
A Case of Acute Osteomyelitis: An Update on Diagnosis and Treatment

Abstract
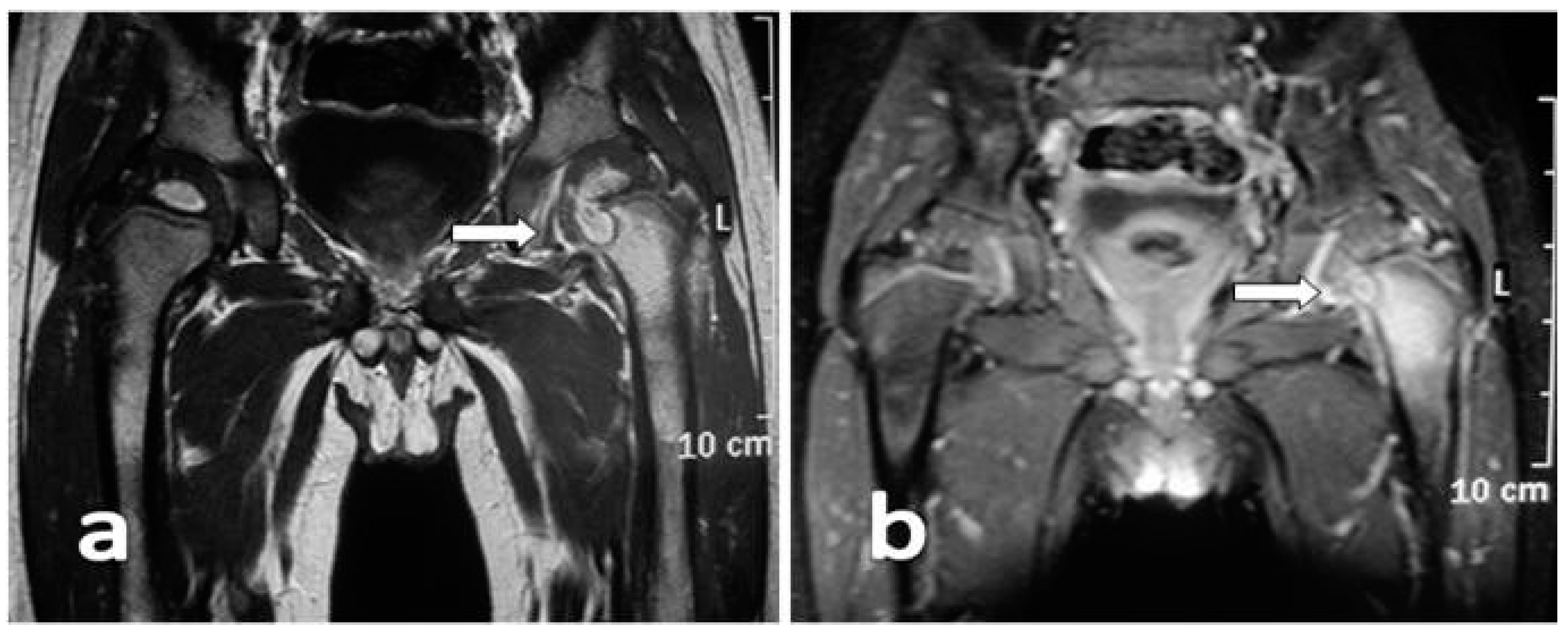
:1. Case Presentation
2. Introduction
3. Diagnosis
4. Update on Therapeutic Management
5. Conclusions
Authors Contribution
Conflicts of Interest
Abbreviations
| WBC | White Blood Cell |
| CRP | C-reactive protein |
| ESR | Erythrocyte Sedimentation Rate |
| MRI | Magnetic Resonance Imaging |
| MSSA | Methicillin-sensitive Staphylococcus aureus |
| MRSA | Methicillin-resistant Staphylococcus aureus |
| PCT | Procalcitonin |
| pGALS | pediatric Gait, Arms, Legs, Spine |
| TMP/SMX | trimethoprim/sulfamethoxazole |
References
- Howard-Jones, A.R.; Isaacs, D. Systematic review of duration and choice of systemic antibiotics therapy for acute haematogenous bacterial osteomyelitis in children. J. Paediatr. Child Health 2013, 49, 760–768. [Google Scholar] [CrossRef] [PubMed]
- The Pediatric Orthopedic Society of North America (POSNA). Acute Osteomyelitis. 2013. Available online: www.posna.org/education/StudyGuide/acuteOsteomyelitis.asp (accessed on 25 May 2016).
- Yeo, A.; Ramachandran, M. Acute haematogenous osteomyelitis in children. BMJ 2014, 348, 66. [Google Scholar] [CrossRef] [PubMed]
- Gafur, O.A.; Copley, L.A.B.; Hollmig, S.T.; Browne, R.H.; Thornton, L.A.; Crawford, S.E. The impact of the current epidemiology of pediatric musculoskeletal infection on evaluation and treatment guidelines. J. Pediatr. Orthop. 2008, 28, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Morrissy, R.T.; Haynes, D.W. Acute hematogenous osteomyelitis: A model with trauma as an etiology. J. Pediatr. Orthop. 1989, 9, 447. [Google Scholar] [CrossRef] [PubMed]
- Whalen, J.L.; Fitzgerald, R.H.; Morrissy, R.T. A histological study of acute haematogenous osteomyelitis following physeal injuries in rabbits. J. Bone Joint Surg. Am. 1988, 70, 1383. [Google Scholar] [PubMed]
- Trueta, J. The 3 types of acute hematogenous osteomyelitis. Schweiz. Med. Wochenschr. 1963, 93, 306. [Google Scholar] [PubMed]
- Kahn, D.S.; Pritzker, K.P. The pathophysiology of bone infection. Clin. Orthop. Relat. Res. 1973, 96, 12. [Google Scholar] [PubMed]
- Dartnell, J.; Ramachandran, M.; Katchburian, M. Haematogenous acute and subacute paediatric osteomyelitis: A systematic review of the literature. J. Bone Joint Surg. Br. 2012, 94, 584–595. [Google Scholar] [CrossRef] [PubMed]
- Pääkkönen, M.; Kallio, M.J.T.; Kallio, P.E.; Peltola, H. Sensitivity of erythrocyte sedimentation rate and C-reactive protein in childhood bone and joint infections. Clin. Orthop. Relat. Res. 2010, 468, 861–866. [Google Scholar] [CrossRef] [PubMed]
- Butbul-Aviel, Y.; Koren, A.; Halevy, R.; Sakran, W. Procalcitonin as a diagnostic aid in osteomyelitis and septic arthritis. Pediatr. Emerg. Care 2005, 21, 828–832. [Google Scholar] [CrossRef] [PubMed]
- Jereb, M.; Kotar, T.; Jurca, T.; Lejko Zupanc, T. Usefulness of procalcitonin for diagnosis of infective endocarditis. Intern. Emerg. Med. 2009, 4, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.C.; Caesar, D.H.; Davison, C.; Phibbs, R.; Than, M.P. Review article: How useful are laboratory investigations in the emergency department evaluation of possible osteomyelitis? Emerg. Med. Australas. 2011, 23, 317–330. [Google Scholar] [CrossRef] [PubMed]
- Maharajan, K.; Patro, D.K.; Menon, J.; Hariharan, A.P.; Parija, S.C.; Poduval, M.; Thimmaiah, S. Serum Procalcitonin is a sensitive and specific marker in the diagnosis of septic arthritis and acute osteomyelitis. J. Orthop. Surg. Res. 2013, 8, 19. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.J.; Wu, M.S.; Lin, K.H.; Lin, W.L.; Chen, H.C.; Wu, J.Y.; Lee, M.C.; Lee, C.C. The use of procalcitonin in the diagnosis of bone and joint infection: A systemic review and meta-analysis. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.D.; Ramaesh, R.; Kalima, P.; Murray, A.; Gaston, M.S. Microbiological characteristics of acute osteoarticular infections in children. J. Med. Microbiol. 2015, 64, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Foster, H.E.; Kay, L.J.; Friswell, M.; Coady, D.; Myers, A. Musculoskeletal screening examination (pGALS) for schoo-aged children based on the adult GALS screen. Arthritis Rheumatol. 2006, 55, 709–716. [Google Scholar] [CrossRef] [PubMed]
- Brix, N.; Rosthøj, S.; Herlin, T.; Hasle, H. Arthritis as presenting manifestation of acute lymphoblastic leukaemia in children. Arch. Dis. Child. 2015, 100, 821–825. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, I.; Creech, C.B. Advances in the diagnosis and management of pediatric osteomyelitis. Curr. Infect. Dis. Rep. 2011, 13, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Pineda, C.; Espinosa, R.; Pena, A. Radiographic imaging in osteomyelitis: The role of plain radiography, computed tomography, ultrasonography, magnetic resonance imaging, and scintigraphy. Semin. Plast. Surg. 2009, 23, 80–89. [Google Scholar] [CrossRef] [PubMed]
- McCarville, M.B.; Chen, J.Y.; Coleman, J.L.; Li, Y.; Li, X.; Adderson, E.E.; Neel, M.D.; Gold, R.E.; Kaufman, R.A. Distinguishing osteomyelitis from Ewing sarcoma on radiography and MRI. Am. J. Roentgenol. 2015, 20, 640–650. [Google Scholar] [CrossRef] [PubMed]
- Connolly, L.P.; Connolly, S.A.; Drubach, L.A.; Jaramillo, D.; Treves, S.T. Acute hematogenous osteomyelitis of children: Assessment of skeletal scintigraphy-based diagnosis in the era of MRI. J. Nucl. Med. 2002, 43, 1310–1316. [Google Scholar] [PubMed]
- British Orthopaedic Association and British Society for Children’s Orthopaedic Surgery. The Management of Acute Bone and Joint Infection in Childhood—A Guide to Good Practice 2013. Available online: http://bscos.org.uk/resources/Downloads/Blue-Book-infection.pdf (accessed on 25 May 2016).
- Peltola, H.; Pääkkönen, M. Acute osteomyelitis in children. New Engl. J. Med. 2014, 370, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Copley, L.A.; Kinsler, A.; Gheen, T.; Shar, A.; Sun, D.; Browne, R. The impact of evidence-based clinical practice guidelines applied by a multidisciplinary team for the care of children with osteomyelitis. J. Bone Joint Surg. Am. 2013, 95, 686–693. [Google Scholar] [CrossRef] [PubMed]
- Hawkshead, J.J.; Patel, N.B.; Steele, R.W.; Heinrich, S.D. Comparative severity of pediatric osteomyelitis attributable to methicillin-resistant versus methicillin-sensitive Staphylococcus aureus. J. Pediatr. Orthop. 2009, 29, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Boyle-Vavra, S.; Daum, R.S. Community-acquired methicillin-resistant Staphylococcus aureus: The role of Panton-Valentine leukocidin. Lab. Investig. 2007, 87, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Tong, S.Y.; Davis, J.S.; Eichenberger, E.; Holland, T.L.; Fowler, V.G., Jr. Staphylococcus aureus Infections: Epidemiology, pathophysiology, clinical manifestations, and management. Clin. Microbiol. Rev. 2015, 28, 603–661. [Google Scholar] [CrossRef] [PubMed]
- Dohin, B.; Gillet, Y.; Kohler, R.; Lina, G.; Vandenesch, F.; Vanhems, P.; Floret, D.; Etienne, J. Pediatric bone and joint infections caused by Panton-Valentine leukocidin-positive Staphylococcus aureus. Pediatr. Infect. Dis. J. 2007, 26, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Dumitrescu, O.; Boisset, S.; Badiou, C.; Bes, M.; Benito, Y.; Reverdy, M.E.; Vandenesch, F.; Etienne, J.; Lina, G. Effect of antibiotics on Staphylococcus aureus producing Panton-Valentine leukocidin. Antimicrob. Agents Chemother. 2007, 51, 1515–1519. [Google Scholar] [CrossRef] [PubMed]
- Zaoutis, T.; Localio, A.R.; Leckerman, K.; Saddlemire, S.; Bertoch, D.; Keren, R. Prolonged intravenous therapy versus early transition to oral antimicrobial therapy for acute osteomyelitis in children. Pediatrics 2009, 123, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Peltola, H.; Pääkkönen, M.; Kallio, P.; Kallio, M.J. Osteomyelitis-Septic Arthritis Study Group: Short- versus long-term antimicrobial treatment for acute hematogenous osteomyelitis of childhood: Prospective, randomized trial on 131 culture-positive cases. Pediatr. Infect. Dis. J. 2010, 29, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Keren, R.; Shah, S.S.; Srivastava, R.; Rangel, S.; Bendel-Stenzel, M.; Harik, N.; Hartley, J.; Lopez, M.; Seguias, L.; Tieder, J.; et al. Pediatric research in inpatient settings network comparative effectiveness of intravenous vs. oral antibiotics for postdischarge treatment of acute osteomyelitis in children. JAMA Pediatr. 2015, 169, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Faust, S.N.; Clark, J.; Pallett, A.; Clarke, N.M. Managing bone and joint infection in children. Arch. Dis. Child. 2012, 97, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Michelow, I.C.; Mandell, J.G. Sequential intravenous oral antibiotic therapy for osteomyelitis: How short is long enough? JAMA Pediatr. 2015, 169, 698–699. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Milstone, A.M. Outpatient antibiotic therapy for acute osteomyelitis in children: Balancing safety and efficacy. JAMA Pediatr. 2015, 169, 108–109. [Google Scholar] [CrossRef] [PubMed]
- Messina, A.F.; Namtu, K.; Guild, M.; Dumois, J.A.; Berman, D.M. Trimethoprim-sulfamethoxazole therapy for children with acute osteomyelitis. Pediatr. Infect. Dis. J. 2011, 30, 1019–1021. [Google Scholar] [CrossRef] [PubMed]
- Tafin-Kampé, K.; Kamsu-Foguem, B. Acute osteomyelitis due to Staphylococcus aureus in children: What is the status of treatment today? Pediatr. Infect. Dis. 2013, 5, 122–126. [Google Scholar] [CrossRef]
- Martin, A.C.; Anderson, D.; Lucey, J.; Guttinger, R.; Jacoby, P.A.; Mok, T.J.; Whitmore, T.J.; Whitewood, C.N.; Burgner, D.P.; Blyth, C.C. Predictors of outcome in pediatric osteomyelitis: Five year experience in a single tertiary center. Pediatr. Infect. Dis. J. 2016, 35, 387–391. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Risk Factors for Long-Term Sequelae |
|---|
| Late diagnosis (>4 days) |
| Inadequate treatment |
| Neonate (prematurity, hypoxia, central venous catheterization) |
| Sickle cell disease |
| Infection by MRSA or Panton-Valentine Leukocidin positive strains |
| Differential Diagnoses |
|---|
| Reactive arthritis |
| Juvenile arthritis |
| Septic arthritis |
| Trauma |
| Cancer (osteoid osteoma, leukemia, eosinophilic granuloma, metastatic neuroblastoma, Ewing’s sarcoma, osteosarcoma) |
| Age Group | Common Pathogens |
|---|---|
| 0–3 months | Staphylococcus aureus |
| Streptococcus agalactiae | |
| Gram negative enteric bacteria | |
| 3 months–4 years | Staphylococcus aureus |
| Streptococcus pyogenes | |
| Kingella kingae | |
| Haemophilus influenzae type b (in non-immunized child) | |
| >5 years | Staphylococcus aureus |
| Streptococcus pyogenes |
| Bacteriology | Antibiotic | Dose mg/kg/die | Maximum Daily Dose | Bone Penetration # |
|---|---|---|---|---|
| If MRSA prevalence in the community <10% | First generation cephalosporin * | 150 divided into 4 equal doses | 2–4 g | 6–7 |
| OR | ||||
| Antistaphylococcal penicillin (cloxacillin, flucloxacilina, dicloxacillin, nafcillin, or oxacillin) | 200 divided into 4 equal doses | 8–12 g | 15–17 | |
| If the prevalence of MRSA in the community >10% and the Prevalence of S. aureus resistant to clindamycin <10% | Clindamycin | 40 divided into 4 equal doses | 3 g | 65–78 |
| If the prevalence of MRSA in community ≥10% and the Prevalence of S. aureus clindamycin resistente ≥10% | Vancomycin | 40 divided into 4 equal doses Or 45 mg divided in 3 equal doses | Dose adjusted according to blood levels with a target of 15–20 μg/mL trough level | 5–67 |
| OR | ||||
| Linezolid if vancomycin is not effective | 30 divided in 3 equal doses | 1.2 g no more than 28 days | 40–51 | |
| Alternatives for specific agents | Ampicillin or amoxicillin for Beta-hemolytic streptococcus group A, Haemophilus influenzae type b (strains which do not produce beta-lactamase, S. pneumoniae sensitive to penicillin | 150–200 dispensed in 4 equal doses | 8–12 g | 3–31 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiappini, E.; Mastrangelo, G.; Lazzeri, S. A Case of Acute Osteomyelitis: An Update on Diagnosis and Treatment. Int. J. Environ. Res. Public Health 2016, 13, 539. https://doi.org/10.3390/ijerph13060539
Chiappini E, Mastrangelo G, Lazzeri S. A Case of Acute Osteomyelitis: An Update on Diagnosis and Treatment. International Journal of Environmental Research and Public Health. 2016; 13(6):539. https://doi.org/10.3390/ijerph13060539
Chicago/Turabian StyleChiappini, Elena, Greta Mastrangelo, and Simone Lazzeri. 2016. "A Case of Acute Osteomyelitis: An Update on Diagnosis and Treatment" International Journal of Environmental Research and Public Health 13, no. 6: 539. https://doi.org/10.3390/ijerph13060539
APA StyleChiappini, E., Mastrangelo, G., & Lazzeri, S. (2016). A Case of Acute Osteomyelitis: An Update on Diagnosis and Treatment. International Journal of Environmental Research and Public Health, 13(6), 539. https://doi.org/10.3390/ijerph13060539