
Heavy Physical Work: Cardiovascular Load in Male Construction Workers

Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Compliance with Ethical Standards
2.3. Study Procedure
2.4. Questionnaire
2.4.1. Smoking
2.4.2. Perceived Exhaustion during Work
2.4.3. Work Ability
2.4.4. Perceived Health
2.4.5. Musculoskeletal Disorders
2.4.6. Self-Reported Leisure-Time Physical Activity Level
2.5. Physical Capacity Assessment
2.5.1. Aerobic Fitness
2.5.2. Muscular Strength
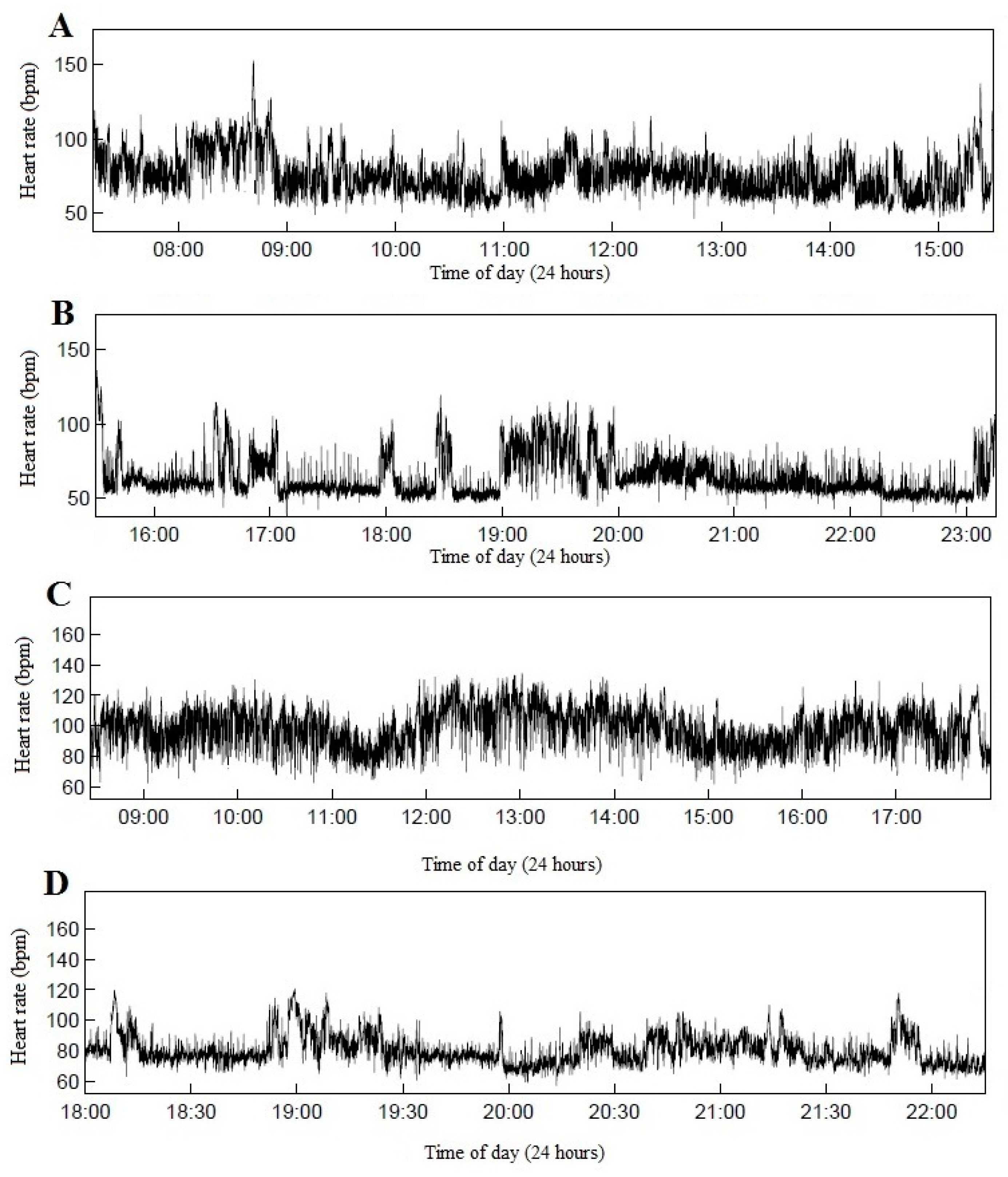
2.6. Assessment of Cardiovascular Load
2.6.1. Instrumentation
2.6.2. Data Processing
2.7. Statistical Analysis
3. Results
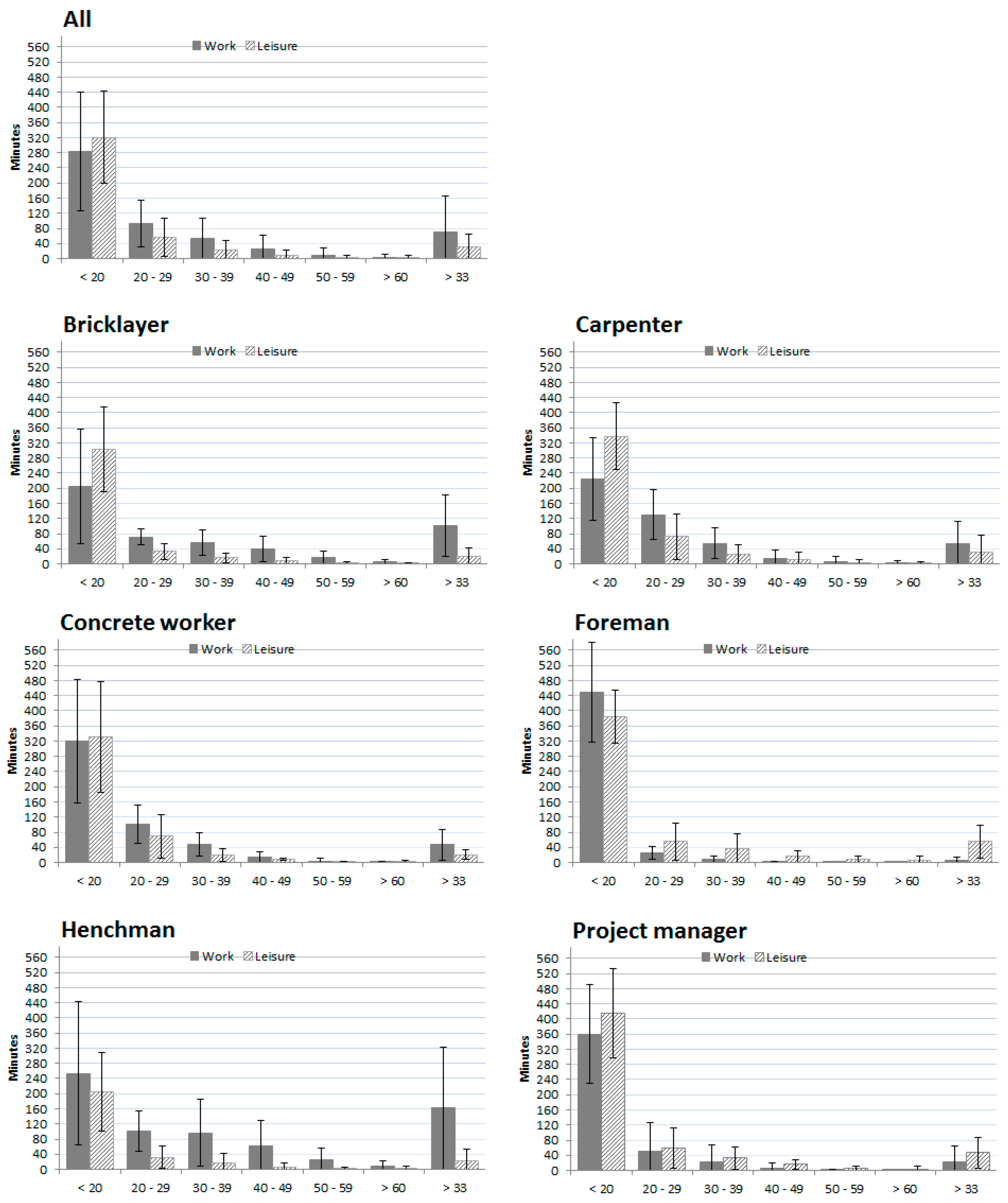
3.1. Cardiovascular Load during Work
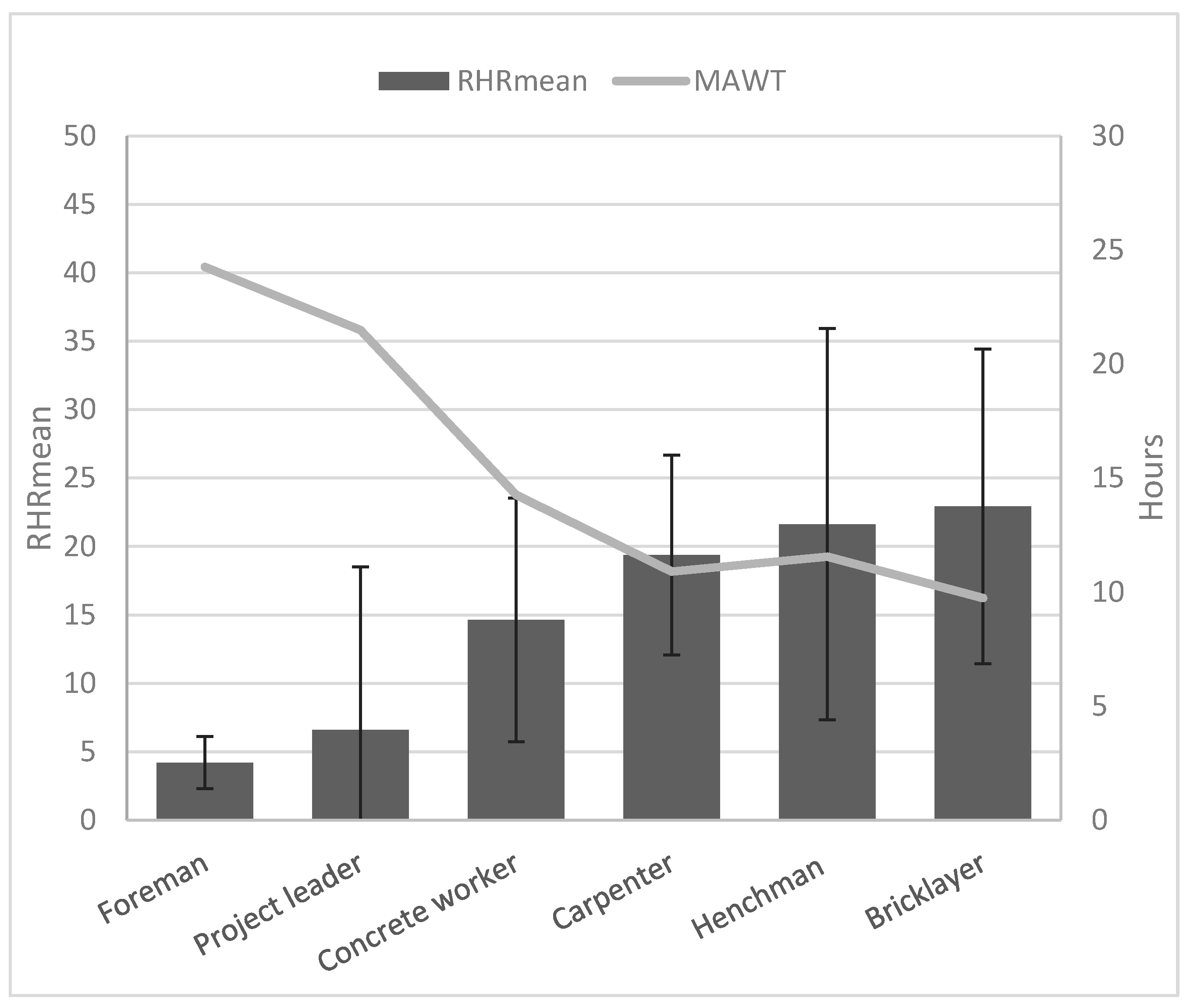
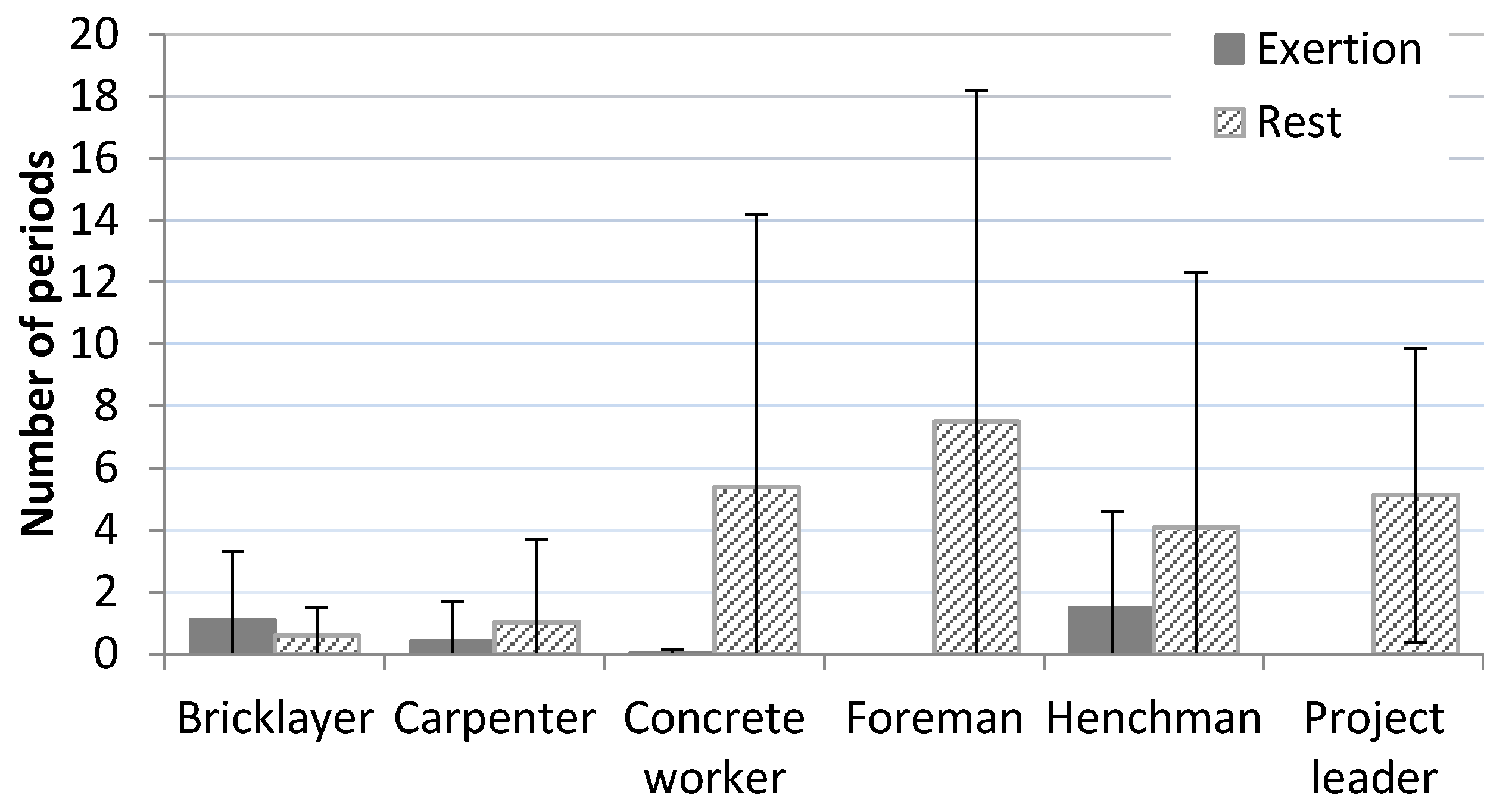
Maximal Acceptable Work Time and Continuous Work and Rest Periods
3.2. Cardiovascular Load during Leisure Time
3.3. Cardiovascular Load and Individual Factors
3.3.1. Age and Seniority
3.3.2. Aerobic Fitness, Leisure Time Physical Activity and Muscular Strength
3.3.3. Work Ability
3.3.4. Musculoskeletal Pain and Perceived Health
3.3.5. Perceived Exhaustion
3.3.6. Smoking
4. Discussion
5. Conclusions
Acknowledgments
Authors Contributions
Conflicts of Interest
References
- Da Costa, B.R.; Vieira, E.R. Risk factors for work-related musculoskeletal disorders: A systematic review of recent longitudinal studies. Am. J. Ind. Med. 2010, 53, 285–323. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, T.I.J.; Elders, L.A.M.; de Zwart, B.C.H.; Burdorf, A. The effects of work-related and individual factors on the Work Ability Index: A systematic review. Occup. Environ. Med. 2009, 66, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Bink, B. The physical working capacity in relation to working time and age. Ergonomics 1962, 5, 25–18. [Google Scholar] [CrossRef]
- Bonjer, F.H. Actual energy expenditure in relation to the physical working capacity. Ergonomics 1962, 5, 29–31. [Google Scholar] [CrossRef]
- Åstrand, P.O.; Rodal, K.; Dahl, H.A.; Strømme, B.S. Applied Work Physiology. In Textbook of Work Physiology, 4th ed.; Human Kinetics Publishers, Inc.: Champaign, IL, USA, 2003; pp. 503–540. [Google Scholar]
- Saha, P.N.; Datta, S.R.; Banerjee, P.K.; Narayane, G.G. An acceptable workload for Indian workers. Ergonomics 1979, 22, 1059–1071. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, S.H.; Kenworth, D.A. Heart rate interpretation methodology. In Ergonomic Design for People at Work; Van Nostrand Reinhold: New York, NY, USA, 1986; pp. 178–179. [Google Scholar]
- Wu, H.C.; Wang, M.J. Relationship between maximum acceptable work time and physical workload. Ergonomics 2002, 45, 280–289. [Google Scholar] [CrossRef] [PubMed]
- Boschman, J.S.; van der Molen, H.F.; Sluiter, J.K.; Frings-Dresen, M.H.W. Musculoskeletal disorders among construction workers: A one-year follow-up study. BMC Musculoskelet. Disord. 2012, 13, 196. [Google Scholar] [CrossRef] [PubMed]
- Stocks, S.J.; Turner, S.; McNamee, R.; Carder, M.; Hussey, L.; Agius, R.M. Occupation and work-related ill-health in UK construction workers. Occup. Med. 2011, 61, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Onder, G.; Cesari, M.; Zamboni, V.; Barillaro, C.; Capoluongo, E.; Pahor, M.; Bernabei, R.; Landi, F.; Ferrucci, L. Lifetime occupation and physical function: A prospective cohort study on persons aged 80 years and older living in a community. Occup. Environ. Med. 2006, 63, 438–442. [Google Scholar] [CrossRef] [PubMed]
- Cassou, B.; Derriennic, F.; Iwatsubo, Y.; Amphoux, M. Physical diability after retirement and occupational risk factors during working life: A cross sectional epidemiological study in the Paris area. J. Epidemiol. Community Health 1992, 46, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Li, C.Y.; Wu, S.C.; Wen, S.W. Longest held occupation in a lifetime and risk of disability in activities of daily living. Occup. Environ. Med. 2000, 57, 550–554. [Google Scholar] [CrossRef] [PubMed]
- Kwak, L.; Proper, K.I.; Hagströmer, M.; Sjöström, M. The repeatability and validity of questionnaires assessing occupational physical activity—A systematic review. Scand. J. Work Environ. Health 2011, 37, 6–29. [Google Scholar] [CrossRef] [PubMed]
- Van der Molen, H.F.; Mol, E.; Kuijer, P.P.; Frings-Dresen, M.H. The evaluation of smaller plasterboards on productivity, work demands and workload in construction workers. Appl. Ergon. 2007, 38, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Van Der Molen, H.F.; Kuijer, P.P.; Hopmans, P.P.; Houweling, A.G.; Faber, G.S.; Hoozemans, M.J.; Frings-Dresen, M.H. Effect of block weight on work demands and physical workload during masonry work. Ergonomics 2008, 51, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Van der Molen, H.F.; Kuijer, P.P.F.M.; Formanoy, M.; Bron, L.; Hoozemans, M.J.M.; Visser, B.; Frings-Dresen, M.H.W. Evaluation of three ergonomic measures on productivity, physical work demands, and workload in gypsum bricklayers. Am. J. Ind. Med. 2010, 53, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Korshøj, M.; Krustrup, P.; Jespersen, T.; Søgaard, K.; Skotte, J.H.; Holtermann, A. A 24-h assessment of physical activity and cardio-respiratory fitness among female hospital cleaners: A pilot study. Ergonomics 2013, 56, 935–943. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Jensen, B.S.; Sogaard, K.; Carneiro, I.G.; Christiansen, C.S.; Hanisch, C.; Holtermann, A. Face validity of the single work ability item: Comparison with objectively measured heart rate reserve over several days. Int. J. Environ. Res. Public Health 2014, 11, 5333–5348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alavinia, S.M.; van Duivenbooden, C.; Burdorf, A. Influence of work-related factors and individual characteristics on work ability among Dutch construction workers. Scand. J. Work Environ. Health 2007, 33, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Strijk, J.E.; Proper, K.I.; van Stralen, M.M.; Wijngaard, P.; van Mechelen, W.; van der Beek, A.J. The role of work ability in the relationship between aerobic capacity and sick leave: A mediation analysis. Occup. Environ. Med. 2011, 68, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Arvidson, E.; Börjesson, M.; Ahlborg, G., Jr.; Lindegård, A.; Jonsdottir, I.H. The level of leisure time physical activity is associated with work ability—A cross sectional and prospective study of health care workers. BMC Public Health 2013, 13, 855. [Google Scholar] [CrossRef] [PubMed]
- Schibye, B.; Hansen, A.F.; Sogaard, K.; Christensen, H. Aerobic power and muscle strength among young and elderly workers with and without physically demanding work tasks. Appl. Ergon. 2001, 32, 425–431. [Google Scholar] [CrossRef]
- Torgén, M.; Punnett, L.; Alfredsson, L.; Kilbom, Å. Physical capacity in relation to present and past physical load at work: A study of 484 men and women aged 41 to 58 years. Am. J. Ind. Med. 1999, 36, 388–400. [Google Scholar] [CrossRef]
- Nygård, C.H.; Kilbom, Å.; Hjelm, E.W.; Winkel, J.; Group, S.M.S. Lifetime occupational exposure to heavy work and individual physical capacity. Int. J. Ind. Ergon. 1994, 14, 365–372. [Google Scholar] [CrossRef]
- Savinainen, M.; Nygård, C.-H.; Ilmarinen, J. A 16-year follow-up study of physical capacity in relation to perceived workload among ageing employees. Ergonomics 2004, 47, 1087–1102. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Fransson, E.I.; Heikkilä, K.; Nyberg, S.T.; Zins, M.; Westerlund, H.; Westerholm, P.; Väänänen, A.; Virtanen, M.; Vahtera, J.; Theorell, T.; et al. Job Strain as a Risk Factor for Leisure-Time Physical Inactivity: An Individual-Participant Meta-Analysis of Up to 170,000 Men and Women: The IPD-Work Consortium. Am. J. Epidemiol. 2012, 176, 1078–1089. [Google Scholar] [CrossRef] [PubMed]
- Karvonen, J.; Vuorimaa, T. Heart rate and exercise intensity during sports activities. Practical application. Sports Med. 1988, 5, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef]
- Noble, B.J.; Borg, G.A.V.; Jacobs, I.; Ceci, R.; Kaiser, P. A category-ratio perceived exertion scale: Relationship to blood and muscle lactates and heart rate. Med. Sci. Sports Exerc. 1983, 15, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Ahlstrom, L.; Grimby-Ekman, A.; Hagberg, M.; Dellve, L. The work ability index and single-item question: Associations with sick leave, symptoms, and health—A prospective study of women on long-term sick leave. Scand. J. Work Environ. Health 2010, 36, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr. SF-36 health survey update. Spine 2000, 25, 3130–3139. [Google Scholar] [CrossRef] [PubMed]
- Steingrímsdóttir, Ó.A.; Vøllestad, N.K.; Røe, C.; Knardahl, S. Variation in reporting of pain and other subjective health complaints in a working population and limitations of single sample measurements. Pain 2004, 110, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Saltin, B.; Grimby, G. Physiological analysis of middle-aged and old former athletes. Comparison with still active athletes of the same ages. Circulation 1968, 38, 1104–1115. [Google Scholar] [CrossRef] [PubMed]
- Åstrand, P.O.; Rodahl, K.; Dahl, H.A.; Strømme, B.S. Evaluation of physical performance on the basis of tests. In Textbook of Work Physiology, 4th ed.; Human Kinetics Publishers, Inc.: Champaign, IL, USA, 2003; pp. 283–284. [Google Scholar]
- Åstrand, P.O.; Ryhming, I. A nomogram for calculation of aerobic capacity (physical fitness) from pulse rate during sub-maximal work. J. Appl. Physiol. 1954, 7, 218–221. [Google Scholar] [PubMed]
- Essendrop, M.; Schibye, B.; Hansen, K. Reliability of isometric muscle strength tests for the trunk, hands and shoulders. Int. J. Ind. Ergon. 2001, 28, 379–387. [Google Scholar] [CrossRef]
- Brage, S.; Brage, N.; Ekelund, U.; Luan, J.; Franks, P.W.; Froberg, K.; Wareham, N.J. Effect of combined movement and heart rate monitor placement on physical activity estimates during treadmill locomotion and free-living. Eur. J. Appl. Physiol. 2006, 96, 517–524. [Google Scholar] [CrossRef] [PubMed]
- The Nord Trøndelag Health Study. Availiable online: https://www.ntnu.edu/hunt/databank (accessed on 10 January 2016).
- Boschman, J.S.; van der Molen, H.F.; Sluiter, J.K.; Frings-Dresen, M.H.W. Occupational demands and health effects for bricklayers and construction supervisors: A systematic review. Am. J. Ind. Med. 2011, 54, 55–77. [Google Scholar] [CrossRef] [PubMed]
- Karlqvist, L.; Leijon, O.; Härenstam, A. Physical demands in working life and individual physical capacity. Eur. J. Appl. Physiol. 2003, 89, 536–547. [Google Scholar] [CrossRef] [PubMed]
- Drain, J.; Billing, D.; Neesham-Smith, D.; Aisbett, B. Predicting physiological capacity of human load carriage—A review. Appl. Ergon. 2016, 52, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Holtermann, A.; Hansen, J.V.; Burr, H.; Sogaard, K.; Sjogaard, G. The health paradox of occupational and leisure-time physical activity. Br. J. Sports Med. 2012, 46, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Hubscher, M.; Ferreira, M.L.; Junqueira, D.R.; Refshauge, K.M.; Maher, C.G.; Hopper, J.L.; Ferreira, P.H. Heavy domestic, but not recreational, physical activity is associated with low back pain: Australian Twin low BACK pain (AUTBACK) study. Eur. Spine J. 2014, 23, 2083–2089. [Google Scholar] [CrossRef] [PubMed]
- Pollock, M.L. The quantification of endurance training programs. Exerc. Sport Sci. Rev. 1973, 1, 155–188. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, J. Work and cardiovascular health: Viewpoint of occupational physiology. Ann. Med. 1989, 21, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Krause, N. Physical activity and cardiovascular mortality—Disentangling the roles of work, fitness, and leisure. Scand. J. Work Environ. Health 2010, 36, 349–355. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Technical | Questionnaire | Profession | Technical | Questionnaire |
|---|---|---|---|---|---|
| n = 42 | n = 255 | n = 42 | n = 255 | ||
| Mean (SD) | Mean (SD) | Number (%) | Number (%) | ||
| Age (years) | 40.4 (13.6) | 42.7 (12.9) | Project manager | 5 (11.9) | 52 (20.4) |
| Male gender (frequency and %) a | 42 (100%) * | 237 (93%) | Carpenter | 12 (28.6) | 70 (27.5) |
| Height (cm) | 179.1 (6.2) | 179.6 (7.1) | Bricklayer | 5 (11.9) | 11 (4.3) |
| Body mass (kg) | 82.5 (11.5) | 85.2 (12.9) | Concrete worker | 8 (19.0) | 41 (16.1) |
| Body mass index (kg/m2) | 25.8 (3.5) | 26.4 (4.0) | Henchman | 7 (16.7) | 13 (5.1) |
| Normal work hours per week | 37.7 (4.9) | 38.4 (3.7) | Foreman | 4 (9.5) | 26 (10.2) |
| Smokers (frequency and %) a | 13 (31%) * | 46 (18%) | Working with various tasks | 1 (2.4) | 16 (6.3) |
| Perceived health (1–5) | 2.6 (0.9) | 2.6 (0.9) | Driver | 0 (0) | 9 (3.5) |
| Waist circumference (cm) | 93.1 (10.4) | NA | Missing | 0 (0) | 17 (6.7) |
| HRmax (bpm) | 179.7 (9.5) | NA | Total | 42 (100) | 255 (100) |
| HRmin (bpm) | 68.7 (0.5) | NA | |||
| Estimated O2max (L·min−1) | 3.1 (0.9) | NA | |||
| Estimated O2max (mL·kg−1·min−1) | 38 .4 (10.7) | NA | |||
| Handstrength (kg) | 54.6 (8.9) | NA | |||
| Blood pressure systolic (mmHg) | 135.2 (12.1) | NA | |||
| Blood pressure diastolic (mmHg) | 78.9 (9.2) | NA |
| Continuously ≥ 5 min | Continuously ≥ 10 min | Continuously ≥ 15 min | |
|---|---|---|---|
| Mean number of episodes | |||
| >0 times | 7 persons (16.7%) | 5 persons (11.9%) | 1 person (2.4%) |
| ≥ 3 times | 3 persons (7.1%) | 0 persons (0%) | 0 persons (0%) |
| ≥ 5 times | 2 persons (4.8%) | 0 persons (0%) | 0 persons (0%) |
| Variable | Unadjusted | Adjusted a | ||
|---|---|---|---|---|
| Beta | p-Value | Beta | p-Value | |
| Age (years) | −0.298 | 0.021 | −0.414 | 0.002 |
| Body mass index (kg/m2) | −0.266 | 0.613 | Not included | Not included |
| Seniority (years) b | −0.234 | 0.085 | Not included | Not included |
| Smoking | 1.390 | 0.377 | Not included | Not included |
| Estimated O2max (L·min−1) | −5.924 | 0.002 | −5.098 | 0.008 |
| Physical activity (1–4) | −3.205 | 0.109 | −2.025 | 0.304 |
| Hand strength (kg) | 0.169 | 0.401 | Not included | Not included |
| Work ability | −1.844 | 0.076 | −0.255 | 0.800 |
| Musculoskeletal pain | 0.569 | 0.617 | Not included | Not included |
| Perceived exhaustion at work | 1.598 | 0.043 | 0.713 | 0.288 |
| Perceived health | 1.802 | 0.346 | Not included | Not included |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lunde, L.-K.; Koch, M.; Veiersted, K.B.; Moen, G.-H.; Wærsted, M.; Knardahl, S. Heavy Physical Work: Cardiovascular Load in Male Construction Workers. Int. J. Environ. Res. Public Health 2016, 13, 356. https://doi.org/10.3390/ijerph13040356
Lunde L-K, Koch M, Veiersted KB, Moen G-H, Wærsted M, Knardahl S. Heavy Physical Work: Cardiovascular Load in Male Construction Workers. International Journal of Environmental Research and Public Health. 2016; 13(4):356. https://doi.org/10.3390/ijerph13040356
Chicago/Turabian StyleLunde, Lars-Kristian, Markus Koch, Kaj Bo Veiersted, Gunn-Helen Moen, Morten Wærsted, and Stein Knardahl. 2016. "Heavy Physical Work: Cardiovascular Load in Male Construction Workers" International Journal of Environmental Research and Public Health 13, no. 4: 356. https://doi.org/10.3390/ijerph13040356
APA StyleLunde, L. -K., Koch, M., Veiersted, K. B., Moen, G. -H., Wærsted, M., & Knardahl, S. (2016). Heavy Physical Work: Cardiovascular Load in Male Construction Workers. International Journal of Environmental Research and Public Health, 13(4), 356. https://doi.org/10.3390/ijerph13040356