
Antifungal Effect of Henna against Candida albicans Adhered to Acrylic Resin as a Possible Method for Prevention of Denture Stomatitis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size and Specimen Preparation
2.2. Exposing Acrylic Specimens to Candida albicans
2.3. Evaluation
- 1-
- Slide count: 2.5 µL of Trypan Blue 0.4% solution in Phosphate (MP-Biomedicals, Santa Ana, CA, USA) was added to 7.5 µL of each sample to be placed on a slide count (Nebauer Slide Counter “Chambers-Marienfeld”, Marienfeld, Lauda-Königshofen, Germany) for microscopic evaluation. With Trypan Blue stain, dead Candida albicans would appear blue in color while live Candida would appear transparent with a blue border line. Trypan Blue stain should allow for counting the number of Candida under light microscope at low power magnifications (10×). Slide count usually contains 4 main squares, and each is divided into 16 squares. Candida was counted in 2 main squares and multiplied by 2 to get the total number of Candida in the slide.
- 2-
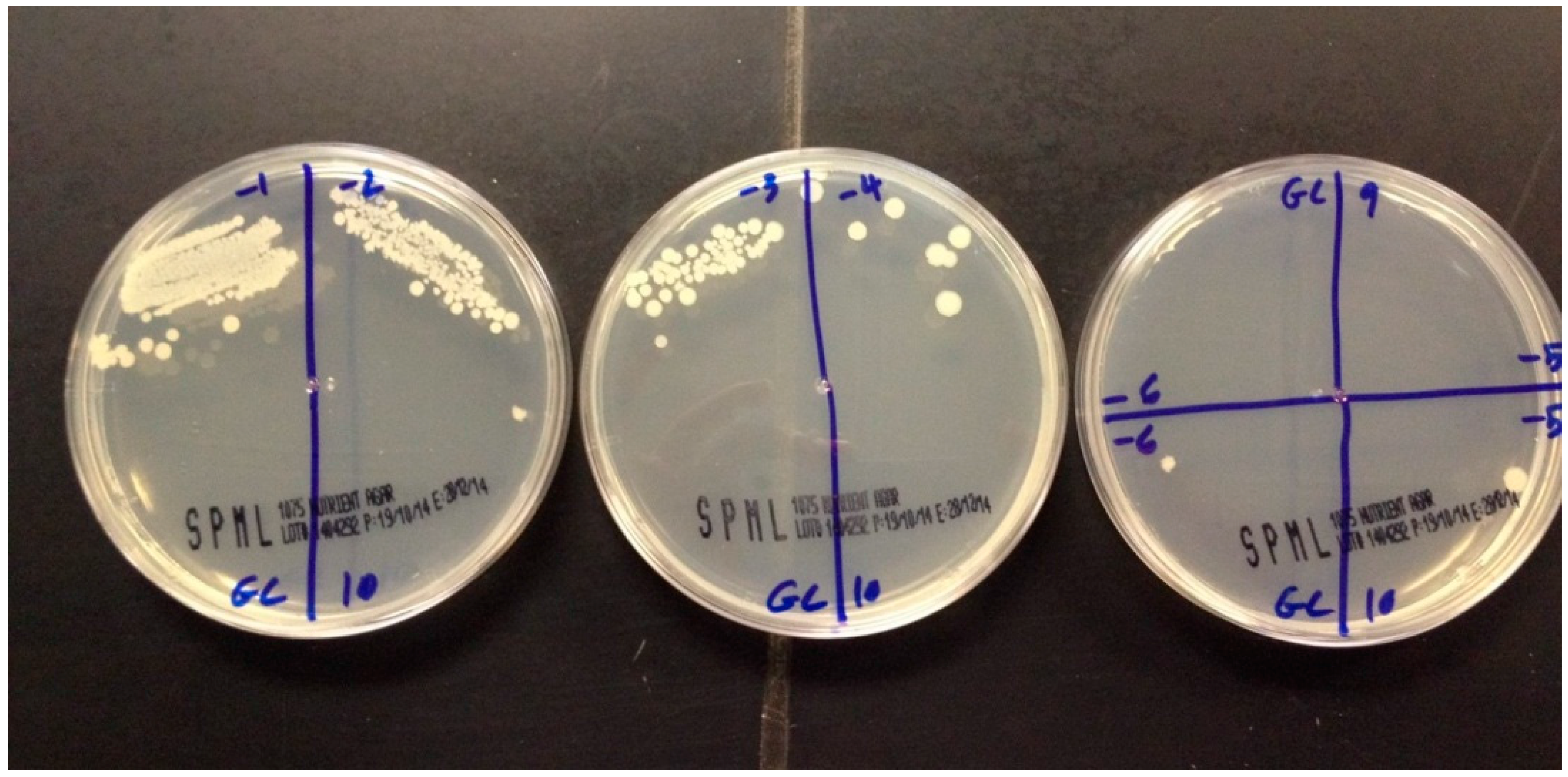
- Miles and Misra assay: This is the standard, accurate culture-based test to quantify live organisms. Briefly, 10 µL of each sample was taken, serially diluted and spread on a quadrant of a Petri dish and then it was incubated at 37 °C for 48 h. Colonies of Candida albicans were counted, using a marker pen counter (colony counter “Scienceware-bel-art products”, Wayne, NJ, USA), in the quadrant where acceptable growth is noted and corrected for the dilution factor. If the number of colonies that cover the whole surface of the Petri dish was more than 500, it was considered as overgrowth.
- 3-
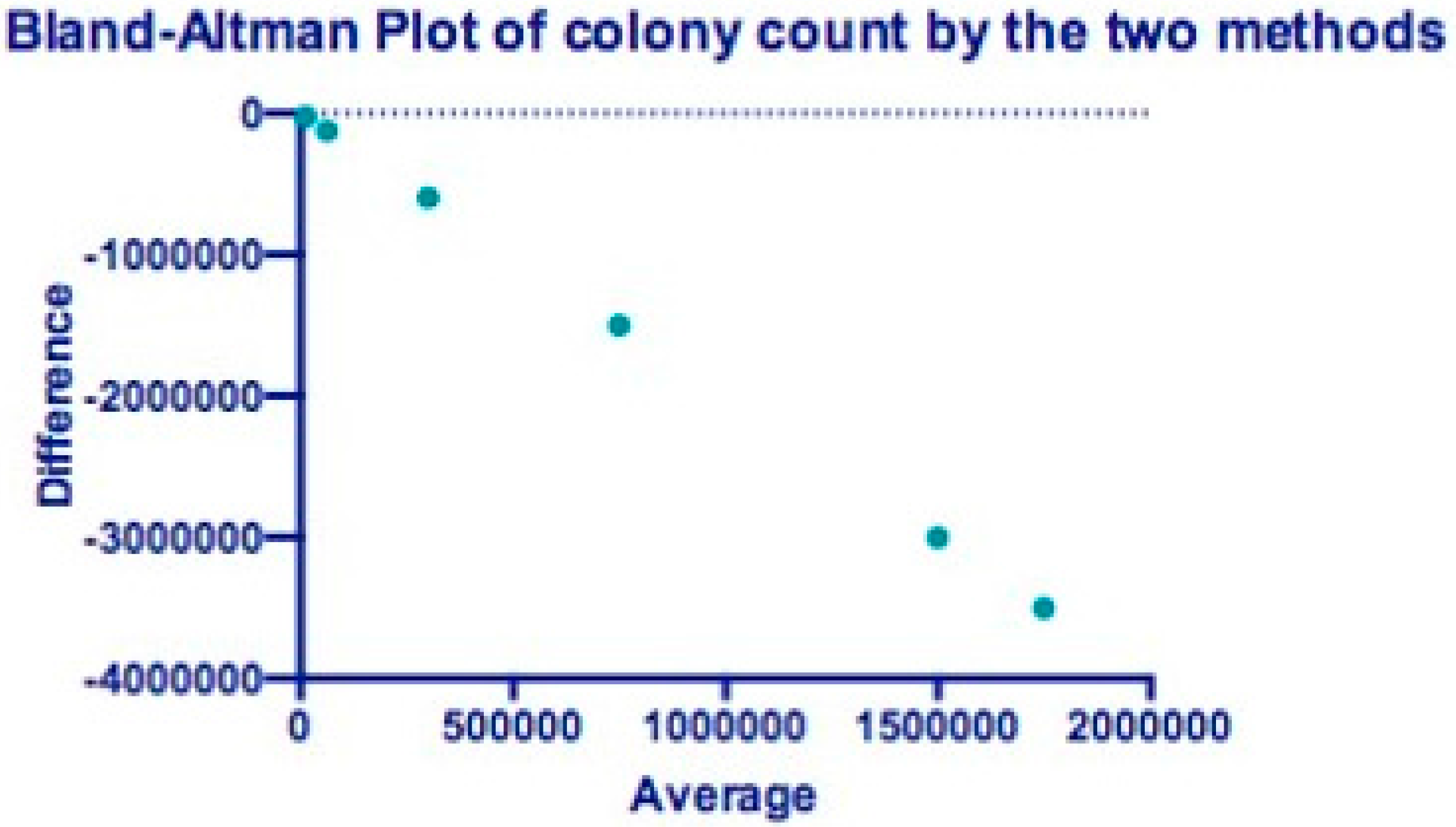
- Statistics: Because the discrete colony count values varied a lot, the mode method was used to represent the results. Log reduction of each concentration by both methods was reported with p-value calculated by the paired t-test to check for robustness. To compare the performance of the two assays, the Bland–Altman plot was performed [33] using Graph Pad 6.0 for Windows (GraphPad Software, La Jolla, CA, USA) to illustrate method agreement. It plotted the difference in average counts between the two methods. All results for all concentration and growth control were included in the analysis. The software calculated the bias that represents the average discrepancy between the methods, and the upper and lower levels of agreement (LOA) calculated as bias ±1.96 X standard deviation of the bias. The closer the bias is to zero and the narrower the limits of agreement, the more agreed the methods are.
3. Results
3.1. Slide Count
3.2. Direct Culture Method
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Pattanaik, S. Denture Stomatitis: A Literature Review. J. Indian Acad. Oral Med. Radiol. 2010, 22, 136. [Google Scholar] [CrossRef]
- Figueiral, M.H.; Azul, A.; Pinto, E.; Fonseca, P.A.; Branco, F.M.; Scully, C. Denture-related stomatitis: Identification of aetiological and predisposing factors—A large cohort. J. Oral Rehabil. 2007, 34, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Zomorodian, K.; Haghighi, N.N.; Rajaee, N.; Pakshir, K.; Tarazooie, B.; Vojdani, M.; Sedaghat, F.; Vosoghi, M. Assessment of Candida species colonization and denture-related stomatitis in complete denture wearers. Med. Mycol. 2011, 49, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Pires, F.R.; Santos, E.B.D.; Bonan, P.R.F.; De Almeida, O.P.; Lopes, M.A. Denture stomatitis and salivary Candida in Brazilian edentulous patients. J. Oral Rehabil. 2002, 29, 1115–1119. [Google Scholar] [CrossRef] [PubMed]
- Ramage, G.; Tomsett, K.; Wickes, B.L.; López-Ribot, J.L.; Redding, S.W. Denture stomatitis: A role for Candida biofilms. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004, 98, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Kossioni, A.E. The prevalence of denture stomatitis and its predisposing conditions in an older Greek population. Gerodontology 2011, 28, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Arendorf, T.M. Denture stomatitis: A review. J. Oral Rehabil. 1987, 14, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Jain, D.; Shakya, P. An in vitro study on effect of Delmopinol application on Candida albicans adherence on heat cured denture base acrylic resin: A thorough study. Indian J. Dent. Res. 2013, 24, 645. [Google Scholar] [CrossRef] [PubMed]
- Castro, D.T.D.; Holtz, R.D.; Alves, O.L.; Watanabe, E.; Valente, M.L.D.C.; Silva, C.H.L.D. Development of a novel resin with antimicrobial properties for dental application. J. Appl. Oral Sci. 2014, 22, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Pereira-Cenci, T.; Del Bel Cury, A.A.; Crielaard, W.; Ten Cate, J.M. Development of Candida-associated denture stomatitis: New insights. J. Appl. Oral Sci. 2008, 16, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Douglas, W.; Walker, D. Nystatin in denture liners—An alternative treatment of denture stomatitis. Br. Dent. J. 1973, 135, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.; Nutt, G. The in vitro fungicidal properties of Visco-gel, alone and combined with nystatin and amphotericin B. J. Oral Rehabil. 1978, 5, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, D.; George, T.; Chandra, J.; Mukherjee, P.; Ghannoum, M. Antifungal susceptibility of Candida biofilms: Unique efficacy of amphotericin B lipid formulations and echinocandins. Antimicrob. Agents Chemother. 2002, 46, 1773–1780. [Google Scholar] [CrossRef] [PubMed]
- Coogan, M.M. (B1) Candida and mycotic infections. Adv. Dent. Res. 2006, 19, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.A.; Alharbi, F.A.; Suresh, C.S. Effectiveness of coating acrylic resin dentures on the Candida adhesion. J. Prosthodont. 2013, 22, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Yodmongkol, S.; Chantarachindawong, R.; Thaweboon, S.; Thaweboon, B.; Amornsakchai, T.; Srikhirin, T. The effects of silane-SiO2 nanocomposite films on Candida albicans adhesion and the surface and physical properties of acrylic resin denture base material. J. Prosthet. Dent. 2014, 112, 1530–1538. [Google Scholar] [CrossRef] [PubMed]
- Izumida, F.E.; Moffa, E.B.; Vergani, C.E.; Machado, A.L.; Jorge, J.H.; Giampaolo, E.T. In vitro evaluation of adherence of Candida albicans, Candida glabrata, and Streptococcus mutans to an acrylic resin modified by experimental coatings. Biofouling 2014, 30, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, M.; Ahmad, A.; Shahid, M.; Khan, M.I.; Khan, S.A.; Manzoor, N.; Mohammad, F. Assessment of colorimetric, antibacterial and antifungal properties of woollen yarn dyed with the extract of the leaves of henna (Lawsonia inermis). J. Clean. Prod. 2012, 27, 42–50. [Google Scholar] [CrossRef]
- Ramírez-Andreo, A.; Hernández-Gil, A.; Brufau, C.; Marín, N.; Jiménez, N.; Hernández-Gil, J.; Tercedor, J.; Soria, C. Allergic contact dermatitis to temporary Henna tattoos. Actas Dermo-Sifiliogr. (Engl. Ed.) 2007, 98, 91–95. [Google Scholar] [CrossRef]
- Bele, A.A.; Jandhav, V.M.; Kadam, V.J. Potential of Tannnins: A review. Asian J. Plant Sci. 2010, 9, 209–214. [Google Scholar]
- Kirkland, D.; Marzin, D. An assessment of the genotoxicity of 2-hydroxy-1, 4-naphthoquinone, the natural dye ingredient of Henna. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2003, 537, 183–199. [Google Scholar] [CrossRef]
- Marzin, D.; Kirkland, D. 2-Hydroxy-1, 4-naphthoquinone, the natural dye of Henna, is non-genotoxic in the mouse bone marrow micronucleus test and does not produce oxidative DNA damage in Chinese hamster ovary cells. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2004, 560, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, G.; Goyal, S.; Poonia, P. Lawsonia inermis Linnaeus: A Phytopharmacological Review. Int. J. Pharm. Sci. Drug Res. 2010, 2, 91–98. [Google Scholar]
- Jha, R.K.; Jha, P.K.; Rana, S.V.; Guha, S.K. Spermicidal action of styrene maleic anhydride polyelectrolyte in combination with magnetic and electrically conductive particles. Int. J. Pharmacol. 2009, 5, 1–12. [Google Scholar] [CrossRef]
- Bairagi, G.; Kabra, A.; Mandade, R. Anthelmintic activity of Lawsonia inermis L. leaves in Indian adult earthworm. Int. J. Res. Pharm. Biomed. Sci. 2011, 2, 237–240. [Google Scholar]
- Mikhaeil, B.R.; Badria, F.A.; Maatooq, G.T.; Amer, M. Antioxidant and immunomodulatory constituents of henna leaves. Z. Naturforschung C 2004, 59, 468–476. [Google Scholar] [CrossRef]
- Muhammad, H.; Muhammad, S. The use of Lawsonia inermis Linn. (Henna) in the management of burn wound infections. Afr. J. Biotechnol. 2005, 4, 934–937. [Google Scholar]
- Dweck, A.C. Natural ingredients for colouring and styling. Int. J. Cosmet. Sci. 2002, 24, 287–302. [Google Scholar] [CrossRef] [PubMed]
- Saadabi, M.A.A. Evaluation of Lawsonia inermis Linn. (Sudanese Henna) leaf extracts as an antimicrobial agent. Res. J. Biol. Sci. 2007, 2, 419–423. [Google Scholar]
- Abulyazid, I.; Mahdy, E.M.E.; Ahmed, R.M. Biochemical study for the effect of henna (Lawsonia inermis) on Escherichia coli. Arabian J. Chem. 2013, 6, 265–273. [Google Scholar] [CrossRef]
- Sritrairat, N.; Nukul, N.; Inthasame, P.; Sansuk, A.; Prasirt, J.; Leewatthanakorn, T.; Piamsawad, U.; Dejrudee, A.; Panichayupakaranant, P.; Pangsomboon, K.; et al. Antifungal activity of lawsone methyl ether in comparison with chlorhexidine. J. Oral Pathol. Med. 2011, 40, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Ponnusamy, K.; Petchiammal, C.; Mohankumar, R.; Hopper, W. In vitro antifungal activity of indirubin isolated from a South Indian ethnomedicinal plant Wrightia tinctoria R. Br. J. Ethnopharmacol. 2010, 132, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Dewitte, K.; Fierens, C.; Stöckl, D.; Thienpont, L.M. Application of the Bland-Altman plot for interpretation of method-comparison studies: A critical investigation of its practice. Clin. Chem. 2002, 48, 799–801, author reply 801–802. [Google Scholar] [PubMed]
- Singla, S.; Gupta, R.; Puri, A.; Singh, V.; Roy, S. Comparison of antiCandidal activity of Punica granatum (Pomegranate) and Lawsonia inermis (Henna leaves): An in vitro study. Int. J. Dent. Res. 2013, 1, 8–13. [Google Scholar] [CrossRef]
- Gendreau, L.; Loewy, Z.G. Epidemiology and etiology of denture stomatitis. J. Prosthodont. 2011, 20, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Yoshijima, Y.; Murakami, K.; Kayama, S.; Liu, D.; Hirota, K.; Ichikawa, T.; Miyake, Y. Effect of substrate surface hydrophobicity on the adherence of yeast and hyphal Candida. Mycoses 2009, 53, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Sivakumar, I.; Arunachalam, K.S.; Sajjan, S.; Ramaraju, A.V.; Rao, B.; Kamaraj, B. Incorporation of antimicrobial macromolecules in acrylic denture base resins: A research composition and update. J. Prosthodont. 2014, 23, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Raj, P.A.; Dentino, A.R. Denture polymers with antimicrobial properties: A review of the development and current status of anionic poly (methyl methacrylate) polymers. Future Med. Chem. 2013, 5, 1635–1645. [Google Scholar] [CrossRef] [PubMed]
- Chandra, J.; Mukherjeel, P.K.; Leidichl, S.D.; Faddoul, F.F.; Hoyer, L.L.; Douglas, L.J.; Ghannouml, M.A. Antifungal resistance of Candidal biofilms formed on denture acrylic in vitro. J. Dent. Res. 2001, 80, 903–908. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group | Agar Dilution Mode | Log Reduction in Candida | p-Value | Counting Chamber Mode | Log Reduction in Candida | p-Value |
|---|---|---|---|---|---|---|
| A | 5 × 106 | - | - | 2 × 106 | - | - |
| B 1% | 2 × 106 | 6.5 | 0.0001 * | 1 × 106 | 6 | 0.001 * |
| C 2.5% | 5 × 105 | 6.7 | 0.2 | 7 × 105 | 6.1 | 0.1 |
| D 5% | 4 × 106 | 6 | 0.6667 | 2 × 106 | NA | NA |
| E 7.5% | 1 × 105 | 6.7 | 0.0001 * | 1.5 × 105 | 6.3 | 0.1 |
| F 10% | 1 × 104 | 6.7 | 0.001 * | 4 × 104 | 6.3 | 0.01 * |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nawasrah, A.; AlNimr, A.; Ali, A.A. Antifungal Effect of Henna against Candida albicans Adhered to Acrylic Resin as a Possible Method for Prevention of Denture Stomatitis. Int. J. Environ. Res. Public Health 2016, 13, 520. https://doi.org/10.3390/ijerph13050520
Nawasrah A, AlNimr A, Ali AA. Antifungal Effect of Henna against Candida albicans Adhered to Acrylic Resin as a Possible Method for Prevention of Denture Stomatitis. International Journal of Environmental Research and Public Health. 2016; 13(5):520. https://doi.org/10.3390/ijerph13050520
Chicago/Turabian StyleNawasrah, Amal, Amani AlNimr, and Aiman A. Ali. 2016. "Antifungal Effect of Henna against Candida albicans Adhered to Acrylic Resin as a Possible Method for Prevention of Denture Stomatitis" International Journal of Environmental Research and Public Health 13, no. 5: 520. https://doi.org/10.3390/ijerph13050520
APA StyleNawasrah, A., AlNimr, A., & Ali, A. A. (2016). Antifungal Effect of Henna against Candida albicans Adhered to Acrylic Resin as a Possible Method for Prevention of Denture Stomatitis. International Journal of Environmental Research and Public Health, 13(5), 520. https://doi.org/10.3390/ijerph13050520