
Structural Factors Affecting Health Examination Behavioral Intention


Abstract
:1. Introduction
1.1. Health Belief Model (HBM)
1.2. Health Knowledge
1.3. Social Support
1.4. Behavioral Intention
1.5. Relationships among Self-Efficacy, Perceived Benefits, and Perceived Barriers
1.6. Relationship between Social Support and Perceived Benefits
1.7. Relationships among Health Knowledge, Social Support, and Cues to Action
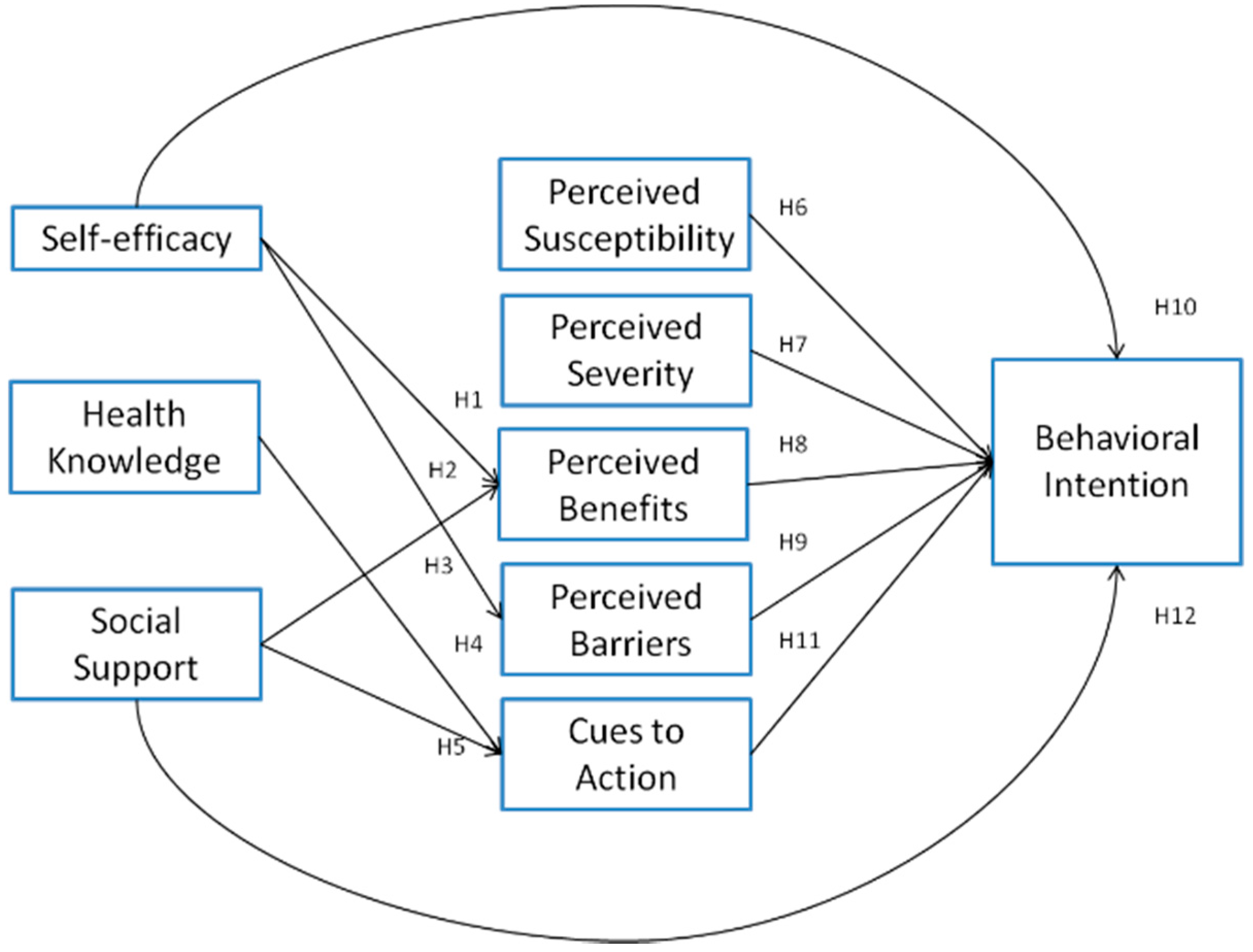
1.8. Relationships among Perceived Severity, Perceived Susceptibility, Perceived Benefits, Perceived Barriers, Self-Efficacy, and Behavioral Intention
1.9. Relationship between Cues to Action and Behavioral Intention
1.10. Relationship between Social Support and Behavioral Intention
2. Method
2.1. Questionnaire Design
2.2. Participants
2.3. Research Instrument
2.4. Internal Consistency, Convergent Validity and Discriminant Validity
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Measurement Model Results
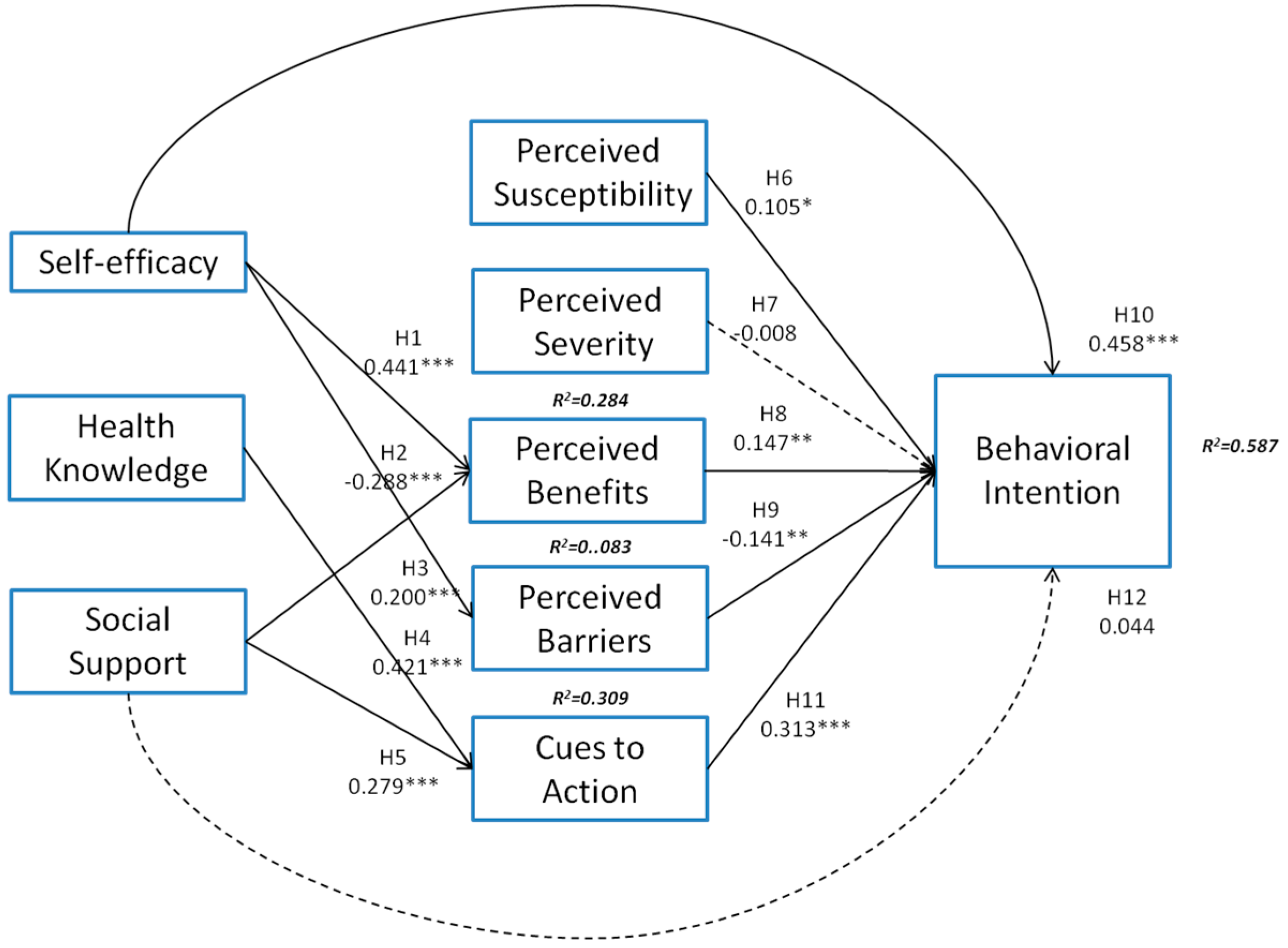
3.3. Structural Model Results
3.4. Hypothesis Testing
4. Discussion
Implications
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix
Self-Efficacy Scale
Health Knowledge
Social Support
Susceptibility
Severity
Benefits
Barriers
Cues to Action
Behavioral Intention
References
- The Top 10 Causes of Death. Available online: http://www.who.int/mediacentre/factsheets/fs310/en/ (accessed on 31 March 2016).
- Ministry of Health and Welfare—Statistics. Available online: http://www.mohw.gov.tw/EN/Ministry/Statistic.aspx?f_list_no=474&fod_list_no=3443 (accessed on 31 July 2014).
- National Health Research Institutes Newsletter. Available online: http://enews.nhri.org.tw/enews_list_new3.php?volume_indx=178&enews_dt=2006-12-01 (accessed on 1 December 2006).
- Becker, M.H.; Maiman, L.A. Sociobehavioral determinants of compliance with health and medical care recommendations. Med. Care 1975, 13, 10–24. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social learning theory and the health belief model. Health Educ. Quart. 1988, 15, 175–183. [Google Scholar] [CrossRef]
- Orji, R.; Vassileva, J.; Mandryk, R. Towards an effective health interventions design: An extension of the health belief model. Online J. Public Health Inform. 2012, 4. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Unger, J.B.; Schuster, D.; Rohrbach, L.A.; Howard-Pitney, B.; Norman, G. Youths’ exposure to environmental tobacco smoke (ets): Associations with health beliefs and social pressure. Addict. Behav. 2003, 28, 39–53. [Google Scholar] [CrossRef]
- Wallace, L.S. Osteoporosis prevention in college women: Application of the expanded health belief model. Am. J. Health Behav. 2002, 26, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Orji, R.; Mandryk, R.L. Developing culturally relevant design guidelines for encouraging healthy eating behavior. Int. J. Hum. Comput. Stud. 2014, 72, 207–223. [Google Scholar] [CrossRef]
- Gillibrand, R.; Stevenson, J. The extended health belief model applied to the experience of diabetes in young people. Br. J. Health Psychol. 2006, 11, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Umeh, K.; Rogan-Gibson, J. Perceptions of threat, benefits, and barriers in breast self-examination amongst young asymptomatic women. Br. J. Health Psychol. 2001, 6, 361–372. [Google Scholar] [CrossRef] [PubMed]
- Radtke, T.; Kaklamanou, D.; Scholz, U.; Hornung, R.; Armitage, C.J. Are diet-specific compensatory health beliefs predictive of dieting intentions and behaviour? Appetite 2014, 76, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Hay, J.L.; Ford, J.S.; Klein, D.; Primavera, L.H.; Buckley, T.R.; Stein, T.R.; Shike, M.; Ostroff, J.S. Adherence to colorectal cancer screening in mammography-adherent older women. J. Behav. Med. 2003, 26, 553–576. [Google Scholar] [CrossRef] [PubMed]
- Anagnostopoulos, F.; Dimitrakaki, C.; Niakas, D.; Tountas, Y. Validity and reliability assessment of health belief scales for mammography screening in greek asymptomatic women. Psychooncology 2013, 22, 1912–1917. [Google Scholar] [CrossRef] [PubMed]
- Gerend, M.A.; Shepherd, J.E. Predicting human papillomavirus vaccine uptake in young adult women: Comparing the health belief model and theory of planned behavior. Ann. Behav. Med. 2012, 44, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.S.; Land, K.C. Testing the health belief model: Lisrel analysis of alternative models of causal relationships between health beliefs and preventive dental behavior. Soc. Psychol. Quart. 1986, 49, 45–60. [Google Scholar] [CrossRef]
- Harrison, J.A.; Mullen, P.D.; Green, L.W. A meta-analysis of studies of the Health Belief Model with adults. Health Educ. Res. 1992, 7, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, C.J. A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Jayanti, R.K.; Burns, A.C. The antecedents of preventive health care behavior: An empirical study. J. Acad. Market. Sci. 1998, 26, 6–15. [Google Scholar] [CrossRef]
- Kenkel, D.S. Health behavior, health knowledge, and schooling. J. Political Econ. 1991, 99, 287–305. [Google Scholar] [CrossRef]
- Haldre, K.; Part, K.; Ketting, E. Youth sexual health improvement in Estonia, 1990–2009: The role of sexuality education and youth-friendly services. Eur. J. Contracept. Reprod. Health Care 2012, 17, 351–362. [Google Scholar] [CrossRef] [PubMed]
- Masuku, S.K.; Lan, S.J. Nutritional knowledge, attitude, and practices among pregnant and lactating women living with hiv in the manzini region of Swaziland. J. Health Popul. Nutr. 2014, 32, 261–269. [Google Scholar] [PubMed]
- Nwokocha, A.R.; Nwakoby, B.A. Knowledge, attitude, and behavior of secondary (high) school students concerning Hiv/Aids in Enugu, Nigeria, in the year 2000. J. Pediatr. Adolesc. Gynecol. 2002, 15, 93–96. [Google Scholar] [CrossRef]
- Zhang, X.; Zhu, M.; Dib, H.H.; Hu, J.; Tang, S.; Zhong, T.; Ming, X. Knowledge, awareness, behavior (KAB) and control of hypertensionamong urban elderly in Western China. Int. J. Cardiol. 2009, 137, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Cobb, S. Social support as a moderator of life stress. Psychosom. Med. 1976, 38, 300–314. [Google Scholar] [CrossRef] [PubMed]
- Kreitner, R.; Kinicki, A. Organizational Behavior, 5th ed.; McGraw-Hill Education: New York, NY, USA, 2001; p. 672. [Google Scholar]
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 1985, 98, 310–357. [Google Scholar] [CrossRef] [PubMed]
- Stanton, S.C.E.; Campbell, L. Perceived social support moderates the link between attachment anxiety and health outcomes. PLoS ONE 2014, 9, e95358. [Google Scholar]
- Fishbein, M.; Ajzen, I. Belief, Attitude, Intention and Behavior: An Introduction to Theory and Research; Addison-Wesley: Reading, MA, USA, 1975; p. 480. [Google Scholar]
- Chen, J.; Liao, Y.; Li, Z.; Tian, Y.; Yang, S.; He, C.; Tu, D.; Sun, X. Determinants of salt-restriction-spoon using behavior in China: Application of the health belief model. PLoS ONE 2013, 8, e83262. [Google Scholar]
- Vander Wal, J.S. The relationship between body mass index and unhealthy weight control behaviors among adolescents: The role of family and peer social support. Econ. Hum. Biol. 2012, 10, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Lajunen, T.; Räsänen, M. Can social psychological models be used to promote bicycle helmet use among teenagers? A comparison of the Health Belief Model, Theory of Planned Behavior and the Locus of Control. J. Safety Res. 2004, 35, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Nieminen, T.; Prattala, R.; Martelin, T.; Harkanen, T.; Hyyppa, M.T.; Alanen, E.; Koskinen, S. Social capital, health behaviours and health: A population-based associational study. BMC Public Health 2013, 13, 613. [Google Scholar] [CrossRef] [PubMed]
- Şimşekoğlu, Ö.; Lajunen, T. Social psychology of seat belt use: A comparison of theory of planned behavior and health belief model. Transp. Res. Pt. F Traffic Psych. Behav. 2008, 11, 181–191. [Google Scholar]
- Sun, X.; Guo, Y.; Wang, S.; Sun, J. Predicting iron-fortified soy sauce consumption Intention: Application of the theory of planned behavior and health belief model. J. Nutr. Educ. Behav. 2006, 38, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Song, F.; Ren, S.; Wang, Y.; Wang, L.; Liu, W.; Wan, Y.; Xu, H.; Zhou, T.; Hu, T.; et al. Predictors of condom use behaviors based on the health belief model (HBM) among female sex workers: A cross-sectional study in Hubei province, China. PLoS ONE 2012, 7, e49542. [Google Scholar] [CrossRef] [PubMed]
- Chow, W.S.; Chan, L.S. Social network, social trust and shared goals in organizational knowledge sharing. Inf. Manag. 2008, 45, 458–465. [Google Scholar] [CrossRef]
- Durrant, R.W.; Brown, Q.L.; Cherrington, A.L.; Andreae, L.J.; Hardy, C.M.; Scarinci, I.C. Social support among African Americans with heart failure: Is there a role for community health advisors? Heart Lung 2013, 42, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Tahmasbipour, N.; Taheri, A. A survey on the relation between social support and mental health in students Shahid Rajaee University. Procedia Soc. Behav. Sci. 2012, 47, 5–9. [Google Scholar] [CrossRef]
- Glozah, F.N.; Pevalin, D.J. Social support, stress, health, and academic success in ghanaian adolescents: A path analysis. J. Adolesc. 2014, 37, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Kruithof, W.J.; van Mierlo, M.L.; Visser-Meily, J.M.; van Heugten, C.M.; Post, M.W. Associations between social support and stroke survivors‘ health-related quality of life—A systematic review. Patient Educ. Couns. 2013, 93, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Marquez, B.; Elder, J.P.; Arredondo, E.M.; Madanat, H.; Ji, M.; Ayala, G.X. Social network characteristics associated with health promoting behaviors among latinos. Health Psychol. 2014, 33, 544–553. [Google Scholar] [CrossRef] [PubMed]
- McKinley, C.J.; Wright, P.J. Informational social support and online health information seeking: Examining the association between factors contributing to healthy eating behavior. Comput. Hum. Behav. 2014, 37, 107–116. [Google Scholar] [CrossRef]
- Griffin, M.J. Health Belief Model, Social Support, and Intent to Screen for Colorectal Cancer in Older African American Men. Ph.D. Thesis, The University of North Carolina, Chapel Hill, NC, USA, 2011. [Google Scholar]
- McClenahan, C.; Shevlin, M.; Adamson, G.; Bennett, C.; O’Neill, B. Testicular self-examination: A test of the health belief model and the theory of planned behaviour. Health Educ. Res. 2007, 22, 272–284. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Multivariate Data Analysis, 5th ed.; Prentice-Hall, Inc.: Upper Saddle River, NJ, USA, 1998; p. 745. [Google Scholar]
- Gaski, J.F.; Nevin, J.R. The differential effects of exercised and unexercised power sources in a marketing channel. J. Mark. Res. 1985, 22, 130–142. [Google Scholar] [CrossRef]
- Bentler, P.M. Handbook of Multivariate Experimental Psychology, 2nd ed.; Plenum: New York, NY, USA, 1988; pp. 317–335. [Google Scholar]
- Anderson, J.C.; Gerbing, D.W. Structural equation modeling in practice: A review and recommended two-step approach. Psychol. Bull. 1988, 103, 411–423. [Google Scholar] [CrossRef]
- Weston, R.; Gore, P.A. A brief guide to structural equation modeling. Counsel. Psychol. 2006, 34, 719–751. [Google Scholar] [CrossRef]
- Ullman, J.B. Structural equation modeling: reviewing the basics and moving forward. J. Pers. Assess. 2006, 87, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Cortina, J.M. What is coefficient alpha? An examination of theory and applications. J. Appl. Psychol. 1993, 78, 98–104. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Item | N | % |
|---|---|---|
| Gender | ||
| Male | 157 | 40.5 |
| Female | 231 | 59.5 |
| Age | ||
| Less than 30 years old | 53 | 13.7 |
| 30–39 years old | 85 | 21.9 |
| 40–49 years old | 108 | 27.8 |
| 49–50 years old | 72 | 18.6 |
| 50–59 years old | 43 | 11.1 |
| over than 60 years old | 27 | 7 |
| Education | ||
| Below junior high school | 46 | 11.9 |
| Senior high school (vocational high school) | 165 | 42.5 |
| College (junior college) | 94 | 24.2 |
| Above Master | 83 | 21.4 |
| Income | ||
| less than NTS 25,000 | 106 | 27.3 |
| between NTS 25,000 and 44,999 | 97 | 25.0 |
| between NTS 45,000 and 64,999 | 80 | 20.6 |
| between NTS 65,000 and 84,999 | 65 | 16.8 |
| more than NTS 85,000 | 50 | 10.3 |
| Marital status | ||
| Married | 282 | 72.7 |
| Not Married | 106 | 27.3 |
| Place of residence | ||
| Taipei | 251 | 64.7 |
| Hualien | 137 | 35.3 |
| Construct | Cronbach’s α | Composite Reliability | Average Variance Extracted |
|---|---|---|---|
| Self-efficacy | 0.87 | 0.87 | 0.71 |
| Health Knowledge | 0.87 | 0.87 | 0.63 |
| Social Support | 0.89 | 0.89 | 0.54 |
| Perceived Susceptibility | 0.76 | 0.77 | 0.53 |
| Perceived Severity | 0.81 | 0.83 | 0.62 |
| Percieved Benefits | 0.89 | 0.89 | 0.68 |
| Perceived Barriers | 0.77 | 0.76 | 0.45 |
| Cues to Action | 0.80 | 0.80 | 0.49 |
| Behavioral Intention | 0.88 | 0.70 | 0.52 |
| Item | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Self-efficacy | 0.84 | ||||||||
| 2. Health Knowledge | 0.39 *** | 0.79 | |||||||
| 3. Social Support | 0.25 *** | 0.20 *** | 0.73 | ||||||
| 4. Perceived Susceptibility | −0.03 | −0.12 * | −0.05 | 0.73 | |||||
| 5. Perceived Severity | 0.11 * | −0.13 ** | 0.24 *** | 0.26 *** | 0.79 | ||||
| 6. Percieved Benefits | 0.42 *** | 0.31 *** | 0.28 *** | 0.00 | 0.29 *** | 0.83 | |||
| 7. Perceived Barriers | −0.22 *** | −0.17 ** | −0.06 | 0.23 *** | 0.09 | −0.10 | 0.67 | ||
| 8. Cues to Action | 0.40 *** | 0.35 *** | 0.28 *** | 0.02 | 0.26 *** | 0.60 *** | −0.07 | 0.70 | |
| 9. Behavioral Intention | 0.58 *** | 0.40 *** | 0.24 *** | 0.06 | 0.17 ** | 0.50 *** | −0.27 *** | 0.53 *** | 0.72 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, H.-T.; Kuo, Y.-M.; Wang, S.-R.; Wang, C.-F.; Tsai, C.-H. Structural Factors Affecting Health Examination Behavioral Intention. Int. J. Environ. Res. Public Health 2016, 13, 395. https://doi.org/10.3390/ijerph13040395
Huang H-T, Kuo Y-M, Wang S-R, Wang C-F, Tsai C-H. Structural Factors Affecting Health Examination Behavioral Intention. International Journal of Environmental Research and Public Health. 2016; 13(4):395. https://doi.org/10.3390/ijerph13040395
Chicago/Turabian StyleHuang, Hui-Ting, Yu-Ming Kuo, Shiang-Ru Wang, Chia-Fen Wang, and Chung-Hung Tsai. 2016. "Structural Factors Affecting Health Examination Behavioral Intention" International Journal of Environmental Research and Public Health 13, no. 4: 395. https://doi.org/10.3390/ijerph13040395
APA StyleHuang, H. -T., Kuo, Y. -M., Wang, S. -R., Wang, C. -F., & Tsai, C. -H. (2016). Structural Factors Affecting Health Examination Behavioral Intention. International Journal of Environmental Research and Public Health, 13(4), 395. https://doi.org/10.3390/ijerph13040395