
Disparities in Hypertension Prevalence, Awareness, Treatment and Control between Bouyei and Han: Results from a Bi-Ethnic Health Survey in Developing Regions from South China

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurements
2.3. Definitions
2.4. Ethics
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics
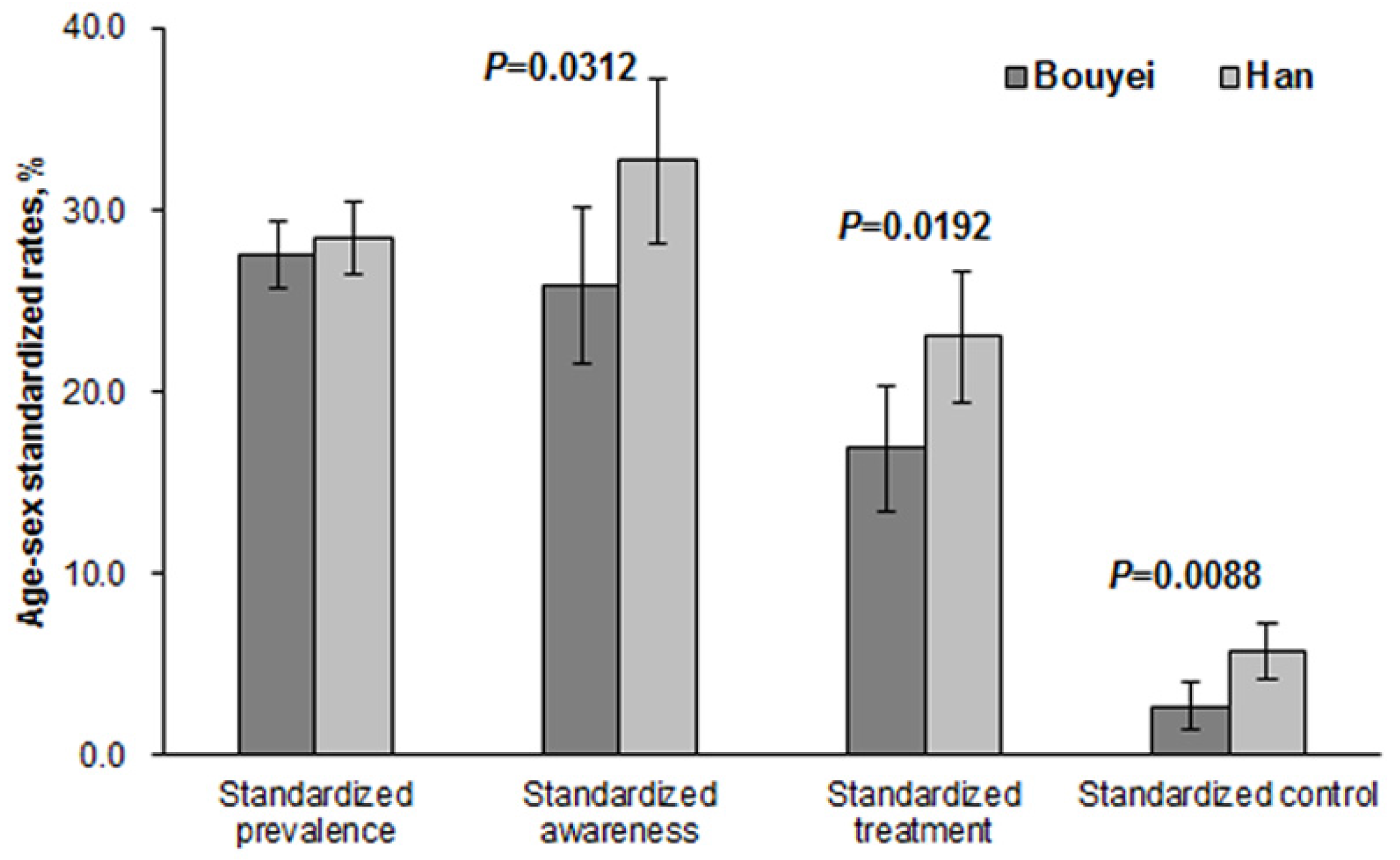
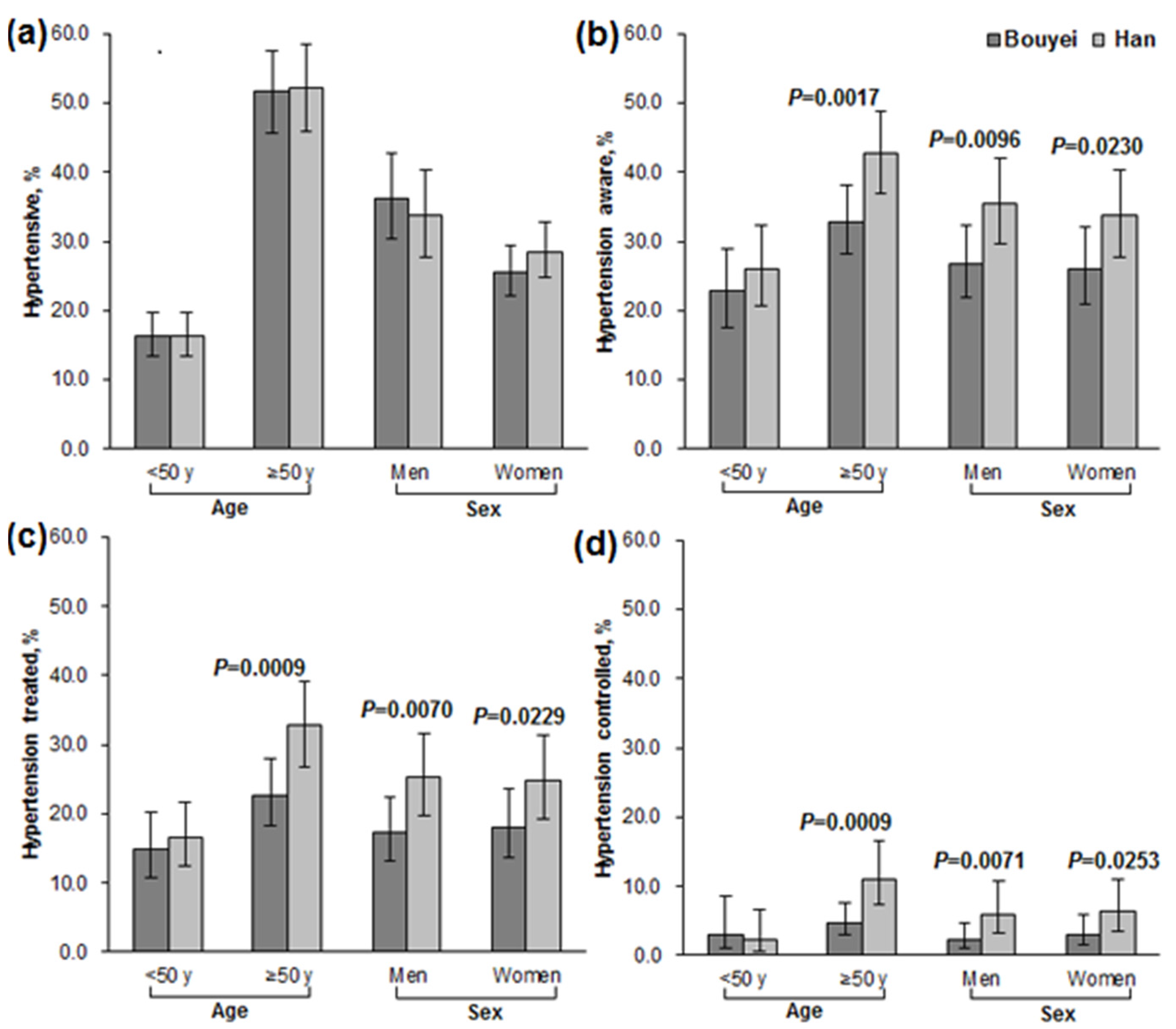
3.2. Prevalence, Awareness, Treatment, and Control
3.3. Associated Factors of Hypertension
3.4. Associated Factors of Effective Hypertension Control in Treated Patients
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| HBP | High Blood Pressure |
| BP | Blood Pressure |
| SBP | Systolic Blood Pressure |
| DBP | Diastolic Blood Pressure |
| IQR | Interquartile range |
| TC | Total Cholesterol |
| TG | Triglyceride |
| LDL | Low-Density Lipoproteins Cholesterol |
| HDL | High-Density Lipoproteins Cholesterol |
| CKD | Chronic Kidney Disease |
References
- Martin, M.J.; Hulley, S.B.; Browner, W.S.; Kuller, L.H.; Wentworth, D. Serum cholesterol, blood pressure, and mortality: Implications from a cohort of 361,662 men. Lancet 1986, 328, 933–936. [Google Scholar] [CrossRef]
- Dzau, V.; Braunwald, E. Resolved and unresolved issues in the prevention and treatment of coronary artery disease: A workshop consensus statement. Am. Heart J. 1991, 121, 1244–1263. [Google Scholar] [CrossRef]
- WHO. A Global Brief on Hypertension: Silent Killer, Global Public Health Crisis; World Health Day 2013; WHO: Geneva, Switzerland, 2013; pp. 1–39. [Google Scholar]
- Liu, L.P.; Wang, D.; Wong, K.S.; Wang, Y.J. Stroke and stroke care in China: Huge burden, significant workload, and a national priority. Stroke 2011, 42, 3651–3654. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Millett, C. Social epidemiology of hypertension in middle-income countries: Determinants of prevalence, diagnosis, treatment, and control in the WHO SAGE study. Hypertension 2013, 62, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Chow, C.K.; Teo, K.K.; Rangarajan, S.; Islam, S.; Gupta, R.; Avezum, A.; Bahonar, A.; Chifamba, J.; Dagenais, G.; Diaz, R.; et al. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, low-income countries. JAMA 2013, 310, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Li, T.D.; Xiong, H. An analysis on unequal phenomenon of economic development in eastern and western areas. J. Southwest Univ. Natl. 2005, 26, 183–186. [Google Scholar]
- Guizhou Provincial Bureau of Statistics. Guizhou Statistical Yearbook 2011; China Statistics Press: Beijing, China, 2012.
- National Bureau of Statistics of China (NBS). Tabulation on the 2010 Population Census of People’s Republic of China; China Statistics Press: Beijing, China, 2012.
- Hu, Y.S.; Yao, C.H.; Wang, W.Z.; Hu, J.P.; He, Y.N.; Zhai, F.Y. Survey on the prevalence of hypertension in different ethnic groups in China in 2002. J. Hyg. Res. 2006, 35, 573–575. [Google Scholar]
- Jones, D.W.; Hall, J.E. Racial and ethnic differences in blood pressure: Biology and sociology. Circulation 2006, 114, 2757–2759. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.M.; Beevers, D.G. Management of hypertension in ethnic minorities. Heart 2005, 91, 1105–1109. [Google Scholar] [CrossRef] [PubMed]
- EI Assaad, M.A.; Topouchian, J.A.; Darne, B.M.; Asmar, R.G. Validation of the Omron 907 device for blood pressure measurement. Blood Press Monit. 2002, 7, 237–241. [Google Scholar] [CrossRef]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T.; et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure; the JNC 7 report. JAMA 2003, 289, 2560–2572. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Recommendations on Physical Activity for Health. 2011. Available online: www.who.int/dietphysicalactivity/leaflet-physical-activity-recommendations.pdf (accessed on 6 June 2015).
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, D.T.; LeFevre, M.L.; MacKenzie, T.D.; Ogedegbe, O.; et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC8). JAMA 2014, 311, 507–520. [Google Scholar] [CrossRef] [PubMed]
- Rabe-Hesketh, S.; Skrondal, A. Multilevel modeling of complex survey data. J. R. Stat. Soc. A 2006, 169, 805–827. [Google Scholar] [CrossRef]
- Ping, B.; Xie, X.X.; Wang, Y.X.; Zhang, S.Q.; Wang, Y.X.; Mao, X.H. Analysis of epidemiologic characteristics of major chronic diseases of the Han and Buyi Adults in LongLi County. Mod. Prev. Med. 2014, 41, 3659–3664. [Google Scholar]
- Li, L.; Zhou, J.; Xu, L.N.; Chen, M.; Yao, Y.T.; Liu, T.; Sun, L.X. Analysis of hypertension of urban and rural areas of Guizhou Province. Chin. J. Health Educ. 2014, 30, 407–410. [Google Scholar]
- Wang, J.W.; Zhang, L.X.; Wang, F.; Liu, L.S.; Wang, H.Y.; the China National Survey of Chronic Kidney Disease Working Group. Prevalence, awareness, treatment, and control of hypertension in China: Results from a national survey. Am. J. Hypertens. 2014, 27, 1355–1361. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.; Dong, G.H.; Wang, D.; Liu, M.M.; Lin, Q.; Meng, X.J.; Xu, L.X.; Hou, H.; Ren, Y.F. Factors associated with prevalence, awareness, treatment and control of hypertension in urban adults from 33 communities in China: The CHPSNE Study. Hypertens. Res. 2011, 34, 1087–1092. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Zhu, Y.C.; Chen, Y.P.; Hu, Y.; Tang, X.W.; Zhang, B. The dynamics of hypertension prevalence, awareness, treatment, control and associated factors in Chinese adults: Results from CHNS 1991–2011. J. Hypertens. 2015, 33, 1688–1696. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.L.; Sun, K.; Yang, Y.; Zhang, H.Y.; Hu, F.B.; Hui, R.T. Plasma uric acid and hypertension in a Chinese community: Prospective study and metaanalysis. Clin. Chem. 2009, 55, 2026–2034. [Google Scholar] [CrossRef] [PubMed]
- Nagahama, K.; Inoue, T.; Iseki, K.; Touma, T.; Kinjo, K.; Ohya, Y.; Takishita, S. Hyperuricemia as a predictor of hypertension in a screened cohort in Okinawa, Japan. Hypertens. Res. 2004, 27, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Mazzali, M.; Hughes, J.; Kim, Y.G.; Jefferson, J.A.; Kang, D.H.; Gordon, K.L.; Lan, H.Y.; Kivlighn, S.; Johnson, R.J. Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hypertension 2001, 38, 1101–1106. [Google Scholar] [CrossRef] [PubMed]
- Mazzali, M.; Kanbay, M.; Segal, M.S.; Shafiu, M.; Jalal, D.; Feig, D.I.; Johnson, R.J. Uric acid and hypertension: Cause or Effect. Curr. Rheumatol. Rep. 2010, 12, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Barber, S.L.; Yao, L. Health Insurance Systems in China: A Briefing Note; World Health Report; Word Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Ishikawa-Takata, K.; Ohta, T.; Tanaka, H. How much exercise is required to reduce blood pressure in essential hypertensives: A dose-response study. Am. J. Hypertens. 2003, 16, 629–633. [Google Scholar] [CrossRef]
- Véras-Silva, A.S.; Mattos, K.C.; Gava, N.S.; Brum, P.C.; Negrão, C.E.; Krieger, E.M. Low-intensity exercise training decreases cardiac output and hypertension in spontaneously hypertensive rats. Am. J. Physiol. 1997, 273, H2627–H2631. [Google Scholar] [PubMed]
- Cleroux, J.; Kouame, N.; Nadeau, A.; Coulombe, D.; Lacourciere, Y. Aftereffects of exercise on regional and systemic hemodynamics in hypertension. Hypertension 1992, 19, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Arakawa, K. Antihypertensive mechanism of exercise. J. Hypertens. 1993, 11, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.; Li, W.T.; Peng, X.; Zhang, P.; An, L.B. Current status of evaluation of health education for hypertension patients in community in China. Chin. Gen. Pract. 2013, 15, 4190–4193. [Google Scholar]
- Wang, H.; Zhang, X.W.; Zhang, J.; He, Q.F.; Hu, R.Y.; Wang, L.X.; Su, D.T.; Xiao, Y.Y.; Pan, J.; Zhen, Y. Factors associated with prevalence, awareness, treatment and control of hypertension among adults in Southern China: A community-based, cross-sectional survey. PLoS ONE 2013, 8, e62469. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Liu, H.M.; Ru, X.J.; Zhang, H.; Wu, S.P.; Wang, W.Z. Hypertension detection, management, control and associated factors among residents accessing community health services in Beijing. Sci. Rep. 2014, 4, 4845. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Bouyei (n = 2746) | Han (n = 2824) | p |
|---|---|---|---|
| No. (%) a | – | – | – |
| Rural | 2430 (88.5) | 996 (35.3) | <0.0001 |
| Men | 1157 (42.1) | 1140 (40.4) | 0.1808 |
| Education | – | – | – |
| Low | 1655 (60.6) | 930 (33.1) | <0.0001 |
| Medium | 797 (29.2) | 1119(39.8) | |
| High | 279 (10.2) | 761 (27.1) | |
| Smoking, never | 1841 (67.1) | 1899 (67.6) | 0.6979 |
| Alcohol Consumption | – | – | – |
| Never/Ex-drinker | 1642 (59.8) | 1832 (65.2) | <0.0001 |
| Light use | 432 (15.7) | 629 (22.4) | |
| Harmful use | 672 (24.5) | 350 (12.5) | |
| Recreational Activity | – | – | – |
| High | 132 (4.9) | 602 (21.5) | <0.0001 |
| Moderate | 142 (5.2) | 418 (14.9) | |
| Low | 2444 (89.9) | 1780 (63.6) | |
| Occupational activity | – | – | – |
| High | 1597 (58.3) | 540 (19.2) | <0.0001 |
| Moderate | 161 (5.9) | 282 (10.0) | |
| Low | 982 (35.8) | 1997 (70.8) | |
| Income | – | – | – |
| Low | 1021 (37.5) | 401 (14.4) | <0.0001 |
| Low-middle | 825 (30.3) | 528 (18.9) | |
| Upper-middle | 463 (17.0) | 964 (34.5) | |
| High | 414 (15.2) | 898 (32.2) | |
| Health insurance, insured | 2709 (98.8) | 2752 (97.6) | 0.0004 |
| Family history, yes | 316 (11.5) | 878 (31.1) | <0.0001 |
| Central obesity b | 408 (19.4) | 939 (39.1) | <0.0001 |
| Hyperuricemia c | 273 (10.0) | 410 (14.7) | <0.0001 |
| Median (IQR) | – | – | – |
| Age, year | 50 (40,62) | 48 (37,60) | <0.0001 |
| Systolic BP, mmHg | 129 (117,145) | 127 (115,142) | <0.0001 |
| Diastolic BP, mmHg | 77 (70,86) | 77 (70,86) | 0.9695 |
| Fasting glucose, mmol/L | 4.9 (4.5,5.3) | 4.9 (4.6,5.3) | 0.0002 |
| TC, mmol/L | 4.8 (4.2,5.5) | 4.9 (4.3,5.6) | 0.0033 |
| TG, mmol/L | 1.1 (0.8,1.6) | 1.3 (0.9,2.0) | <0.0001 |
| LDL, mmol/L | 2.6 (2.1,3.2) | 2.8 (2.3,3.3) | <0.0001 |
| HDL, mmol/L | 1.6 (1.3,1.8) | 1.4 (1.2,1.6) | <0.0001 |
| Age a and Sex | Prevalence, No. (%) | Awareness among Hypertension, No. (%) | Treatment among Hypertension, No. (%) | Control among Hypertension, No. (%) | ||||
|---|---|---|---|---|---|---|---|---|
| Bouyei | Han | Bouyei | Han | Bouyei | Han | Bouyei | Han | |
| Age | – | – | – | – | – | – | – | – |
| <50 year | 237 (17.9) | 261 (16.8) | 54 (22.8) | 69 (26.4) | 35 (14.8) | 43 (16.5) | 5 (2.1) | 6 (2.3) |
| ≥50 year | 731 (51.5) | 691 (54.6) | 237 (32.4) | 314 (45.4) | 156 (21.3) | 253 (36.6) | 30 (4.1) | 88 (12.7) |
| Sex | – | – | – | – | – | – | – | – |
| Men | 479 (41.4) | 427 (37.5) | 145 (30.3) | 171 (40.1) | 89 (18.6) | 124 (29.0) | 15 (3.1) | 41 (9.6) |
| Women | 489 (30.8) | 525 (31.2) | 146 (29.9) | 212 (40.4) | 102 (20.9) | 172 (32.8) | 20 (4.1) | 53 (10.1) |
| All | 968 (35.3) | 952 (33.7) | 291 (30.1) | 383 (40.2) | 191 (19.7) | 296 (31.1) | 35 (3.6) | 94 (9.9) |
| Variables | Bouyei | Han | ||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Location (Ref = rural) | 0.99 (0.63, 1.56) | 0.9647 | 1.08 (0.75, 1.56) | 0.6750 |
| Age (Ref ≤ 50 years) | 5.23 (4.11, 6.65) | <0.0001 | 4.93 (3.91, 6.22) | <0.0001 |
| Education (Ref = low) | – | – | – | – |
| High | 0.79 (0.50, 1.24) | 0.2985 | 0.64 (0.46, 0.90) | 0.0096 |
| Medium | 0.85 (0.66, 1.11) | 0.2292 | 0.74 (0.57, 0.96) | 0.0229 |
| Insurance (Ref = no) | 0.75 (0.26, 2.15) | 0.5963 | 2.18 (0.89, 5.38) | 0.0900 |
| Family history (Ref = yes) | 0.89 (0.64, 1.24) | 0.4795 | 0.57 (0.46, 0.71) | <0.0001 |
| Physical activity (Ref = low) | – | – | – | – |
| High | 1.01 (0.79, 1.29) | 0.9514 | 1.17 (0.92, 1.48) | 0.1953 |
| Moderate | 0.84 (0.56, 1.26) | 0.3899 | 1.00 (0.75, 1.33) | 0.9723 |
| Alcohol drinker (Ref = harmful) | – | – | – | – |
| Non/ex drinker | 0.55 (0.42, 0.72) | <.0001 | 0.75 (0.54, 1.03) | 0.0805 |
| Light drinker | 0.56 (0.41, 0.77) | 0.0004 | 0.77 (0.54, 1.08) | 0.1315 |
| Smoking (Ref = ever) | 1.00 (0.78, 1.28) | 0.9886 | 0.89 (0.70, 1.12) | 0.3171 |
| Central obesity (Ref = no) | 1.96 (1.49, 2.58) | <0.0001 | 2.31 (1.87, 2.86) | <0.0001 |
| Diabetes (Ref = no) a | 1.81 (1.00, 3.27) | 0.0489 | 2.08 (1.42, 3.04) | 0.0002 |
| Dyslipidemia (Ref = no) b | 1.71 (1.33, 2.21) | <0.0001 | 1.32 (1.07, 1.65) | 0.0117 |
| Hyperuricemia (Ref = no) | 2.19 (1.57, 3.05) | <0.0001 | 1.98 (1.49, 2.63) | <0.0001 |
| Variables | Bouyei a | Han | ||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Age (Ref ≤ 50 years) | 0.93 (0.26, 3.37) | 0.9081 | 3.68 (1.25, 10.80) | 0.0182 |
| Sex (Ref = women) | 0.87 (0.20, 3.87) | 0.8560 | 1.95 (0.75, 5.03) | 0.1681 |
| Family history (Ref = yes) | 1.75 (0.43, 7.13) | 0.4384 | 0.63 (0.35, 1.14) | 0.1263 |
| Physical activity (Ref = low) | – | – | – | – |
| High | 1.87 (0.71, 4.93) | 0.4998 | 1.85 (0.91, 3.73) | 0.0880 |
| Moderate | 6.98 (1.34, 36.36) | 0.0371 | 2.07 (0.82, 5.20) | 0.1215 |
| Alcohol drinker (Ref = harmful) | – | – | – | – |
| Non/ex drinker | 1.88 (0.53, 6.70) | 0.2564 | 1.92 (0.68, 5.38) | 0.2164 |
| Light drinker | 1.01 (0.20, 5.20) | 0.6688 | 1.31 (0.39, 4.37) | 0.6580 |
| Smoking (Ref = ever) | 0.51 (0.11, 2.28) | 0.3780 | 1.80 (0.69, 4.70) | 0.2281 |
| Central obesity (Ref = no) | 1.25 (0.47, 3.36) | 0.6554 | 1.03 (0.55, 1.92) | 0.9244 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dong, F.; Wang, D.; Pan, L.; Yu, Y.; Wang, K.; Li, L.; Wang, L.; Liu, T.; Zeng, X.; Sun, L.; et al. Disparities in Hypertension Prevalence, Awareness, Treatment and Control between Bouyei and Han: Results from a Bi-Ethnic Health Survey in Developing Regions from South China. Int. J. Environ. Res. Public Health 2016, 13, 233. https://doi.org/10.3390/ijerph13020233
Dong F, Wang D, Pan L, Yu Y, Wang K, Li L, Wang L, Liu T, Zeng X, Sun L, et al. Disparities in Hypertension Prevalence, Awareness, Treatment and Control between Bouyei and Han: Results from a Bi-Ethnic Health Survey in Developing Regions from South China. International Journal of Environmental Research and Public Health. 2016; 13(2):233. https://doi.org/10.3390/ijerph13020233
Chicago/Turabian StyleDong, Fen, Dingming Wang, Li Pan, Yangwen Yu, Ke Wang, Ling Li, Li Wang, Tao Liu, Xianjia Zeng, Liangxian Sun, and et al. 2016. "Disparities in Hypertension Prevalence, Awareness, Treatment and Control between Bouyei and Han: Results from a Bi-Ethnic Health Survey in Developing Regions from South China" International Journal of Environmental Research and Public Health 13, no. 2: 233. https://doi.org/10.3390/ijerph13020233
APA StyleDong, F., Wang, D., Pan, L., Yu, Y., Wang, K., Li, L., Wang, L., Liu, T., Zeng, X., Sun, L., Zhu, G., Feng, K., Zhang, B., Xu, K., Pang, X., Chen, T., Pan, H., Ma, J., Zhong, Y., ... Shan, G. (2016). Disparities in Hypertension Prevalence, Awareness, Treatment and Control between Bouyei and Han: Results from a Bi-Ethnic Health Survey in Developing Regions from South China. International Journal of Environmental Research and Public Health, 13(2), 233. https://doi.org/10.3390/ijerph13020233