.; Szołtysek-Bołdys, I. Estimation of urinary cotinine cut-off points distinguishing non-smokers, passive and active smokers. Biomarkers 2007, 12, 484–496. [Google Scholar] [CrossRef] [PubMed]
- Rebagliato, M.; Bolumar, F.; Florey Cdu, V. Assessment of exposure to environmental tobacco smoke in nonsmoking pregnant women in different environments of daily living. Am. J. Epidemiol. 1995, 142, 525–530. [Google Scholar] [PubMed]
- Kaufman, F.L.; Kharrazi, M.; Delorenze, G.N.; Eskenazi, B.; Bernert, J.T. Estimation of environmental tobacco smoke exposure during pregnancy using a single question on household smokers versus serum cotinine. J. Expo. Anal. Environ. Epidemiol. 2002, 12, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Polanska, K.; Hanke, W.; Gromadzinska, J.; Ligocka, D.; Gulczynska, E.; Sobala, W.; Wasowicz, W. Polish mother and child cohort study—Defining the problem, the aim of the study and methodological assumption. Int. J. Occup. Med. Environ. Health 2009, 22, 383–391. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, 2016. Available online: https://www.R-project.org/ (accessed on 11 August 2016).
- Lopez-Raton, M.; Rodriguez-Alvarez, M.X.; Cadarso-Suarez, C.; Gude-Sampedro, F. OptimalCutpoints: An R Package for Selecting Optimal Cutpoints in Diagnostic Tests. J. Stat. Softw. 2014, 61, 1–36. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Mullen, P.D.; Carbonari, J.P.; Tabak, E.R.; Glenday, M.C. Improving disclosure of smoking by pregnant women. Am. J. Obstet. Gynecol. 1991, 165, 409–413. [Google Scholar] [CrossRef]
- World Health Organization. Global Adult Tobacco Survey (GATS). Available online: http://www.who.int/tobacco/surveillance/en_tfi_gats_poland_report_2010.pdf (accessed on 9 September 2016).
- Goniewicz, M.L.; Zielinska-Danch, W. Electronic Cigarette Use among Teenagers and Young Adults in Poland. Pediatrics 2012, 130, e879–e885. [Google Scholar] [CrossRef] [PubMed]
- Coleman, T.; Chamberlain, C.; Davey, M.A.; Cooper, S.E.; Leonardi-Bee, J. Pharmacological interventions for promoting smoking cessation during pregnancy. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef]
- Coleman, T.; Chamberlain, C.; Davey, M.A.; Cooper, S.E.; Leonardi-Bee, J. Pharmacological interventions for promoting smoking cessation during pregnancy. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Wojtyła, A.; Gozdziewska, M.; Paprzycki, P.; Bilinski, P. Tobacco-related Foetal Origin of Adult Diseases Hypothesis—Population studies in Poland. Ann. Agric. Environ. Med. 2012, 19, 117–128. [Google Scholar] [PubMed]
- Balwicki, Ł.; Zarzeczna-Baran, M.; Wierucki, Ł.; Jędrzejczyk, T.; Strahl, M.; Wrotkowska, M.; Goniewicz, M.L.; Zdorjewski, T. Smoking among pregnant women in small towns in Poland. Int. J. Public Health 2016, 61, 111–118. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Tobacco Smoke Exposure * | n | Geometric Mean (ng/mL) | 95% CI (ng/mL) |
|---|---|---|---|
| Non-smokers | |||
| 1st trimester (n = 1505; missing = 231) | 1274 | 1.14 | 1.06–1.22 |
| 2nd trimester (n = 1356; missing = 554) | 802 | 1.10 | 1.01–2.00 |
| 3rd trimester (n = 1273; missing = 293) | 980 | 1.15 | 1.07–1.24 |
| Smokers | |||
| 1st trimester (n = 196; missing = 39) | 157 | 78.77 | 65.53–94.68 |
| 2nd trimester (n = 142; missing = 36) | 106 | 98.48 | 81.83–118.52 |
| 3rd trimester (n = 122; missing = 23) | 99 | 85.84 | 69.75–105.65 |
| Passive smokers ** | |||
| 1st trimester husband/partner smoking (n = 423; missing = 61) | 362 | 1.84 | 1.56–2.16 |
| 2nd trimester husband/partner smoking (n = 338; missing = 148) | 190 | 2.08 | 1.66–2.60 |
| 3rd trimester husband/partner smoking (n = 325; missing = 82) | 243 | 1.89 | 1.55–2.31 |
| 1st trimester ETS exposure (n = 614; missing = 99) | 515 | 1.55 | 1.36–1.76 |
| 2nd trimester ETS exposure (n = 236; missing = 106) | 130 | 3.24 a | 2.34–4.49 |
| 3rd trimester ETS exposure (n = 204; missing = 65) | 139 | 3.42 b | 2.57–4.56 |
| 1st trimester smoking allowed at home (n = 239; missing = 30) | 209 | 2.86 | 2.27–3.61 |
| 2nd trimester smoking allowed at home (n = 185; missing = 80) | 105 | 3.53 | 2.51–4.96 |
| 3rd trimester smoking allowed at home (n = 181; missing = 45) | 136 | 3.19 | 2.37–4.28 |
| Cotinine Concentrations * | 1st Trimester | 2nd Trimester | 3rd Trimester |
|---|---|---|---|
| 1st trimester | (1464) | 0.85 | 0.62 |
| 2nd trimester | (923) | (924) | 0.79 |
| 3rd trimester | (1039) | (863) | (1102) |
| Smoking Status * | Median | 95% CI |
|---|---|---|
| Active smoking | ||
| 1st trimester: optimal cut-off | 9.8 | 9.5–12.9 |
| 1st trimester: optimal sensitivity | 96.8 | 93.6–99.4 |
| 1st trimester: optimal specificity | 95.4 | 94.2–96.4 |
| 3rd trimester: optimal cut-off | 10.1 | 4.2–13.5 |
| 3rd trimester: optimal sensitivity | 97.0 | 92.9–100.0 |
| 3rd trimester: optimal specificity | 95.3 | 91.6–96.7 |
| Passive smoking | ||
| 1st trimester: optimal cut-off | 1.52 | 1.2–2.2 |
| 1st trimester: optimal sensitivity | 63.6 | 48.8–77.5 |
| 1st trimester: optimal specificity | 72.1 | 58.9–84.8 |
| 3rd trimester: optimal cut-off | 1.5 | 0.9–2.9 |
| 3rd trimester: optimal sensitivity | 66.2 | 43.4–85.3 |
| 3rd trimester: optimal specificity | 71.3 | 50.2–90.4 |
| Characteristics | Non-Smokers n (%) | Smokers n (%) | Se (95%CI) | Sp (95% CI) | PV+ (95% CI) | PV− (95% CI) | ||
|---|---|---|---|---|---|---|---|---|
| <10 ng/mL | ≥10 ng/mL | <10 ng/mL | ≥10 ng/mL | |||||
| the 1st trimester of pregnancy | ||||||||
| All the women | 1214 (95.3) | 60 (4.7) | 5 (3.2) | 152 (96.8) | 71.7 (65.1–77.7) | 99.6 (99.0–99.9) | 96.8 (92.7–99.0) | 95.3 (94.0–96.4) |
| Maternal age (years) | ||||||||
| <30 | 667 (93.8) | 44 (6.2) * | 4 (3.7) | 103 (96.3) | 70.1 (62.0–77.3) | 99.4 (98.5–99.8) | 96.3 (90.7–99.0) | 93.8 (91.8–95.5) |
| ≥30 | 535 (97.1) | 16 (2.9) | 1 (2) | 48 (98) | 75 (62.6–85.0) | 99.8 (99.0–100) | 98 (89.1–99.9) | 97.1 (95.3–98.3) |
| Parity | ||||||||
| 0 | 638 (95.7) | 29 (4.3) | 2 (2.7) | 73 (97.3) | 71.6 (61.8–80.1) | 99.7 (98.9–100) | 97.3 (90.7–99.7) | 95.7 (93.8–97.1) |
| 1 | 407 (95.8) | 18 (4.2) | 2 (3.5) | 55 (96.5) | 75.3 (63.9–84.7) | 99.5 (98.2–99.9) | 96.5 (87.9–99.6) | 95.8 (93.4–97.5) |
| ≥2 | 169 (92.9) | 13 (7.1) | 1 (4) | 24 (96.0) | 64.9 (47.5–79.8) | 99.4 (96.8–100) | 96 (79.6–99.9) | 92.9 (88.1–96.1) |
| Marital status | ||||||||
| Married | 996 (96.8) | 33 (3.2) ** | 3 (3.4) | 84 (96.6) | 71.8 (62.7–79.7) | 99.7 (99.1–99.9) | 96.6 (90.3–99.3) | 96.8 (95.5–97.8) |
| Single | 217 (88.9) | 27 (11.1) | 2 (2.9) | 68 (97.1) | 71.6 (61.4–80.4) | 99.1 (96.7–99.9) | 97.1 (90.1–99.7) | 88.9 (84.3–92.6) |
| Maternal education | ||||||||
| ≤9 | 27 (77.1) | 8 (22.9) *,a | 0 (0) | 35 (100) | 81.4 (66.6–91.6) | 100 (81.7–100) | 100 (85.5–100) | 77.1 (59.9–89.6) |
| 10–12 | 326 (91.1) | 32 (8.9) **,b | 3 (3.6) | 80 (96.4) | 71.4 (62.1–79.6) | 99.1 (97.4–99.8) | 96.4 (89.8–99.2) | 91.1 (87.6–93.8) |
| >12 | 860 (97.7) | 20 (2.3) **,c | 2 (5.3) | 36 (94.7) | 64.3 (50.4–76.6) | 99.8 (99.2–100) | 94.7 (82.3–99.4) | 97.7 (96.5–98.6) |
| the 3rd trimester of pregnancy | ||||||||
| All the women | 935 (95.4) | 45 (4.6) | 4 (4.0) | 95 (96) | 67.9 (59.4–75.5) | 99.6 (98.9–99.9) | 96.0 (90.0–98.9) | 95.4 (93.9–96.6) |
| Maternal age (years) | ||||||||
| <30 | 530 (94.3) | 32 (5.7) * | 4 (6.2) | 61 (93.8) | 65.6 (55.0–75.1) | 99.3 (98.1–99.8) | 93.8 (85–98.3) | 94.3 (92.1–96.1) |
| ≥30 | 399 (96.8) | 13 (3.2) | 0 (0) | 33 (100) | 71.7 (56.5–84.0) | 100 (98.6–100) | 100 (84.7–100) | 96.8 (94.7–98.3) |
| Parity | ||||||||
| 0 | 482 (95.3) | 24 (4.7) | 3 (5.9) | 48 (94.1) | 66.7 (54.6–77.3) | 99.4 (98.2–99.9) | 94.1 (83.8–98.8) | 95.3 (93.0–96.9) |
| 1 | 326 (95.9) | 14 (4.1) | 1 (3.4) | 28 (96.6) | 66.7 (50.5–80.4) | 99.7 (98.3–100) | 96.6 (82.2–99.9) | 95.9 (93.2–97.7) |
| ≥2 | 127 (94.8) | 7 (5.2) | 0 (0) | 19 (100) | 73.1 (52.2–88.4) | 100 (95.7–100) | 100 (75.1–100) | 94.8 (89.5–97.9) |
| Marital status | ||||||||
| Married | 773 (96.5) | 28 (3.5) ** | 2 (4.4) | 43 (95.6) | 60.6 (48.3–72.0) | 99.7 (99.1–100.0) | 95.6 (84.9–99.5) | 96.5 (95.0–97.7) |
| Single | 161 (90.4) | 17 (9.6) | 2 (3.7) | 52 (96.3) | 75.4 (63.5–84.9) | 98.8 (95.6–99.9) | 96.3 (87.3–99.5) | 90.4 (85.1–94.3) |
| Maternal education | ||||||||
| ≤9 | 20 (87) | 3 (13) | 0 (0) | 31 (100) | 91.2 (76.3–98.1) | 100 (76.2–100) | 100 (83.8–100) | 87 (66.4–97.2) |
| 10–12 | 265 (91.7) | 24 (8.3) **,b | 2 (3.8) | 50 (96.2) | 67.6 (55.7–78.0) | 99.3 (97.3–99.9) | 96.2 (86.8–99.5) | 91.7 (87.9–94.6) |
| >12 | 649 (97.3) | 18 (2.7) *,c | 2 (12.5) | 14 (87.5) *,c | 43.8 (26.4–62.3) | 99.7 (98.9–100) | 87.5 (61.7–98.4) | 97.3 (95.8–98.4) |
| Characteristics | Not Exposed to Passive Smoking ° n (%) | Exposed to Passive Smoking ° n (%) | Se (95%CI) | Sp (95% CI) | PV+ (95% CI) | PV− (95% CI) | ||
|---|---|---|---|---|---|---|---|---|
| <1.5 ng/mL | ≥1.5 ng/mL | <1.5 ng/mL | ≥1.5 ng/mL | |||||
| the 1st trimester of pregnancy | ||||||||
| All the women | 744 (70.7) | 309 (29.3) | 77 (36.8) | 132 (63.2) | 29.9 (25.7–34.4) | 90.6 (88.4–92.5) | 63.2 (56.2–69.7) | 70.7 (67.8–73.4) |
| Maternal age (years) | ||||||||
| <30 | 373 (67.6) | 179 (32.4) * | 58 (37.7) | 96 (62.3) | 34.9 (29.3–40.9) | 86.5 (83–89.6) | 62.3 (54.2–70.0) | 67.6 (63.5–71.5) |
| ≥30 | 362 (74.0) | 127 (26.0) | 19 (34.5) | 36 (65.5) | 22.1 (16.0–29.2) | 95 (92.3–97.0) | 65.5 (51.4–77.8) | 74 (69.9–77.9) |
| Parity | ||||||||
| 0 | 370 (69.9) | 159 (30.1) | 50 (37.9) | 82 (62.1) | 34 (28.1–40.4) | 88.1 (84.6–91) | 62.1 (53.3–70.4) | 69.9 (65.8–73.8) |
| 1 | 262 (70.1) | 112 (29.9) | 19 (39.6) | 29 (60.4) | 20.6 (14.2–28.2) | 93.2 (89.6–95.9) | 60.4 (45.3–74.2) | 70.1 (65.1–74.7) |
| ≥2 | 112 (74.7) | 38 (25.3) | 8 (27.6) | 21 (72.4) | 35.6 (23.6–49.1) | 93.3 (87.3–97.1) | 72.4 (52.8–87.3) | 74.7 (66.9–81.4) |
| Marital status | ||||||||
| Married | 646 (72.6) | 244 (27.4) ** | 57 (43.8) | 73 (56.2) * | 23 (18.5–28.1) | 91.9 (89.6–93.8) | 56.2 (47.2–64.8) | 72.6 (69.5–75.5) |
| Single | 98 (60.1) | 65 (39.9) | 20 (25.3) | 59 (74.7) | 47.6 (38.5–56.7) | 83.1 (75.0–89.3) | 74.7 (63.6–83.8) | 60.1 (52.2–67.7) |
| Maternal education | ||||||||
| ≤9 | 3 (23.1) | 10 (76.9) **,a | 6 (27.3) | 16 (72.7) | 61.5 (40.6–79.8) | 33.3 (7.5–70.1) | 72.7 (49.8–89.3) | 23.1 (5.0–53.8) |
| 10–12 | 167 (67.3) | 81 (32.7) | 33 (31.4) | 72 (68.6) *,b | 47.1 (38.9–55.3) | 83.5 (77.6–88.4) | 68.6 (58.8–77.3) | 67.3 (61.1–73.1) |
| >12 | 574 (72.6) | 217 (27.4) **,c | 38 (46.3) | 44 (53.7) | 16.9 (12.5–22) | 93.8 (91.6–95.6) | 53.7 (42.3–64.7) | 72.6 (69.3–75.6) |
| the 3rd trimester of pregnancy | ||||||||
| All the women | 590 (71.4) | 236 (28.6) | 51 (37.5) | 85 (62.5) | 26.5 (21.7–31.7) | 92 (89.7–94.0) | 62.5 (53.8–70.6) | 71.4 (68.2–74.5) |
| Maternal age (years) | ||||||||
| <30 | 316 (69.8) | 137 (30.2) | 38 (37.6) | 63 (62.4) | 31.5 (25.1–38.4) | 89.3 (85.6–92.3) | 62.4 (52.2–71.8) | 69.8 (65.3–74.0) |
| ≥30 | 268 (73.0) | 99 (27.0) | 13 (37.1) | 22 (62.9) | 18.2 (11.8–26.2) | 95.4 (92.2–97.5) | 62.9 (44.9–78.5) | 73 (68.2–77.5) |
| Parity | ||||||||
| 0 | 294 (73.0) | 109 (27.0) | 33 (35.9) | 59 (64.1) | 35.1 (27.9–42.8) | 89.9 (86.1–93.0) | 64.1 (53.5–73.9) | 73 (68.3–77.2) |
| 1 | 213 (68.7) | 97 (31.3) | 11 (42.3) | 15 (57.7) | 13.4 (7.7–21.1) | 95.1 (91.4–97.5) | 57.7 (36.9–76.6) | 68.7 (63.2–73.8) |
| ≥2 | 83 (73.5) | 30 (26.5) | 7 (38.9) | 11 (61.1) | 26.8 (14.2–42.9) | 92.2 (84.6–96.8) | 61.1 (35.7–82.7) | 73.5 (64.3–81.3) |
| Marital status | ||||||||
| Married | 503 (71.7) | 199 (28.3) | 33 (39.8) | 50 (60.2) | 20.1 (15.3–25.6) | 93.8 (91.5–95.7) | 60.2 (48.9–70.8) | 71.7 (68.2–75.0) |
| Single | 86 (69.9) | 37 (30.1) | 18 (34.0) | 35 (66.0) | 48.6 (36.7–60.7) | 82.7 (74.0–89.4) | 66 (51.7–78.5) | 69.9 (61.0–77.9) |
| Maternal education | ||||||||
| ≤9 | 5 (41.7) | 7 (58.3) | 2 (18.2) | 9 (81.8) | 56.3 (29.9–80.2) | 71.4 (29.0–96.3) | 81.8 (48.2–97.7) | 41.7 (15.2–72.3) |
| 10–12 | 134 (63.8) | 76 (36.2) *,b | 29 (39.2) | 45 (60.8) | 37.2 (28.6–46.4) | 82.2 (75.5–87.7) | 60.8 (48.8–72.0) | 63.8 (56.9–70.3) |
| >12 | 450 (74.6) | 153 (25.4) *,c | 20 (39.2) | 31 (60.8) | 16.8 (11.7–23.1) | 95.7 (93.5–97.4) | 60.8 (46.1–74.2) | 74.6 (71.0–78.1) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polanska, K.; Krol, A.; Kaluzny, P.; Ligocka, D.; Mikolajewska, K.; Shaheen, S.; Walton, R.; Hanke, W. Estimation of Saliva Cotinine Cut-Off Points for Active and Passive Smoking during Pregnancy—Polish Mother and Child Cohort (REPRO_PL). Int. J. Environ. Res. Public Health 2016, 13, 1216. https://doi.org/10.3390/ijerph13121216
Polanska K, Krol A, Kaluzny P, Ligocka D, Mikolajewska K, Shaheen S, Walton R, Hanke W. Estimation of Saliva Cotinine Cut-Off Points for Active and Passive Smoking during Pregnancy—Polish Mother and Child Cohort (REPRO_PL). International Journal of Environmental Research and Public Health. 2016; 13(12):1216. https://doi.org/10.3390/ijerph13121216
Chicago/Turabian StylePolanska, Kinga, Anna Krol, Pawel Kaluzny, Danuta Ligocka, Karolina Mikolajewska, Seif Shaheen, Robert Walton, and Wojciech Hanke. 2016. "Estimation of Saliva Cotinine Cut-Off Points for Active and Passive Smoking during Pregnancy—Polish Mother and Child Cohort (REPRO_PL)" International Journal of Environmental Research and Public Health 13, no. 12: 1216. https://doi.org/10.3390/ijerph13121216
APA StylePolanska, K., Krol, A., Kaluzny, P., Ligocka, D., Mikolajewska, K., Shaheen, S., Walton, R., & Hanke, W. (2016). Estimation of Saliva Cotinine Cut-Off Points for Active and Passive Smoking during Pregnancy—Polish Mother and Child Cohort (REPRO_PL). International Journal of Environmental Research and Public Health, 13(12), 1216. https://doi.org/10.3390/ijerph13121216