
The Effects of Coarse Particles on Daily Mortality: A Case-Crossover Study in a Subtropical City, Taipei, Taiwan

Abstract
:1. Introduction
2. Materials and Methods
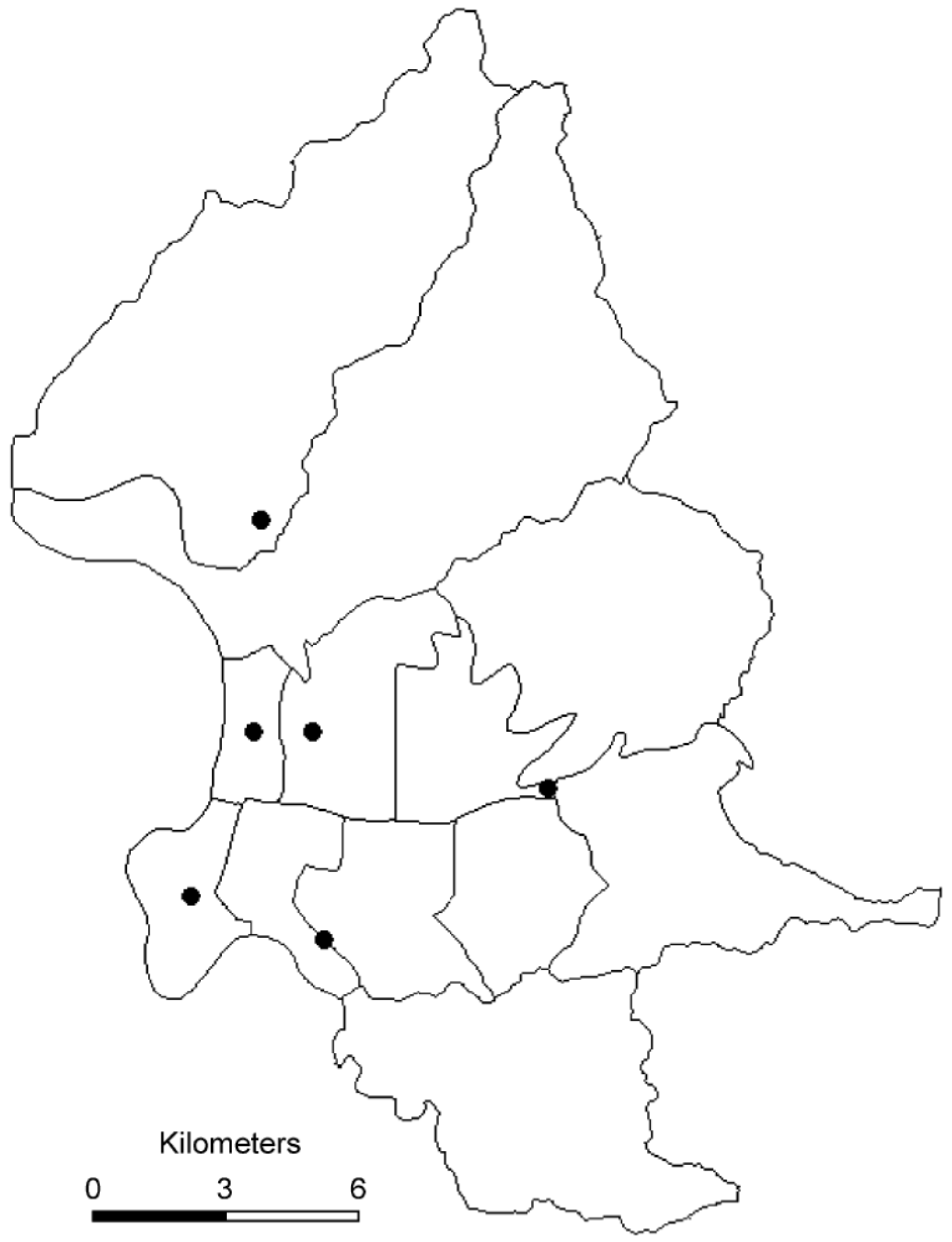
2.1. Taipei City
2.2. Mortality Data
2.3. Pollutants and Meteorological Data
2.4. Statistics
3. Results and Discussion
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Levy, J.I.; Hammitt, J.K.; Spengler, J.D. Estimating the mortality impacts of particulate matter: What can be learned from between-study variability? Environ. Health Perspect. 2000, 108, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A.; Burnett, R.T.; Thurston, G.D.; Thun, M.J.; Calle, E.E.; Krewski, D.P.; Godleski, J.J. Cardiovascular mortality and long-term exposure to particulate air pollution: Epidemiological evidence of general pathophysiological pathways of disease. Circulation 2004, 109, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Goodman, P.G.; Dockery, D.W.; Clancy, L. Cause-specific mortality and the extended effects of particulate pollution and temperature exposure. Environ. Health Perspect. 2004, 112, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Analitis, A.; Katsouyanni, K.; Dimakopoulou, K.; Samoli, E.; Nikoloulopoulos, A.K.; Petasakis, Y.; Touloumi, G.; Schwartz, J.; Anderson, H.R.; Cambra, K.; et al. Short-term effects of ambient particles on cardiovascular and respiratory mortality. Epidemiology 2006, 17, 230–233. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J. The effects of particulate air pollution on daily deaths: A multi-city case-crossover analysis. Occup. Environ. Med. 2004, 61, 956–961. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.J.; Anderson, H.R.; Ostra, B.; Pandey, K.D.; Krzyzanowski, M.; Kunzli, N.; Gutschmidt, K.; Pope, A.; Romieu, I.; Samet, J.M.; et al. The global burden of disease due to outdoor air pollution. J. Toxicol. Environ. Health Part A 2006, 68, 1–7. [Google Scholar]
- World Health Organization (WHO). WHO Air Quality Guidelines: Global Update 2005; Geneva, Switzerland, 2006. [Google Scholar]
- Samet, J.M.; Graff, D.; Bernsten, J.; Ghio, A.J.; Huang, Y.C.; Delvin, R.B. A comparison of studies on the effects of controlled exposure to fine, coarse, and ultrafine ambient particulate matter from a single location. Inhal. Toxicol. 2007, 19, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Zanobetti, A.; Schwartz, J.; Dockery, D.W. Airborne particles are a risk factor for hospital admissions for heart and lung disease. Environ. Health Perspect. 2000, 108, 1071–1077. [Google Scholar] [CrossRef] [PubMed]
- Le Tertre, A.; Medina, S.; Samoli, E.; Forsberg, B.; Michelozzi, P.; Boumghar, A.; Boumghar, A.; Vonk, J.M.; Bellini, A.; Atkinson, R.; et al. Short-term effects of particulate air pollution on cardiovascular diseases in eight European cities. J. Epidemiol. Community Health 2002, 56, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Bedeschi, E.; Campari, C.; Candela, S.; Collini, G.; Caranci, N.; Frasca, G.; Galassi, C.; Francesca, G.; Vigotti, M.A. Urban air pollution and respiratory emergency visits at pediatric unit, Reggio Emilia, Italy. J. Toxicol. Environ. Health Part A 2007, 70, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Beckerman, B.S.; Jerrett, M.; Finkelestein, M.; Kanaroglou, P.; Brook, J.R.; Arain, M.A.; Sears, M.R.; Stieb, D.; Balmes, J.; Chapman, K. The association between chronic exposure to traffic-related air pollution and ischemic heart disease. J. Toxicol. Environ. Health Part A 2012, 75, 402–411. [Google Scholar] [CrossRef] [PubMed]
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L.; Samet, J.M. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. J. Am. Med. Assoc. 2006, 295, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Cifuentes, L.A.; Vega, J.; Kopfer, K.; Lave, L.B. Effect of the fine fraction of particulate matter versus the coarse mass and other pollutants on daily nortality in Santiago Chile. J. Air Waste Manag. Assoc. 2000, 50, 1287–1298. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.; Dockery, D.W.; Neas, L.M. Is daily mortality associated specifically with fine particles? J. Air Waste Manage. Assoc. 1996, 46, 927–939. [Google Scholar] [CrossRef]
- Zanobetti, A.; Schwartz, J. The effect of fine and coarse particulate air pollution and mortality: A national analysis. Environ. Health Perspect. 2009, 117, 898–903. [Google Scholar] [CrossRef] [PubMed]
- Liao, D.; Shaffer, M.L.; He, F.; Rodriguez-Colon, S.; Eu, R.; Whitsel, E.A.; Bixler, E.O.; Cascio, W.E. Fine particulate air pollution is associated with higher vulnerability to atrial fibrillation—The APACR study. J. Toxicol. Environ. Health Part A 2011, 74, 693–705. [Google Scholar] [CrossRef] [PubMed]
- Wilson, W.E.; Suh, H.H. Fine particles and coarse particles: Concentration relationship relevant to epidemiologic studies. J. Air Waste Manag. Assoc. 1997, 47, 1238–1249. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A.; Dockery, D.W. Health effects of fine particulate air pollution: Lines that connect. J. Air Waste Manage. Assoc. 2006, 36, 709–742. [Google Scholar] [CrossRef]
- Brunekreef, B.; Forsberg, B. Epidemiological evidence of effects of coarse airborne particles on health. Eur. Respir. J. 2005, 26, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Li, Y.; Ma, Y.; Pan, G.; Zeng, G.; Xu, X.; Chen, B.; Kan, H. Coarse particles and mortality in three Chinese cities: The China air pollution and health effects study (CAPES). Sci. Total Environ. 2011, 409, 4934–4938. [Google Scholar] [CrossRef] [PubMed]
- Fang, G.C.; Chang, C.N.; Wu, Y.S.; Wang, V.; Fu, P.P.; Yang, D.G. The study of fine and coarse particles, and metallic elements for the daytime and night time in a suburban area of central Taiwan, Taichung. Chemosphere 2000, 41, 639–644. [Google Scholar] [CrossRef]
- Wang, H.; Shooter, D. Source apportionment of fine and coarse atmospheric particles in Auckland, New Zealand. Sci. Total Environ. 2005, 340, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Peng, R.D.; Bell, M.L.; Geyh, A.S.; McDermott, A.; Zeger, S.L.; Samet, J.M.; Dominici, F. Emergency admissions for cardiovascular and respiratory diseases and the chemical composition of fine particle air pollution. Environ. Health Perspect. 2009, 117, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Suh, H.H.; Zanobetti, A.; Schwartz, J.; Coull, B.A. Chemical properties of air pollutants and cause-specific hospital admissions among the elderly in Atlanta, Georgia. Environ. Health Perspect. 2011, 119, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Peng, R.D.; Chang, H.H.; Bell, M.L.; McDermott, A.; Zeger, S.L.; Samet, J.M.; Dominici, F. Coarse particulate matter air pollution and hospital admissions for cardiovascular and respiratory diseases among medicare patients. J. Am. Med. Assoc. 2008, 299, 2172–2179. [Google Scholar] [CrossRef] [PubMed]
- Malig, B.J.; Ostro, B.D. Coarse particles and mortality: Evidence from a multi-city study in California. Occup. Environ. Med. 2009, 66, 832–839. [Google Scholar] [CrossRef] [PubMed]
- Kan, H.; London, S.J.; Chen, G.; Zhang, Y.; Song, G.; Zhao, N.; Jiang, L.; Chen, B. Differentiating the effects of fine and coarse particles on daily mortality in Shanghai, China. Environ. Int. 2007, 33, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Janssen, N.A.H.; Fischer, P.; Marra, M.; Ameling, C.; Cassee, F.R. Short-term effects of PM2.5, PM10 and PM2.5–10 on daily mortality in the Netherlands. Sci. Total Environ. 2013, 463, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Samoli, E.; Stafoggia, M.; Rodopoulou, S.; Ostro, B.; Declercq, C.; Alessandrini, E.; Diaz, J.; Karanasiou, A.; Kelessis, A.G.; Le Tertre, A.; et al. Association between fine and coarse particles and mortality in Mediterranean cities: Results from the MED-PARTICLES project. Environ. Health Perspect. 2013, 121, 932–938. [Google Scholar] [CrossRef] [PubMed]
- Meister, K.; Johansson, C.; Forsberg, B. Estimated short-term effects of coarse particles on daily mortality in Stockholm, Sweden. Environ. Health Perspect. 2012, 120, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; Ebisu, K.; Peng, R.D.; Walker, J.; Samet, J.M.; Zeger, S.L.; Dominici, F. Seasonal and regional short-term effects of fine particles on hospital admissions in 202 US counties, 1999–2005. Am. J. Epidemiol. 2008, 168, 1301–1310. [Google Scholar] [CrossRef] [PubMed]
- Maclure, M. The case-crossover design: A method for studying transient effects on the risk of acute events. Am. J. Epidemiol. 1991, 133, 144–153. [Google Scholar] [PubMed]
- Marshall, R.J.; Jackson, R.T. Analysis of case-crossover designs. Stat. Med. 1993, 12, 2333–2341. [Google Scholar] [CrossRef] [PubMed]
- Mittleman, M.A.; Maclure, M.; Robins, J.M. Control sampling strategies for case-crossover studies: An assessment of relative efficiency. Am. J. Epidemiol. 1995, 142, 91–98. [Google Scholar] [PubMed]
- Levy, D.; Lumley, T.; Sheppard, L.; Kaufman, J.; Checkoway, H. Referent selection in case-crossover analyses of acute health effects of air pollution. Epidemiology 2001, 12, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Neas, L.N.; Schwartz, J.; Dockery, D. A case-crossover analysis of air pollution and mortality in Philadelphia. Environ. Health Perspect. 1999, 107, 629–631. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.T.; Schwartz, J. Reanalysis of the effects of air pollution on daily mortality in Seoul, Korea: A case-crossover design. Environ. Health Perspect. 1999, 107, 633–636. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Zeger, S. On the equivalence of case-crossover and time series methods in environmental epidemiology. Biostatistics 2007, 8, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Lumley, T.; Levy, D. Bias in the case-crossover design: Implications for studies of air pollution. Environmetrics 2000, 11, 689–704. [Google Scholar] [CrossRef]
- Janes, H.; Sheppard, L.; Lumley, T. Case-crossover analyses of air pollution exposure data: Referent selection strategies and their implications for bias. Epidemiology 2005, 16, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Mittleman, M.A. Optimal referent selection strategies in case-crossover studies: A settled issue. Epidemiology 2005, 16, 15–16. [Google Scholar] [CrossRef]
- Katsouyanni, K.; Touloumi, G.; Spix, C.; Schwartz, J.; Balducci, F.; Medina, S.; Rossi, G.; Wojtyniak, B.; Sunyer, J.; Bacharova, L.; et al. Short term effects of ambient sulphur dioxide and particulate matter on mortality in 12 European cities: Results from time series data from the APHEA project. Br. Med. J. 1997, 314, 1658–1663. [Google Scholar] [CrossRef]
- Hsieh, Y.L.; Yang, Y.H.; Wu, T.N.; Yang, C.Y. Air pollution and hospital admissions for myocardial infarction in a subtropical city: Taipei, Taiwan. J. Toxicol. Environ. Health A 2010, 73, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Dockery, D.W.; Pope, C.A. An association between air pollution and mortality in six U.S. cities. New Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Englert, N. Fine particles and human health—A review of epidemiological studies. Toxicol. Lett. 2004, 149, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Mar, T.F.; Norris, G.A.; Koenig, J.Q.; Larson, T.V. Associations between air pollution and mortality in Phoenix, 1995–1997. Environ. Health Perspect. 2000, 108, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Ostro, B.D.; Broadwin, R.; Lipsett, M.J. Coarse and fine particles and daily mortality in the Coachella Valley, California: A follow-up study. J. Expo. Anal. Environ. Epidemiol. 2000, 10, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Castillegos, M.; Borja-Aburto, V.H.; Dockery, D.W.; Gold, D.R.; Loomis, D. Airborne coarse particles and mortality. Inhal. Toxicol. 2000, 12, 61–72. [Google Scholar] [CrossRef]
- Mallone, S.; Stafoggia, M.; Faustini, A.; Gobi, G.P.; Marconi, A.; Forastiere, F. Saharan dust and association between particulate matter and daily mortality in Rome, Italy. Environ. Health Perspect. 2011, 119, 1409–1414. [Google Scholar] [CrossRef] [PubMed]
- Tobias, A.; Perez, L.; Diaz, J.; Linares, C.; Alastruey, A.; Querol, X. Short-term effects of particulate matter on total mortality during saharan dust outbreak: A case-crossover analysis in Madrid (Spain). Sci. Total Environ. 2011, 412, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Perez, L.; Tobias, A.; Querol, X.; Kunzli, N.; Pey, J.; Alastuey, A.; Viana, M.; Valero, N.; Gonzalez-Cabre, M.; Sunyer, J. Coarse particles from Saharan Dust and daily mortality. Epidemiology 2008, 19, 800–807. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y.; Chang, C.C.; Chuang, H.Y.; Tsai, S.S.; Wu, T.N.; Ho, C.K. Relationship between air pollution and daily mortality in a subtropical city: Taipei, Taiwan. Environ. Int. 2004, 30, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.S.; Chang, C.C.; Liou, S.H.; Yang, C.Y. The effects of fine particulate air pollution on daily mortality: A case-crossover study in a subtropical city, Taipei, Taiwan. Int. J. Environ. Res. Public Health 2014, 11, 5081–5093. [Google Scholar] [CrossRef] [PubMed]
- Host, S.; Larrieu, S.; Pascal, L.; Blanchard, M.; Declercq, C.; Fabre, P.; Jusot, J.F.; Chardon, B.; Le Tertre, A.; Wagner, V.; et al. Short-term associations between fine and coarse particles and hospital admissions for cardiorespiratory diseases in six French cities. Occup. Environ. Med. 2008, 65, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Adar, S.D.; Filigrana, P.A.; Clements, N.; Peel, J.L. Ambient coarse particulate matter and human health: A systematic review and meta-analysis. Curr. Environ. Health Rep. 2014, 1, 258–274. [Google Scholar] [CrossRef] [PubMed]
- Schins, R.P.; Lightbody, J.H.; Borm, P.J.; Shi, T.M.; Donaldson, K.; Stone, V. Inflammatory effects of coarse and fine particulate matter in relation to chemical and biological constituents. Toxicol. Appl. Pharmacol. 2004, 195, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.; Soukup, J.M.; Sioutas, C.; Cassee, F.R. Response of human alveolar macrophages to ultrafine, fine, and coarse urban air pollution particles. Exp. Lung Res. 2003, 29, 29–44. [Google Scholar] [CrossRef] [PubMed]
- Tong, H.; Cheng, W.Y.; Samet, J.M.; Gilmour, M.I.; Devlin, R.B. Differential cardiopulmonary effects of size-fractionated ambient particulate matter in mice. Cardiovasc. Toxicol. 2010, 10, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Ghio, A.J.; Carraway, M.S.; Madden, M.C. Composition of air pollution particles and oxidative stress in cells, tissues, and living systems. J. Toxicol. Environ. Health Part B. 2012, 15, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Behbod, B.; Urch, B.; Speck, M.; Scott, J.A.; Liu, L.; Poon, R.; Coull, B.; Schwartz, J.; Koutrakis, P.; Silverman, F.; et al. Endotoxin in concentrated coarse and fine ambient particles induce acute systemic inflammation in controlled human exposure. Occup. Environ. Med. 2013, 70, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Graff, D.W.; Cascio, W.E.; Rappold, A.; Zhou, H.B.; Huang, Y.C.; Delvin, R.B. Exposure to concentrated coarse air pollution particles causes mild cardiopulmonary effects in healthy young adults. Environ. Health Perspect. 2009, 117, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Alexis, N.E.; Lay, J.C.; Zeman, K.; Bennett, W.E.; Peden, D.B.; Soukup, J.M.; Devlin, R.B.; Becker, S. Biological material on inhaled coarse fraction particulate matter activates airway phagocytes in vivo in healthy volunteers. J. Allergy Clin. Immunol. 2006, 117, 1396–1403. [Google Scholar] [CrossRef] [PubMed]
- Samet, J.M.; Krewski, D. Health effects associated with exposure to ambient air pollution. J. Toxicol. Environ. Health Part A 2007, 70, 227–242. [Google Scholar] [CrossRef] [PubMed]
- Gong, H.; Linn, W.S.; Terrell, S.L.; Clark, K.W.; Geller, M.D.; Anderson, K.R.; Cascio, W.E.; Sioutas, C. Altered heart-rate variability in asthmatic and healthy volunteers exposed to concentrated ambient coarse particles. Inhal. Toxicol. 2004, 16, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Barbato, A.; Turato, G.; Baraldo, S.; Bazzan, E.; Calabrese, F.; Tura, M.; Zuin, R.; Beghe, B.; Maestrelli, P.; Fabbri, L.M.; et al. Airway inflammation in childhood asthma. Am. J. Respir. Crit. Care Med. 2003, 168, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Brussel, G.G.; Joos, G.F.; Bracke, K.R. New insights into the immunology of chronic obstructive pulmonary disease. Lancet 2011, 378, 1015–1026. [Google Scholar] [CrossRef]
- Schwartz, J.; Marcus, A. Mortality and air pollution in London: A time series analysis. Am. J. Epidemiol. 1990, 131, 185–194. [Google Scholar] [PubMed]
- Zeger, S.L.; Thomas, D.; Dominici, F.; Samet, J.M.; Schwartz, J.; Dockery, D.; Cohen, A. Exposure measurement error in time-series studies of air pollution: Concepts and consequences. Environ. Health Perspect. 2000, 108, 419–426. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | Min | 25% | 50% | 75% | Max | Mean |
|---|---|---|---|---|---|---|
| PM10 (μg/m3) a | 15.33 | 36.26 | 48.01 | 62.28 | 205.35 | 52.07 |
| PM2.5 (μg/m3) a | 8.25 | 19.79 | 27.75 | 37.02 | 117.72 | 30.65 |
| PM2.5–10(μg/m3) a | 2.79 | 14.65 | 19.61 | 24.78 | 144.15 | 21.45 |
| SO2 (ppb) a | 1.12 | 3.07 | 4.05 | 5.35 | 11.14 | 4.32 |
| NO2 (ppb) a | 3.73 | 20.66 | 24.53 | 29.55 | 55.51 | 25.37 |
| CO (ppm) a | 0.15 | 0.53 | 0.66 | 0.82 | 1.73 | 0.70 |
| O3 (ppb) b | 6.98 | 30.19 | 37.76 | 49.64 | 115.43 | 40.63 |
| Temperature (°C) | 9.35 | 19.67 | 24.32 | 28.27 | 32.78 | 23.74 |
| Humidity (%) | 47.92 | 66.95 | 73.21 | 79.28 | 94.19 | 73.02 |
| Total deaths per day | 2 | 11 | 14 | 17 | 32 | 14.29 |
| Respiratory deaths | 0 | 1 | 1 | 2 | 7 | 1.51 |
| Circulatory death | 0 | 2 | 4 | 5 | 11 | 3.93 |
| Variable | PM2.5 | PM2.5–10 | SO2 | NO2 | CO | O3 |
|---|---|---|---|---|---|---|
| PM10 | 0.91 * | 0.83 * | 0.63 * | 0.47 * | 0.45 * | 0.44 * |
| PM2.5 | 1.00 | 0.51 * | 0.61 * | 0.52 * | 0.51 * | 0.44 * |
| PM2.5–10 | - | 1.00 * | 0.47 * | 0.27 * | 0.24 * | 0.32 * |
| SO2 | - | - | 1.00 | 0.49 * | 0.45 * | 0.31 * |
| NO2 | - | - | - | 1.00 | 0.88 * | 0.25 * |
| CO | - | - | - | - | 1.00 | 0.14 * |
| O3 | - | - | - | - | - | 1.00 |
| Temperature | Total Deaths AOR (95% CI) | Respiratory Disease AOR (95% CI) | Circulatory Disease AOR (95% CI) |
|---|---|---|---|
| ≥23 °C (617 days) | |||
| Without adjustment b | 1.11 (1.06–1.17) | 1.11 (0.95–1.29) | 1.10 (1.01–1.21) |
| Adjusted for SO2 | 1.11 (1.06–1.17) | 1.10 (0.97–1.29) | 1.10 (1.00–1.20) |
| Adjusted for NO2 | 1.08 (1.03–1.14) | 1.07 (0.91–1.27) | 1.07 (0.97–1.18) |
| Adjusted for CO | 1.07 (1.02–1.12) | 1.06 (0.90–1.25) | 1.06 (0.97–1.17) |
| Adjusted for O3 | 1.12 (1.07–1.17) | 1.10 (0.94–1.29) | 1.11 (1.01–1.22) |
| <23 °C (479 days) | |||
| Without adjustment b | 1.04 (1.01–1.07) | 1.03 (0.93–1.13) | 1.05 (1.00–1.11) |
| Adjusted for SO2 | 1.05 (1.02–1.09) | 1.04 (0.94–1.16) | 1.07 (1.01–1.14) |
| Adjusted for NO2 | 1.01 (0.98–1.04) | 1.00 (0.91–1.11) | 1.03 (0.97–1.09) |
| Adjusted for CO | 1.02 (0.99–1.05) | 1.02 (0.92–1.13) | 1.03 (0.97–1.10) |
| Adjusted for O3 | 1.04 (1.01–1.07) | 1.03 (0.93–1.13) | 1.06 (1.00–1.11) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, M.-H.; Chiu, H.-F.; Yang, C.-Y. The Effects of Coarse Particles on Daily Mortality: A Case-Crossover Study in a Subtropical City, Taipei, Taiwan. Int. J. Environ. Res. Public Health 2016, 13, 347. https://doi.org/10.3390/ijerph13030347
Cheng M-H, Chiu H-F, Yang C-Y. The Effects of Coarse Particles on Daily Mortality: A Case-Crossover Study in a Subtropical City, Taipei, Taiwan. International Journal of Environmental Research and Public Health. 2016; 13(3):347. https://doi.org/10.3390/ijerph13030347
Chicago/Turabian StyleCheng, Meng-Hsuan, Hui-Fen Chiu, and Chun-Yuh Yang. 2016. "The Effects of Coarse Particles on Daily Mortality: A Case-Crossover Study in a Subtropical City, Taipei, Taiwan" International Journal of Environmental Research and Public Health 13, no. 3: 347. https://doi.org/10.3390/ijerph13030347
APA StyleCheng, M. -H., Chiu, H. -F., & Yang, C. -Y. (2016). The Effects of Coarse Particles on Daily Mortality: A Case-Crossover Study in a Subtropical City, Taipei, Taiwan. International Journal of Environmental Research and Public Health, 13(3), 347. https://doi.org/10.3390/ijerph13030347