
Identification of Haplotype Tag Single-Nucleotide Polymorphisms within the PPAR Family Genes and Their Clinical Relevance in Patients with Major Trauma

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical Evaluation
2.3. SNP Selection
2.4. Genotyping of Selected SNPs
2.5. Ex Vivo Tumor Necrosis Factor α Production
2.6. Statistical Analysis
3. Results
3.1. Construction of Haplotype Blocks and Selection of SNPs
3.2. Allele Frequencies and Genotype Distribution of the Selected SNPs among Trauma Patients
3.3. Overall Clinical Characteristics of Patients with Major Trauma
3.4. Clinical Relevance of the Nine Selected SNPs with Development of Sepsis and MODS in Trauma Patients
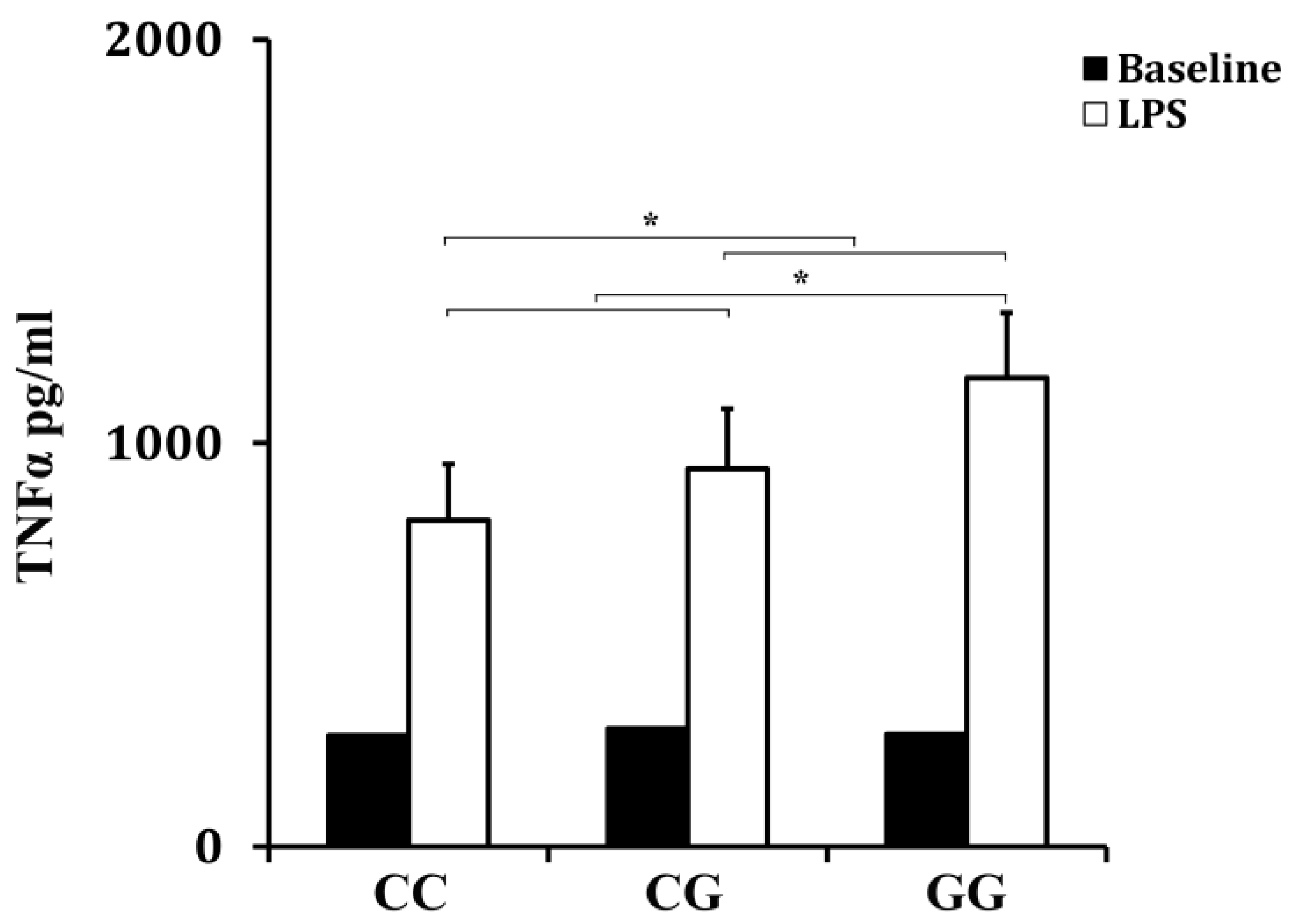
3.5. Effect of rs10865710 on LPS-Induced TNFα Production
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| PPAR | peroxisome proliferator-activated receptor |
| iMLDR | improved multiplex ligation detection reaction |
| MOD | multiple organ dysfunction |
| TNFα | tumor necrosis factor α |
| LPS | lipopolysaccharides |
| MODS | multiple organ dysfunction syndrome |
| RXR | retinoid X receptor |
| PPRE | PPAR response element |
| SNP | single-nucleotide polymorphism |
| CHB | Chinese Han Beijing |
| ISS | Injury Severity Score |
| HWE | Hardy–Weinberg equilibrium |
| OR | odds ratio |
| IL-1β | interleukin-1 beta |
References
- Wang, Z.; Jiang, J. An overview of research advances in road traffic trauma in China. Traffic Inj. Prev. 2003, 4, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Kersten, S.; Desvergne, B.; Wahli, W. Roles of ppars in health and disease. Nature 2000, 405, 421–424. [Google Scholar] [PubMed]
- Kota, B.P.; Huang, T.H.; Roufogalis, B.D. An overview on biological mechanisms of ppars. Pharmacol. Res. 2005, 51, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.D.; Plutzky, J. Peroxisome proliferator-activated receptors as transcriptional nodal points and therapeutic targets. Circulation 2007, 115, 518–533. [Google Scholar] [CrossRef] [PubMed]
- Pawlak, M.; Lefebvre, P.; Staels, B. Molecular mechanism of pparalpha action and its impact on lipid metabolism, inflammation and fibrosis in non-alcoholic fatty liver disease. J. Hepatol. 2015, 62, 720–733. [Google Scholar] [CrossRef] [PubMed]
- Das, S.K.; Chakrabarti, R. Role of ppar in cardiovascular diseases. Recent Pat. Cardiovasc. Drug Discov. 2006, 1, 193–209. [Google Scholar] [CrossRef] [PubMed]
- Janani, C.; Ranjitha Kumari, B.D. Ppar gamma gene—A review. Diabetes Metab. Syndr. 2015, 9, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Giordano Attianese, G.M.; Desvergne, B. Integrative and systemic approaches for evaluating pparbeta/delta (ppard) function. Nucl. Recept. Signal. 2015, 13, e001. [Google Scholar] [PubMed]
- Annese, V.; Rogai, F.; Settesoldi, A.; Bagnoli, S. Ppargamma in inflammatory bowel disease. PPAR Res. 2012, 2012, 620839. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Chu, E.S.; Zhang, J.; Li, X.; Liang, Q.; Chen, J.; Chen, M.; Teoh, N.; Farrell, G.; Sung, J.J.; et al. Peroxisome proliferator activated receptor alpha inhibits hepatocarcinogenesis through mediating nf-kappab signaling pathway. Oncotarget 2014, 5, 8330–8340. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Kume, S.; Tanaka, Y.; Isshiki, K.; Araki, S.; Chin-Kanasaki, M.; Sugimoto, T.; Koya, D.; Haneda, M.; Sugaya, T.; et al. Gw501516, a ppardelta agonist, ameliorates tubulointerstitial inflammation in proteinuric kidney disease via inhibition of tak1-nfkappab pathway in mice. PLoS ONE 2011, 6, e25271. [Google Scholar]
- Yao, J.; Pan, D.; Zhao, Y.; Zhao, L.; Sun, J.; Wang, Y.; You, Q.D.; Xi, T.; Guo, Q.L.; Lu, N. Wogonin prevents lipopolysaccharide-induced acute lung injury and inflammation in mice via peroxisome proliferator-activated receptor gamma-mediated attenuation of the nuclear factor-kappab pathway. Immunology 2014, 143, 241–257. [Google Scholar] [CrossRef] [PubMed]
- Bao, X.C.; Fang, Y.Q.; You, P.; Zhang, S.; Ma, J. Protective role of peroxisome proliferator-activated receptor beta/delta in acute lung injury induced by prolonged hyperbaric hyperoxia in rats. Respir. Physiol. Neurobiol. 2014, 199, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Jeon, Y.; Jung, Y.; Kim, M.C.; Kwon, H.C.; Kang, K.S.; Kim, Y.K.; Kim, S.N. Sargahydroquinoic acid inhibits tnfalpha-induced ap-1 and nf-kappab signaling in hacat cells through pparalpha activation. Biochem. Biophys. Res. Commun. 2014, 450, 1553–1559. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.F.; Zhang, H. Nfkb and nfkbi polymorphisms in relation to susceptibility of tumour and other diseases. Histol. Histopathol. 2007, 22, 1387–1398. [Google Scholar] [PubMed]
- Zeng, L.; Du, J.; Gu, W.; Zhang, A.Q.; Wang, H.Y.; Wen, D.L.; Qiu, L.; Yang, X.T.; Sun, J.H.; Zhang, M.; et al. Rs1800625 in the receptor for advanced glycation end products gene predisposes to sepsis and multiple organ dysfunction syndrome in patients with major trauma. Crit. Care 2015, 19, 6. [Google Scholar] [CrossRef] [PubMed]
- Pan, W.; Zhang, A.Q.; Gu, W.; Gao, J.W.; Du, D.Y.; Zhang, L.Y.; Zeng, L.; Du, J.; Wang, H.Y.; Jiang, J.X. Identification of haplotype tag snps within the nuclear factor-kappab family genes and their clinical relevance in patients with major trauma. Crit. Care 2015, 19, 95. [Google Scholar] [CrossRef] [PubMed]
- West, S.D.; Ziegler, A.; Brooks, T.; Krencicki, M.; Myers, O.; Mold, C. An fcgammariia polymorphism with decreased c-reactive protein binding is associated with sepsis and decreased monocyte hla-dr expression in trauma patients. J. Trauma Acute Care Surg. 2015, 79, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Burke, R.V.; Jeon, C.Y.; Chang, S.C.; Chang, P.Y.; Morgenstern, H.; Tashkin, D.P.; Mao, J.; Cozen, W.; Mack, T.M.; et al. Polymorphisms of peroxisome proliferator-activated receptors and survival of lung cancer and upper aero-digestive tract cancers. Lung Cancer 2014, 85, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Frazier-Wood, A.C.; Ordovas, J.M.; Straka, R.J.; Hixson, J.E.; Borecki, I.B.; Tiwari, H.K.; Arnett, D.K. The ppar alpha gene is associated with triglyceride, low-density cholesterol and inflammation marker response to fenofibrate intervention: The goldn study. Pharmacogenom. J. 2013, 13, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Ma, G.; Wang, H.; Mo, G.; Cui, L.; Li, Y.; Shao, Y.; Liu, X.; Xie, Y.; Li, J.; Fu, J.; et al. The pro12ala polymorphism of ppar-gamma gene is associated with sepsis disease severity and outcome in chinese han population. PPAR Res. 2014, 2014, 701971. [Google Scholar] [CrossRef] [PubMed]
- Association for the Advancement of Automotive Medicine. The Abbreviated Injury Scale; AAAM: Barrington, IL, USA, 2005. [Google Scholar]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.L.; Ramsay, G.; et al. 2001 sccm/esicm/accp/ats/sis international sepsis definitions conference. Crit. Care Med 2003, 31, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.C.; Cook, D.J.; Christou, N.V.; Bernard, G.R.; Sprung, C.L.; Sibbald, W.J. Multiple organ dysfunction score: A reliable descriptor of a complex clinical outcome. Crit. Care Med. 1995, 23, 1638–1652. [Google Scholar] [CrossRef] [PubMed]
- Genebank. Available online: http://www.Ncbi.Nlm.Nih.Gov/genbank/ (accessed on 24 January 2015).
- Barrett, J.C.; Fry, B.; Maller, J.; Daly, M.J. Haploview: Analysis and visualization of ld and haplotype maps. Bioinformatics 2005, 21, 263–265. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, S.B.; Schaffner, S.F.; Nguyen, H.; Moore, J.M.; Roy, J.; Blumenstiel, B.; Higgins, J.; DeFelice, M.; Lochner, A.; Faggart, M.; et al. The structure of haplotype blocks in the human genome. Science 2002, 296, 2225–2229. [Google Scholar] [CrossRef] [PubMed]
- Dai, Q.; Wei, H.L.; Huang, J.; Zhou, T.J.; Chai, L.; Yang, Z.H. Kras polymorphisms are associated with survival of crc in chinese population. Tumour Biol. 2015. [Google Scholar] [CrossRef] [PubMed]
- PowerSampleSize. Available online: http://biostat.Mc.Vanderbilt.Edu/wiki/Main/PowerSampleSize (accessed on 24 February 2015).
- Zingarelli, B.; Sheehan, M.; Hake, P.W.; O’Connor, M.; Denenberg, A.; Cook, J.A. Peroxisome proliferator activator receptor-gamma ligands, 15-deoxy-delta(12,14)-prostaglandin j2 and ciglitazone, reduce systemic inflammation in polymicrobial sepsis by modulation of signal transduction pathways. J. Immunol. 2003, 171, 6827–6837. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Zhou, G.; Zeng, Z. Effects of peroxisome proliferator-activated receptor-beta/delta on sepsis induced acute lung injury. Chin. Med. J. 2014, 127, 2129–2137. [Google Scholar] [PubMed]
- Meirhaeghe, A.; Fajas, L.; Gouilleux, F.; Cottel, D.; Helbecque, N.; Auwerx, J.; Amouyel, P. A functional polymorphism in a stat5b site of the human ppar gamma 3 gene promoter affects height and lipid metabolism in a french population. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 289–294. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Gene | rs Number | Location | Variation | MAF 1 (%) | Region |
|---|---|---|---|---|---|
| PPARα | rs135551 | 6523 | G/A | 8.4 | Intron 2 |
| rs5769178 | 14776 | A/C | 15.7 | Intron 2 | |
| rs4253711 | 48535 | G/A | 15.6 | Intron 3 | |
| rs4823613 | 51809 | A/G | 21.7 | Intron 3 | |
| PPARβ | rs6902123 | 20087 | T/C | 5.6 | Intron 2 |
| rs2016520 | 68444 | T/C | 26.3 | 5′-UTR | |
| PPARγ | rs4684846 | 9501 | G/A | 46.0 | Intron 1 |
| rs10865710 | 23850 | C/G | 34.9 | Extron A2 | |
| rs1822825 | 120615 | G/A | 45.3 | Intron 5 |
| SNPs | Number | MAF 1 (%) | Genotypes, Number (%) | HWE 3 Test | |||
|---|---|---|---|---|---|---|---|
| Patients | Database 2 | Wild-Type | Heterozygous | Variant | |||
| rs135551 | 734 | 7.6 | 8.4 | 628 (85.6) | 101 (13.8) | 5 (0.6) | 0.67 |
| rs5769178 | 734 | 15.0 | 15.7 | 525 (71.5) | 198 (27.0) | 11 (1.5) | 0.11 |
| rs4253711 | 734 | 14.4 | 15.6 | 543 (74.0) | 170 (23.2) | 21 (2.8) | 0.09 |
| rs4823613 | 734 | 23.2 | 21.7 | 436 (59.4) | 256 (34.9) | 42 (5.7) | 0.59 |
| rs6902123 | 734 | 3.1 | 5.6 | 690 (94.0) | 42 (5.7) | 2 (0.3) | 0.12 |
| rs2016520 | 734 | 30.4 | 26.3 | 357 (48.6) | 308 (42.0) | 69 (9.4) | 0.83 |
| rs4684846 | 727 | 45.8 | 46.0 | 208 (28.6) | 372 (51.2) | 147 (20.2) | 0.41 |
| rs10865710 | 734 | 34.6 | 34.9 | 316 (43.1) | 328 (44.7) | 90 (12.2) | 0.73 |
| rs1822825 | 732 | 45.5 | 45.3 | 215 (29.4) | 368 (50.3) | 149 (20.3) | 0.71 |
| Clinical Characteristics | Patient Data (n = 734) |
|---|---|
| Mean age ± SD, years | 41.3 ± 12.1 |
| Age range, years | 18–65 |
| Males/females, n | 591/143 |
| Mean ISS 1 ± SD | 22.3 ± 9.4 |
| ≥16 to <25, n | 435 |
| ≥25, n | 299 |
| Injured body regions, n | |
| Head | 391 |
| Thorax | 473 |
| Abdomen | 280 |
| Extremities | 436 |
| Number of regions injured, n | |
| Two | 272 |
| Three | 188 |
| All four | 66 |
| Organ dysfunction, n (%) | 374 (51.0%) |
| One, n | 258 |
| Two, n | 95 |
| Three or above, n | 21 |
| Sepsis, n (%) | 300 (40.9%) |
| Source of infection (%) | |
| Respiratory tract infection | 46.4 |
| Primary bloodstream infection | 19.6 |
| Urinary tract infection | 14.9 |
| Catheter-associated infection | 9.5 |
| Wound infection | 7.2 |
| Others 2 | 2.4 |
| Pathogens (positive blood cultures), % | |
| Gram-negative | 21.7 |
| Gram-positive | 11.3 |
| Fungi | 3.3 |
| Mixed Gram-negative and Gram-positive | 9.7 |
| Negative blood cultures | 54.0 |
| SNPs | Genotype | Number | Age, Years | Sex, Male/Female, n | ISS 1 | Sepsis, n | MOD 2 Score |
|---|---|---|---|---|---|---|---|
| rs135551 | AA | 5 | 40.8 ± 16.6 | 3/2 | 15.6 ± 3.8 | 2 | 4.0 ± 2.2 |
| AG | 101 | 40.0 ± 11.7 | 87/14 | 21.3 ± 8.1 | 36 | 4.5 ± 2.2 | |
| GG | 628 | 41.4 ± 12.1 | 501/127 | 22.5 ± 9.6 | 262 | 4.9 ± 2.6 | |
| rs5769178 | AA | 525 | 40.9 ± 12.6 | 429/96 | 21.8 ± 9.3 | 209 | 4.8 ± 2.5 |
| AC | 198 | 42.5 ± 10.6 | 156/42 | 23.3 ± 9.1 | 86 | 4.9 ± 2.6 | |
| CC | 11 | 34.9 ± 7.6 | 6/5 | 28.9 ± 15.8 | 5 | 5.4 ± 2.7 | |
| rs4253711 | AA | 21 | 40.1 ± 14.2 | 16/5 | 23.3 ± 12.9 | 7 | 4.5 ± 2.1 |
| AG | 170 | 40.4 ± 11.5 | 132/38 | 22.3 ± 8.8 | 62 | 4.7 ± 2.5 | |
| GG | 543 | 41.6 ± 12.2 | 443/100 | 22.3 ± 9.5 | 231 | 4.9 ± 2.5 | |
| rs4823613 | AA | 436 | 41.5 ± 12.1 | 351/85 | 22.2 ± 9.6 | 186 | 5.0 ± 2.5 |
| AG | 256 | 41.2 ± 12.0 | 207/49 | 22.4 ± 9.1 | 100 | 4.9 ± 2.5 | |
| GG | 42 | 39.1 ± 12.9 | 33/9 | 22.8 ± 9.5 | 14 | 5.1 ± 2.6 | |
| rs6902123 | CC | 2 | 41.2 ± 5.7 | 2/0 | 25.0 ± 4.2 | 1 | 5.5 ± 2.1 |
| CT | 42 | 40.5 ± 12.0 | 31/11 | 21.1 ± 8.4 | 16 | 3.9 ± 1.8 | |
| TT | 690 | 41.3 ± 12.1 | 558/132 | 22.4 ± 9.5 | 283 | 4.9 ± 2.5 | |
| rs2016520 | CC | 69 | 41.7 ± 10.9 | 53/13 | 22.5 ± 8.9 | 25 | 4.6 ± 2.5 |
| CT | 308 | 41.1 ± 12.0 | 243/65 | 22.3 ± 9.9 | 131 | 4.8 ± 2.4 | |
| TT | 357 | 41.3 ± 12.4 | 292/65 | 22.2 ± 9.1 | 144 | 5.0 ± 2.6 | |
| rs4684846 | AA | 147 | 41.0 ± 11.6 | 117/30 | 23.1 ± 9.1 | 63 | 5.3 ± 2.7 |
| AG | 372 | 41.1 ± 12.4 | 302/70 | 22.0 ± 9.4 | 146 | 4.7 ± 2.3 | |
| GG | 208 | 41.8 ± 11.9 | 166/42 | 22.2 ± 9.8 | 89 | 5.0 ± 2.7 | |
| rs10865710 | CC | 316 | 41.0 ± 11.9 | 257/59 | 22.3 ± 10.0 | 116 | 4.9 ± 2.5 |
| CG | 328 | 41.3 ± 12.3 | 263/65 | 22.3 ± 9.0 | 134 | 4.6 ± 2.3 | |
| GG | 90 | 41.9 ± 12.0 | 71/19 | 22.4 ± 9.0 | 50 | 5.8 ± 3.0 | |
| a1, b1 | a2 | ||||||
| rs1822825 | AA | 149 | 41.9 ± 11.9 | 117/32 | 21.1 ± 9.3 | 60 | 4.9 ± 2.4 |
| AG | 368 | 40.9 ± 12.2 | 299/69 | 22.6 ± 9.1 | 156 | 4.8 ± 2.6 | |
| GG | 215 | 41.4 ± 12.1 | 174/41 | 22.6 ± 10.1 | 83 | 4.9 ± 2.4 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, J.-W.; Zeng, L.; Zhang, A.-Q.; Wang, X.; Pan, W.; Du, D.-Y.; Zhang, L.-Y.; Gu, W.; Jiang, J.-X. Identification of Haplotype Tag Single-Nucleotide Polymorphisms within the PPAR Family Genes and Their Clinical Relevance in Patients with Major Trauma. Int. J. Environ. Res. Public Health 2016, 13, 374. https://doi.org/10.3390/ijerph13040374
Gao J-W, Zeng L, Zhang A-Q, Wang X, Pan W, Du D-Y, Zhang L-Y, Gu W, Jiang J-X. Identification of Haplotype Tag Single-Nucleotide Polymorphisms within the PPAR Family Genes and Their Clinical Relevance in Patients with Major Trauma. International Journal of Environmental Research and Public Health. 2016; 13(4):374. https://doi.org/10.3390/ijerph13040374
Chicago/Turabian StyleGao, Jun-Wei, Ling Zeng, An-Qiang Zhang, Xiao Wang, Wei Pan, Ding-Yuan Du, Lian-Yang Zhang, Wei Gu, and Jian-Xin Jiang. 2016. "Identification of Haplotype Tag Single-Nucleotide Polymorphisms within the PPAR Family Genes and Their Clinical Relevance in Patients with Major Trauma" International Journal of Environmental Research and Public Health 13, no. 4: 374. https://doi.org/10.3390/ijerph13040374
APA StyleGao, J. -W., Zeng, L., Zhang, A. -Q., Wang, X., Pan, W., Du, D. -Y., Zhang, L. -Y., Gu, W., & Jiang, J. -X. (2016). Identification of Haplotype Tag Single-Nucleotide Polymorphisms within the PPAR Family Genes and Their Clinical Relevance in Patients with Major Trauma. International Journal of Environmental Research and Public Health, 13(4), 374. https://doi.org/10.3390/ijerph13040374