
Spatial Patterns of Ischemic Heart Disease in Shenzhen, China: A Bayesian Multi-Disease Modelling Approach to Inform Health Planning Policies



Abstract
:1. Introduction
2. Materials
2.1. Study Area
2.2. Data
3. Methods
3.1. Hierarchical Model 1
3.2. Hierarchical Model 2
3.3. Hierarchical Model 3
3.4. Prior Specification and Model Assessment
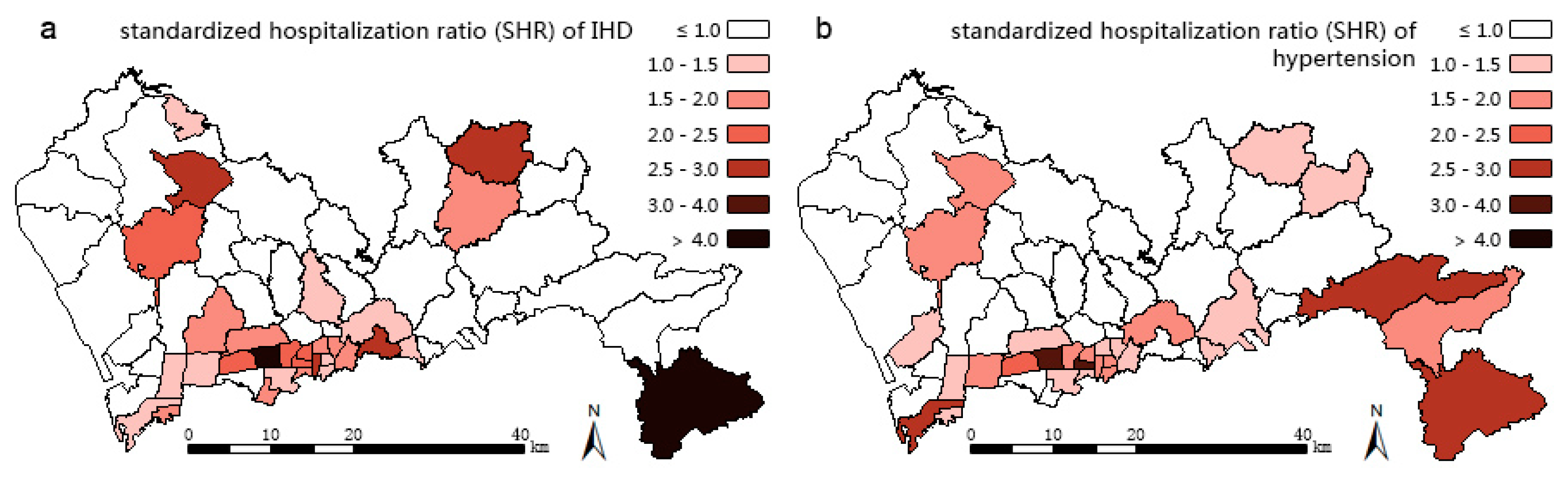
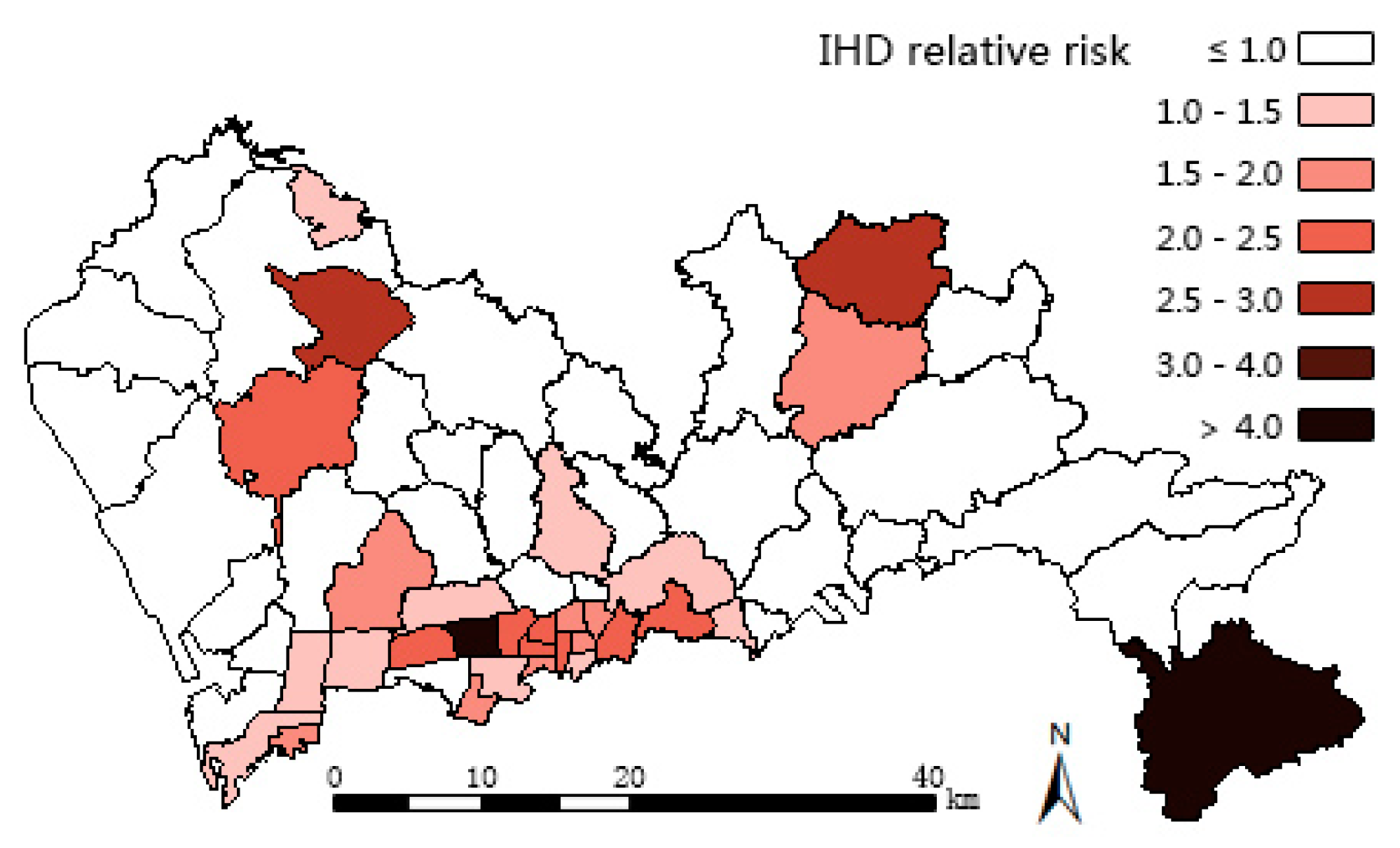
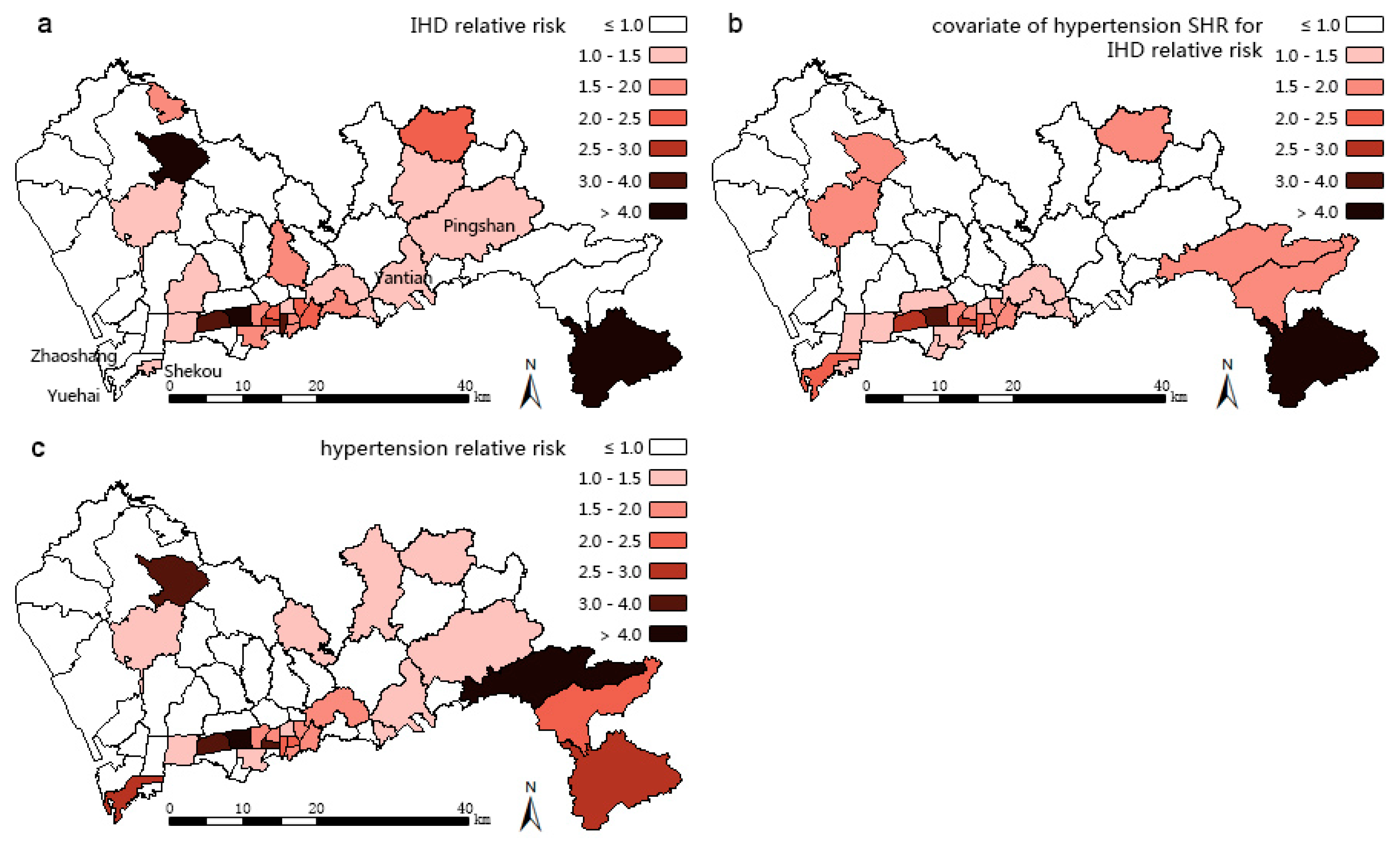
4. Results
5. Discussion
5.1. BMDA to Discover Spatial Patterns of Disease
5.2. BMDA to Discover Spatial Patterns of Unmeasured Risk Factors
5.3. Policy Applications
5.4. Implications for Planning
5.5. Limitations of the Study
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Global Health Estimates 2014 Summary Tables: Deaths by Cause, Age and Sex, 2000–2012; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar]
- World Health Organization. A Global Brief. on Hypertension: Silent Killer, Global Public Health Crisis; World Health Day 2013; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Wang, L. Exploration of strategies for chronic disease prevention and control and relevant system construction in China. Eng. Sci. 2014, 16, 22–30. (In Chinese) [Google Scholar]
- China’s Ministry of Health; China’s Ministry of Education. China National Plan for NCD Prevention and Treatment (2012–2015). Ph.D. Dissertation, Ministry of Health, Beijing, China, 2012. [Google Scholar]
- Ping, L.I. Interventional Effectiveness of Community Behaviors in Patients with Hypertension and Diabetes Mellitus. Med. Soc. 2005, 5, 001. (In Chinese) [Google Scholar]
- Law, J.; Chan, P.W. Bayesian spatial random effect modelling for analysing burglary risks controlling for offender, socioeconomic, and unknown risk factors. Appl. Spat. Anal. Policy 2012, 5, 73–96. [Google Scholar] [CrossRef]
- Law, J.; Quick, M.; Chan, P. Bayesian spatio-temporal modeling for analysing local patterns of crime over time at the small-area level. J. Quant. Criminol. 2014, 30, 57–78. [Google Scholar] [CrossRef]
- Bernadinelli, L.; Pascutto, C.; Best, N.G.; Gilks, W.R. Disease mapping with errors in covariates. Stat. Med. 1997, 16, 741–752. [Google Scholar] [CrossRef]
- Dreassi, E. Polytomous disease mapping to detect uncommon risk factors for related diseases. Biom. J. 2007, 49, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Best, N.; Hansell, A.L. Geographic variations in risk: Adjusting for unmeasured confounders through joint modeling of multiple diseases. Epidemiology (Camb. Mass.) 2009, 20, 400. [Google Scholar] [CrossRef] [PubMed]
- Knorr-Held, L.; Best, N.G. A shared component model for detecting joint and selective clustering of two diseases. J. R. Stat. Soc.: Ser. A (Stat. Soc.) 2001, 164, 73–85. [Google Scholar] [CrossRef] [Green Version]
- Besag, J.; York, J.; Mollié, A. Bayesian image restoration, with two applications in spatial statistics. Ann. Inst. Stat. Math. 1991, 43, 1–20. [Google Scholar] [CrossRef]
- Held, L.; Natário, I.; Fenton, S.E.; Rue, H.; Becker, N. Towards joint disease mapping. Stat. Methods Med. Res. 2005, 14, 61–82. [Google Scholar] [CrossRef] [PubMed]
- Mahaki, B.; Mehrabi, Y.; Kavousi, A.; Akbari, M.E.; Waldhoer, T.; Schmid, V.J.; Yaseri, M. Multivariate disease mapping of seven prevalent cancers in Iran using a shared component model. Asian Pac. J. Cancer Prev. 2011, 12, 2353–2358. [Google Scholar] [PubMed]
- Chamanpara, P.; Moghimbeigi, A.; Faradmal, J.; Poorolajal, J. Joint disease mapping of two digestive cancers in Golestan province, Iran using a shared component model. Osong. Public Health Res. Perspect. 2015, 6, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Lawson, A.B. Bayesian Disease Mapping: Hierarchical Modeling in Spatial Epidemiology; CRC Press: Boca Raton, FL, USA, 2013. [Google Scholar]
- Liu, L. 2010 Chinese Guidelines for the Management of Hypertension. Chin. J. Hypertens. 2011, 19, 701–743. [Google Scholar]
- Yang, J.; Yin, Z. Risk factors of cardiovascular diseases and classification of prevention of coronary heart disease. Shanghai J. Prev. Med. 2005, 17, 10–13. (In Chinese) [Google Scholar]
- Zamorano, J.; Erdine, S.; Pavia, A.; Kim, J.H.; Al-Khadra, A.; Westergaard, M.; Sutradhar, S.; Yunis, C. CRUCIAL Investigators. Proactive multiple cardiovascular risk factor management compared with usual care in patients with hypertension and additional risk factors: The CRUCIAL trial. Curr. Med. Res. Opin. 2011, 27, 821–833. [Google Scholar] [PubMed]
- Shenzhen Statistics and Information Bureau. Shenzhen Statistical Yearbook, Beijing, China, 2013. Available online: http://www.sztj.gov.cn/nj2013/indexce.htm (accessed on 9 December 2015).
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems. World Health Organization, 2004; Volume 1. [Google Scholar]
- Lawson, A.B.; Biggeri, A.B.; Boehning, D.; Lesaffre, E.; Viel, J.F.; Clark, A.; Divino, F. Disease mapping models: An empirical evaluation. Disease Mapping Collaborative Group. Stat. Med. 2000, 19, 2217–2241. [Google Scholar]
- Lunn, D.J.; Thomas, A.; Best, N.; Spiegelhalter, D. WinBUGS-a Bayesian modelling framework: Concepts, structure, and extensibility. Stat. Comput. 2000, 10, 325–337. [Google Scholar] [CrossRef]
- Spiegelhalter, D.J.; Best, N.G.; Carlin, B.P.; Van Der Linde, A. Bayesian measures of model complexity and fit. J. R. Stat. Soc.: Ser. B (Stat. Methodol.) 2002, 64, 583–639. [Google Scholar] [CrossRef]
- Soni, J.; Ansari, U.; Sharma, D.; Soni, S. Predictive data mining for medical diagnosis: An overview of heart disease prediction. Int. J. Comput. Appl. 2011, 17, 43–48. [Google Scholar] [CrossRef]
- Khan, A.; Uddin, S.; Srinivasan, U. Adapting graph theory and social network measures on healthcare data: A new framework to understand chronic disease progression. In Proceedings of the Australasian Computer Science Week Multiconference, Canberra, Australia, 2–5 February 2016; ACM: New York, NY, USA, 2016; p. 66. [Google Scholar]
- Carretero, O.A.; Oparil, S. Essential hypertension part I: Definition and etiology. Circulation 2000, 101, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Sheiham, A.; Watt, R.G. The common risk factor approach: A rational basis for promoting oral health. Community Dent. Oral Epidemiol. 2000, 28, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Law, J.; Chan, P.W. Monitoring residual spatial patterns using Bayesian hierarchical spatial modelling for exploring unknown risk factors. Trans. GIS 2011, 15, 521–540. [Google Scholar] [CrossRef]
- Chinese Society of Cardiology of Chinese Medical Association, and Editorial Board of Chinese Journal of Cardiology. Prevention guidelines for cardiovascular disease in China. Chin. J. Cardiol. 2011, 39, 3–22. (In Chinese) [Google Scholar]
- Liang, X.; Shi, X. Report on Ability of Chronic Diseases Control and Prevention of China; People’s Health Press: Beijing, China, 2013. (In Chinese) [Google Scholar]
- Cheng, Z. Application of Kish selecting method in Chinese social research. Stat. Res. 2009, 26, 103–104. (In Chinese) [Google Scholar]
- Lyu, S.; Su, J.; Xiang, Q.; Wu, M. Suggestion on improvement of surveillance technique for chronic diseases and related risk factors in China. Dis. Surveill. 2014, 29, 247–249. (In Chinese) [Google Scholar]
- Chen, Y.; Li, H.; Wang, L. The development of Chinese chronic diseases and risk factors surveillance and its challenges. Chin. J. Prev. Med. 2012, 46, 389–391. (In Chinese) [Google Scholar]
- Wang, Y.; Du, Q.; Ren, F.; Liang, S.; Lin, D.N.; Tian, Q.; Chen, Y.; Li, J.-J. Spatio-temporal variation and prediction of ischemic heart disease hospitalizations in Shenzhen, China. Int. J. Environ. Res. Public Health 2014, 11, 4799–4824. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Du, Q.; Liang, S.; Nie, K.; Lin, D.N.; Chen, Y.; Li, J.J. Analysis of the spatial variation of hospitalization admissions for hypertension disease in Shenzhen, China. Int. J. Environ. Res. Public Health 2014, 11, 713–733. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Nie, L.; Long, M.; Liu, J.; Zhang, X.; Wang, W. Effect analysis of health education and dietary intervention on integrated hypertension management. Community Med. J. 2010, 8, 20–21. (In Chinese) [Google Scholar]
- Wang, X.; Su, A.; Chen, Y.; Wu, Y.; Yang, W.; Cheng, X. Implementation Effects and Evaluation of Suitable Health Management Technology among the Aged in Guangming New District of Shenzhen. Chin. Primary Health Care 2011, 25, 17–19. (In Chinese) [Google Scholar]
- Hu, F.B.; Liu, Y.; Willett, W.C. Preventing chronic diseases by promoting healthy diet and lifestyle: Public policy implications for China. Obes. Rev. 2011, 12, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Lam, K.K.; Johnston, J.M. Health insurance and healthcare utilisation for Shenzhen residents: A tale of registrants and migrants? BMC Public Health 2012, 12, 868. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Yang, J. A study of knowledge, attitude and behaviour in community-based integral prevention of chronic diseases. Health Econ. Res. 2011, 289, 29–31. (In Chinese) [Google Scholar]
- Jiang, Y.; Zhang, M.; Li, Y.; Li, X.; Wang, L.; Zhao, W. Investigation on self-measurement and awareness of body weight among Chinese adults in 2010. Chin. J. Health Educ. 2013, 29, 485–488. (In Chinese) [Google Scholar]
- Wang, W.; Li, X.; Du, J.; Zhao, M. Investigating the substance use problem in the community of Sichuan province with ASSIST. Chin. J. Drug Depend. 2015, 24, 49–53. (In Chinese) [Google Scholar]
- Sun, H.; Zeng, Q.; Du, J.; Chen, H.; Fan, C.; Jiang, H.; Zhao, M. Reliability and validity of the Chinese version of Alcohol, Smoking, and Substance Use Involvement Screening Test. Chin. Ment. Health J. 2010, 24, 351–355. (In Chinese) [Google Scholar]
- Ge, K.; Yang, X.; Cheng, Y. Dietary guidelines for Chinese residents (2007). Acta Nutr. Sin. 2008, 20, 14–15. (In Chinese) [Google Scholar]
- Hao, W.; Cao, D.; Yu, X. Drinking and drinking-related problems in China. Chin. J. Drug Depend. 2007, 16, 193–197. (In Chinese) [Google Scholar]
- Health and Family Planning Commission of Shenzhen Municipality. Notice on the Issuing Shenzhen Regional Health Service Planning (2015–2020). Available online: http://www.szhpfpc.gov.cn/wsj/main?fid=open&fun=show_news1&from=view&nid=25876 (accessed on 9 December 2015). (In Chinese)
- The General Office of the State Council. Notice of the General Office of the State Council on the issuing the outline of the national health service system planning (2015–2020). Gaz. State Council People’s Repub. China 2015, 10, 25–39. (In Chinese) [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | Disease | Parameter/Component | Median CI (5%, 95%) of Variances | Median CI (5%, 95%) of Component Ratio | DIC |
|---|---|---|---|---|---|
| 1 | IHD | 0.789 (0.517, 1.046) | - | 530.2 | |
| 0.708 (−6.318, 4.480) | 85.5% (75.0%, 85.6%) | ||||
| 2 | IHD | 1.494 (0.790, 2.502) | - | 488.6 | |
| 0.014 (−0.130, 0.132) | 72.5% (41.6%, 80.2%) | ||||
| 3 | IHD | 1.145 (0.873, 1.494) | - | 520.8 | |
| −0.023 (−0.120, 0.121) | 69.6% (44.3%, 78.4%) | ||||
| hypertension | 0.873 (0.669, 1.145) | - | 489.1 | ||
| −0.017 (−0.091, 0.092) | 80.2% (49.2%, 90.6%) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, Q.; Zhang, M.; Li, Y.; Luan, H.; Liang, S.; Ren, F. Spatial Patterns of Ischemic Heart Disease in Shenzhen, China: A Bayesian Multi-Disease Modelling Approach to Inform Health Planning Policies. Int. J. Environ. Res. Public Health 2016, 13, 436. https://doi.org/10.3390/ijerph13040436
Du Q, Zhang M, Li Y, Luan H, Liang S, Ren F. Spatial Patterns of Ischemic Heart Disease in Shenzhen, China: A Bayesian Multi-Disease Modelling Approach to Inform Health Planning Policies. International Journal of Environmental Research and Public Health. 2016; 13(4):436. https://doi.org/10.3390/ijerph13040436
Chicago/Turabian StyleDu, Qingyun, Mingxiao Zhang, Yayan Li, Hui Luan, Shi Liang, and Fu Ren. 2016. "Spatial Patterns of Ischemic Heart Disease in Shenzhen, China: A Bayesian Multi-Disease Modelling Approach to Inform Health Planning Policies" International Journal of Environmental Research and Public Health 13, no. 4: 436. https://doi.org/10.3390/ijerph13040436
APA StyleDu, Q., Zhang, M., Li, Y., Luan, H., Liang, S., & Ren, F. (2016). Spatial Patterns of Ischemic Heart Disease in Shenzhen, China: A Bayesian Multi-Disease Modelling Approach to Inform Health Planning Policies. International Journal of Environmental Research and Public Health, 13(4), 436. https://doi.org/10.3390/ijerph13040436