
Interactions between Neighborhood Social Environment and Walkability to Explain Belgian Older Adults’ Physical Activity and Sedentary Time

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling and Procedures
2.2. Measures
2.2.1. Independent Variables
The Neighborhood Social Environment
Physical Environment: GIS-Based Neighborhood Walkability
2.2.2. Outcome Measures
Self-Reported PA and SB
Accelerometer-Based PA and SB
2.2.3. Covariates
2.3. Statistical Analyses
3. Results
3.1. Sample Characteristics
3.2. The Neighborhood Social Environment and PA, and Moderation Effects
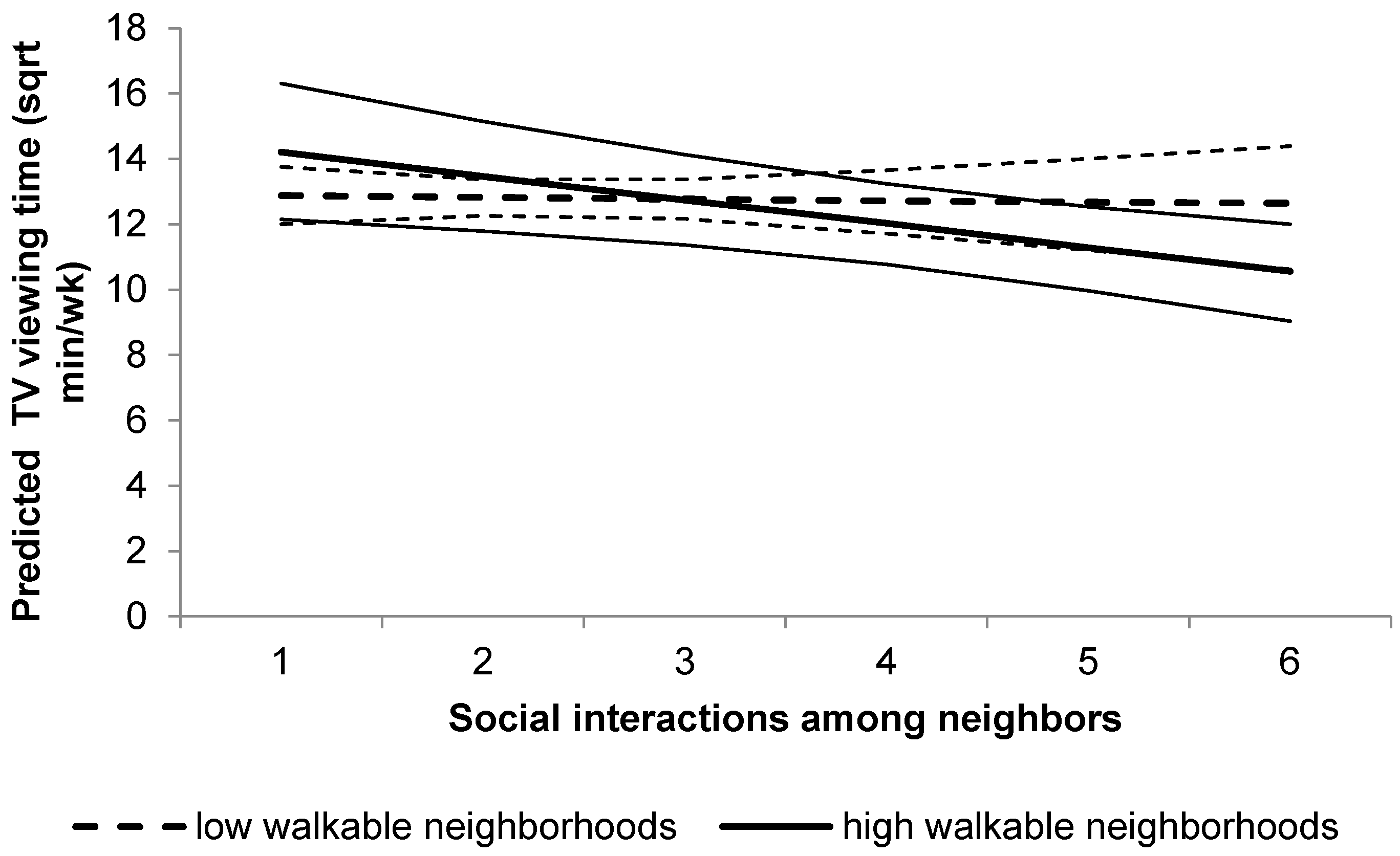
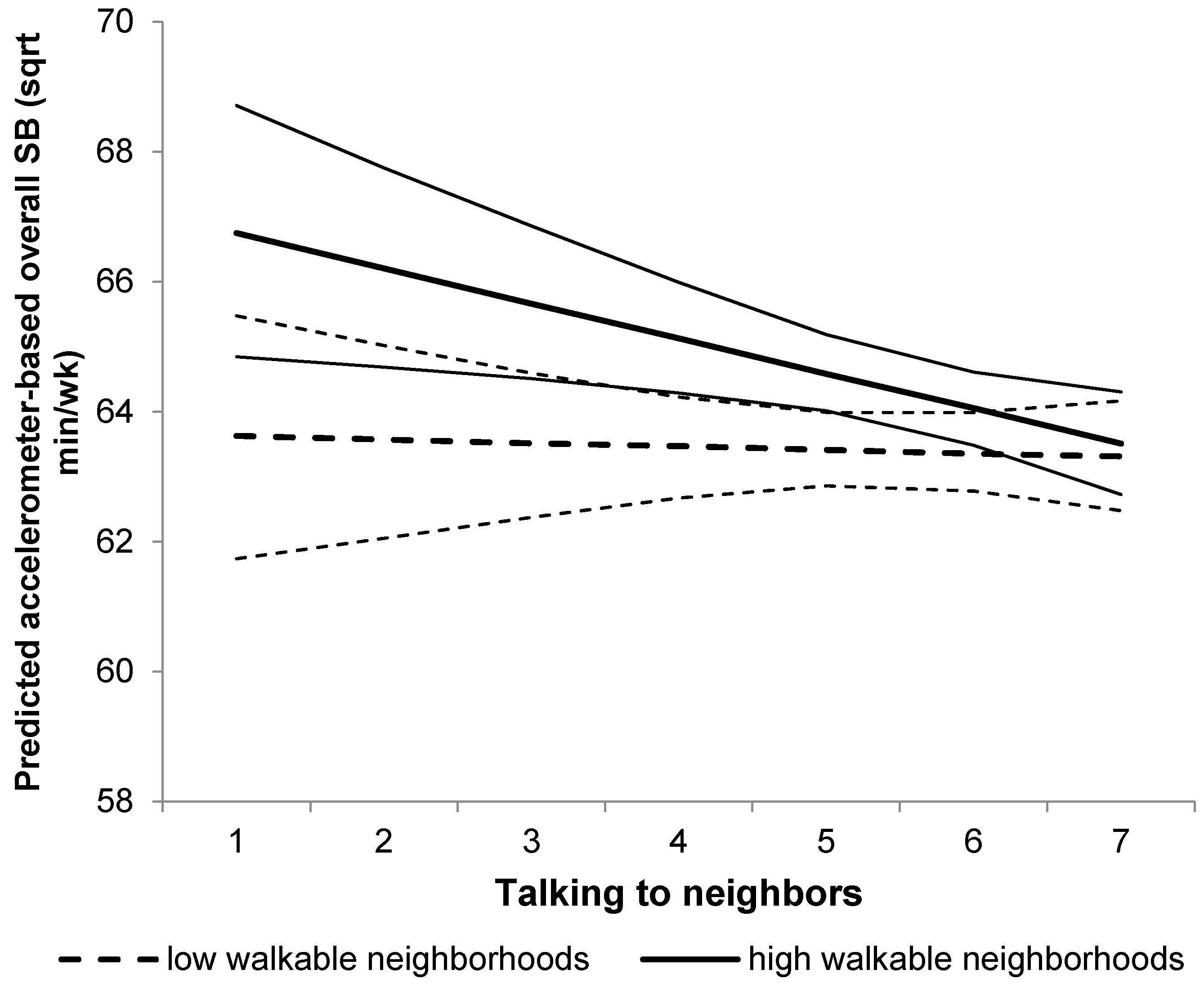
3.3. The Neighborhood Social Environment and SB, and Moderation Effects
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| PA | physical activity |
| MVPA | moderate-to-vigorous physical activity |
| SB | Sedentary behavior |
| GIS | Geographic Information Systems |
References
- Chodzko-Zajko, W.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Tak, E.; Kuiper, R.; Chorus, A.; Hopman-Rock, M. Prevention of onset and progression of basic ADL disability by physical activity in community dwelling older adults: A meta-analysis. Ageing Res. Rev. 2013, 12, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Simonsick, E.M.; Lafferty, M.E.; Phillips, C.L.; Mendes de Leon, C.F.; Kasl, S.V.; Seeman, T.E.; Fillenbaum, G.; Hebert, P.; Lemke, J.H. Risk due to inactivity in physically capable older adults. Am. J. Public Health 1993, 83, 1443–1450. [Google Scholar] [CrossRef] [PubMed]
- Paterson, D.H.; Warburton, D.E. Physical activity and functional limitations in older adults: A systematic review related to Canada’s Physical Activity Guidelines. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 38. [Google Scholar] [CrossRef] [PubMed]
- Rezende, L.F.; Rey-López, J.; Matsudo, V.K.; Luiz, O. Sedentary behavior and health outcomes among older adults: A systematic review. BMC Public Health 2014, 14, 333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helmerhorst, H.J.F.; Wijndaele, K.; Brage, S.; Wareham, N.J. Objectively measured sedentary time may predict insulin resistance independent of moderate- and vigorous-intensity physical activity. Diabetes 2009, 58, 1776–1779. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.K.; Healy, G.N.; Winkler, E.A.H.; Gardiner, P.A.; Sugiyama, T.; Dunstan, D.W.; Matthews, C.E.; Owen, N. Relationship of television time with accelerometer-derived sedentary time: NHANES. Med. Sci. Sports Exerc. 2011, 43, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Chad, K.E.; Reeder, B.A.; Harrison, E.L.; Ashworth, N.L.; Sheppard, S.M.; Schultz, S.L.; Bruner, B.G.; Fisher, K.L.; Lawson, J.A. Profile of physical activity levels in community-dwelling older adults. Med. Sci. Sports Exerc. 2005, 37, 1774–1784. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.W.; Popkin, B.M. Time use and physical activity: A shift away from movement across the globe. Obes. Rev. 2012, 13, 659–680. [Google Scholar] [CrossRef] [PubMed]
- Eurobarometer Sport and Physical Activity. Available online: http://ec.europa.eu/public_opinion/archives/ebs/ebs_334_en.pdf (accessed on 8 April 2014).
- Centers for Disease Control and Prevention U.S. Physical Activity Statistics. Available online: http://apps.nccd.cdc.gov/brfss/age.asp?cat=PA&yr=2009&qkey=4418&state=US (accessed on 19 November 2013).
- Matthews, C.E.; Chen, K.Y.; Freedson, P.S.; Buchowski, M.S.; Beech, B.M.; Pate, R.R.; Troiano, R.P. Amount of time spent in sedentary behaviors in the United States, 2003–2004. Am. J. Epidemiol. 2008, 167, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Doherty, T.J. Invited review: Aging and sarcopenia. J. Appl. Physiol. 2003, 95, 1717–1727. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Owen, N.; Fotheringham, M.J. Behavioral epidemiology: A systematic framework to classify phases of research on health promotion and disease prevention. Ann. Behav. Med. 2000, 22, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Owen, N. Ecological models of health behavior. In Health Behavior. Theory, Research and Practice; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2015. [Google Scholar]
- McNeill, L.H.; Kreuter, M.W.; Subramanian, S.V. Social environment and physical activity: A review of concepts and evidence. Soc. Sci. Med. 2006, 63, 1011–1022. [Google Scholar] [CrossRef] [PubMed]
- Putnam, R.D. Bowling alone: America’s declining social capital. J. Democr. 1995, 6, 65–78. [Google Scholar] [CrossRef]
- Lochner, K.; Kawachi, I.; Kennedy, B.P. Social capital: A guide to its measurement. Health Place 1999, 5, 259–270. [Google Scholar] [CrossRef]
- Fisher, K.J.; Li, F.; Michael, Y.; Cleveland, M. Neighborhood-level influences on physical activity among older adults: A multilevel analysis. J. Aging Phys. Act. 2004, 12, 45–63. [Google Scholar] [PubMed]
- Van Dyck, D.; Teychenne, M.; McNaughton, S.A.; De Bourdeaudhuij, I.; Salmon, J. Relationship of the perceived social and physical environment with mental health-related quality of life in middle-aged and older adults: Mediating effects of physical activity. PLoS ONE 2015, 10, e0120475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Cauwenberg, J.; De Donder, L.; Clarys, P.; De Bourdeaudhuij, I.; Buffel, T.; De Witte, N.; Dury, S.; Verté, D.; Deforche, B. Relationships between the perceived neighborhood social environment and walking for transportation among older adults. Soc. Sci. Med. 2014, 104, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Shimura, H.; Winkler, E.; Owen, N. Individual, psychosocial and environmental correlates of 4-year declines in walking among middle-to-older aged adults. J. Phys. Act. Health 2014, 11, 1078–1084. [Google Scholar] [CrossRef] [PubMed]
- Van Cauwenberg, J.; De Donder, L.; Clarys, P.; De Bourdeaudhuij, I.; Owen, N.; Dury, S.; De Witte, N.; Buffel, T.; Verté, D.; Deforche, B. Relationship of individual, social, and physical environmental factors with older adults’ television viewing time. J. Aging Phys. Act. 2014, 22, 508–517. [Google Scholar] [CrossRef] [PubMed]
- Van Holle, V.; McNaughton, S.; Teychenne, M.; Timperio, A.; Van Dyck, D.; De Bourdeaudhuij, I.; Salmon, J. Social and physical environmental correlates of adults’ weekend sitting time and moderating effects of retirement status and physical health. Int. J. Environ. Res. Public Health 2014, 11, 9790–9810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, B.; Perkins, D.D.; Brown, G. Place attachment in a revitalizing neighborhood: Individual and block levels of analysis. J. Environ. Psychol. 2003, 23, 259–271. [Google Scholar] [CrossRef]
- Brug, J.; Chinapaw, M. Determinants of engaging in sedentary behavior across the lifespan; lessons learned from two systematic reviews conducted within DEDIPAC. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 134. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.D.; Sallis, J.F.; Saelens, B.E.; Leary, L.; Cain, K.; Conway, T.L.; Hess, P.M. The development of a walkability index: Application to the neighborhood quality of life study. Br. J. Sports Med. 2010, 44, 924–933. [Google Scholar] [CrossRef] [PubMed]
- King, A.C.; Sallis, J.F.; Frank, L.D.; Saelens, B.E.; Cain, K.; Conway, T.L.; Chapman, J.E.; Ahn, D.K.; Kerr, J. Aging in neighborhoods differing in walkability and income: Associations with physical activity and obesity in older adults. Soc. Sci. Med. 2011, 73, 1525–1533. [Google Scholar] [CrossRef] [PubMed]
- Van Holle, V.; Van Cauwenberg, J.; Van Dyck, D.; Deforche, B.; Van de Weghe, N.; De Bourdeaudhuij, I. Relationship between neighborhood walkability and older adults’ physical activity: Results from the Belgian Environmental Physical Activity Study in Seniors (BEPAS Seniors). Int. J. Behav. Nutr. Phys. Act. 2014, 11, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kikuchi, H.; Inoue, S.; Sugiyama, T.; Owen, N.; Oka, K.; Shimomitsu, T. Correlates of prolonged television viewing time in older Japanese men and women. BMC Public Health 2013, 13, 213. [Google Scholar] [CrossRef] [PubMed]
- Alfonzo, M.A. To walk or not to walk? The hierarchy of walking needs. Environ. Behav. 2005, 37, 808–836. [Google Scholar] [CrossRef]
- Unger, D.G.; Wandersman, A. The importance of neighbors: The social, cognitive, and affective components of neighboring. Am. J. Community Psychol. 1985, 13, 139–169. [Google Scholar] [CrossRef]
- Sampson, R.J. Neighborhoods and Violent Crime: A Multilevel Study of Collective Efficacy. Science 1997, 277, 918–924. [Google Scholar] [CrossRef] [PubMed]
- Van Dyck, D.; Cardon, G.; Deforche, B.; Sallis, J.F.; Owen, N.; De Bourdeaudhuij, I. Neighborhood SES and walkability are related to physical activity behavior in Belgian adults. Prev. Med. (Baltim) 2010, 50 (Suppl. 1), S74–S79. [Google Scholar] [CrossRef] [PubMed]
- Owen, N.; Humpel, N.; Leslie, E.; Bauman, A.; Sallis, J.F. Understanding environmental influences on walking: Review and research agenda. Am. J. Prev. Med. 2004, 27, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Giles-Corti, B.; Timperio, A.; Bull, F.; Pikora, T. Understanding physical activity environmental correlates: Increased specificity for ecological models. Exerc. Sport Sci. Rev. 2005, 33, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Owen, N.; Sugiyama, T.; Eakin, E.E.; Gardiner, P.A.; Tremblay, M.S.; Sallis, J.F. Adults’ sedentary behavior determinants and interventions. Am. J. Prev. Med. 2011, 41, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.M.; Schwarz, U.; Skelton, D.A. Development of a consensus taxonomy of sedentary behaviors (SIT): Report of Delphi round 1. PLoS ONE 2013, 8, 1–16. [Google Scholar] [CrossRef] [PubMed]
- The International Physical Activity Questionnaire (IPAQ). Available online: http://www.ipaq.ki.se/ (accessed on 15 September 2010).
- Van Holle, V.; De Bourdeaudhuij, I.; Deforche, B.; Van Cauwenberg, J.; Van Dyck, D. Assessment of physical activity in older Belgian adults: Validity and reliability of an adapted interview version of the long International Physical Activity Questionnaire (IPAQ-L). BMC Public Health 2015, 15, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murtagh, E.M.; Murphy, M.H.; Boone-Heinonen, J. Walking: The first steps in cardiovascular disease prevention. Curr. Opin. Cardiol. 2010, 25, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Siegel, P.Z.; Brackbill, R.M.; Heath, G.W. The epidemiology of walking for exercise: Implications for promoting activity among sedentary groups. Am. J. Public Health 1995, 85, 706–710. [Google Scholar] [CrossRef] [PubMed]
- Van Cauwenberg, J.; Van Holle, V.; De Bourdeaudhuij, I.; Owen, N.; Deforche, B. Older adults’ reporting of specific sedentary behaviors: Validity and reliability. BMC Public Health 2014, 14, 734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahlqvist, S.; Song, Y.; Ogilvie, D. Is active travel associated with greater physical activity? The contribution of commuting and non-commuting active travel to total physical activity in adults. Prev. Med. (Baltim) 2012, 55, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Melanson, E.L.; Freedson, P.S. Validity of the Computer Science and Applications, Inc. (CSA) activity monitor. Med. Sci. Sports Exerc. 1995, 27, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Copeland, J.L.; Esliger, D.W. Accelerometer assessment of physical activity in active, healthy older adults. J. Aging Phys. Act. 2009, 17, 17–30. [Google Scholar] [PubMed]
- Pruitt, L.A.; Glynn, N.W.; King, A.C.; Guralnik, J.M.; Aiken, E.K.; Miller, G.; Haskell, W.L. Use of accelerometry to measure physical activity in older adults at risk for mobility disability. J. Aging Phys. Act. 2008, 16, 416–434. [Google Scholar] [PubMed]
- Cain, K.L.; Geremia, C.M. Accelerometer Data Collection and Scoring Manual For Adult & Senior Studies. Available online: http://www.drjamessallis.sdsu.edu/Documents/Accelerometer_Data_Collection_and_Scoring_Manual_Cain&Geremia_Updated_July2011.pdf (accessed on 2 November 2015).
- Van Cauwenberg, J.; Van Holle, V.; De Bourdeaudhuij, I.; Van Dyck, D.; Deforche, B. Neighborhood walkability and health outcomes among older adults: The mediating role of physical activity. Health Place 2016, 37, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Choi, L.; Ward, S.C.; Schnelle, J.F.; Buchowski, M.S. Assessment of wear/nonwear time classification algorithms for triaxial accelerometer. Med. Sci. Sports Exerc. 2012, 44, 2009–2016. [Google Scholar] [CrossRef] [PubMed]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the Computer Science and Applications, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36): I. conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.D.; Saelens, B.E.; Powell, K.E.; Chapman, J.E. Stepping towards causation: Do built environments or neighborhood and travel preferences explain physical activity, driving, and obesity? Soc. Sci. Med. 2007, 65, 1898–1914. [Google Scholar] [CrossRef] [PubMed]
- Twisk, J.W.R. Applied Multilevel Analysis; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar]
- Day, R. Local environments and older people’s health: Dimensions from a comparative qualitative study in Scotland. Health Place 2008, 14, 299–312. [Google Scholar] [CrossRef] [PubMed]
- Van Cauwenberg, J.; Van Holle, V.; Simons, D.; Deridder, R.; Clarys, P.; Goubert, L.; Nasar, J.; Salmon, J.; De Bourdeaudhuij, I.; Deforche, B. Environmental factors influencing older adults’ walking for transportation: A study using walk-along interviews. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmood, A.; Chaudhury, H.; Michael, Y.L.; Campo, M.; Hay, K.; Sarte, A. A photovoice documentation of the role of neighborhood physical and social environments in older adults’ physical activity in two metropolitan areas in North America. Soc. Sci. Med. 2012, 74, 1180–1192. [Google Scholar] [CrossRef] [PubMed]
- Moran, M.; Van Cauwenberg, J.; Hercky-Linnewiel, R.; Cerin, E.; Deforche, B.; Plaut, P. Understanding the relationships between the physical environment and physical activity in older adults: a systematic review of qualitative studies. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lund, H. Testing the claims of new urbanism: Local access, pedestrian travel, and neighboring behaviors. J. Am. Plan. Assoc. 2003, 69, 414–429. [Google Scholar] [CrossRef]
- Stathi, A.; Fox, K.R.; McKenna, J. Physical activity and dimensions of subjective well-being in older adults. J. Aging Phys. Act. 2002, 10, 76–92. [Google Scholar]
- De Donder, L.; De Witte, N.; Buffel, T.; Dury, S.; Verte, D. Social capital and feelings of unsafety in later life: A study on the influence of social networks, place attachment, and civic participation on perceived safety in Belgium. Res. Aging 2012, 34, 425–448. [Google Scholar] [CrossRef]
- Foster, S.; Giles-Corti, B. The built environment, neighborhood crime and constrained physical activity: An exploration of inconsistent findings. Prev. Med. (Baltim) 2008, 47, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Van Cauwenberg, J.; Clarys, P.; De Bourdeaudhuij, I.; Van Holle, V.; Verté, D.; De Witte, N.; De Donder, L.; Buffel, T.; Dury, S.; Deforche, B. Older adults’ transportation walking: A cross-sectional study on the cumulative influence of physical environmental factors. Int. J. Health Geogr. 2013, 12, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, D. Neighborhood and individual factors in activity in older adults: Results From the neighbourhood and senior health study. J. Aging Phys. Act. 2008, 16, 144–170. [Google Scholar] [PubMed]
- Mollenkopf, H.; Marcellini, F.; Ruoppila, I.; Flaschenträger, P.; Gagliardi, C.; Spazzafumo, L. Outdoor mobility and social relationships of elderly people. Arch. Gerontol. Geriatr. 1997, 24, 295–310. [Google Scholar] [CrossRef]
- Van Dyck, D.; Cardon, G.; Deforche, B.; De Bourdeaudhuij, I. IPAQ interview version: Convergent validity with accelerometers and comparison of physical activity and sedentary time levels with the self-administered version. J. Sports Med. Phys. Fit. 2015, 55, 776–786. [Google Scholar]
- Matthews, C.E. Use of self-report instruments to assess physical activity. In Physical Activity Assessments for Health-Related Research; Welk, G.J., Ed.; Human Kinetics: Champaign, IL, USA, 2002; pp. 107–123. [Google Scholar]
- Rikli, R.E. Reliability, validity, and methodological issues in assessing physical activity in older adults. Res. Q. Exerc. Sport 2000, 71, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Kwan, M.; Woo, J.; Kwok, T. The standard oxygen consumption value equivalent to one metabolic equivalent (3.5 mL/min/kg) is not appropriate for elderly people. Int. J. Food Sci. Nutr. 2004, 55, 179–182. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Statistics-Belgium FOD Economie, Kleine en Middelgrote Ondernemingen, Middenstand en Energie. Available online: http://statbel.fgov.be/nl/statistieken/cijfers/arbeid_leven/opleiding/niveau/ (accessed on 10 December 2015).




{kind=link}
{kind=link}
{kind=link}
| Socio-Demographics | N = 431 | |
|---|---|---|
| Gender (% female) | 54.5 | |
| Age in years (M ± SD) | 74.4 ± 6.2 | |
| Living situation (% with partner) | 65.5 | |
| Educational level (% tertiary) | 38.3 | |
| Former occupation (%) | ||
| household | 18.5 | |
| blue collar | 26.4 | |
| white collar | 55.1 | |
| Neighborhood Social Environment | M ± SD | Range |
| Talking to neighbors 1 (/7) | 5.5 ± 1.4 | 1.0–7.0 |
| Social interactions among neighbors 1 (/7) | 2.2 ± 1.1 | 1.0–6.3 |
| Social trust and cohesion neighborhood 1 (/5) | 3.7 ± 0.8 | 1.0–5.0 |
| Social diversity neighborhood 2 (/5) | 4.2 ± 0.7 | 1.7–5.0 |
| Dependent variables | M ± SD | MED; IQR |
| Transport walking3 (min·week−1) | 86.8 ± 141.9 | 30.0; 0.0–120.0 |
| Recreational walking3 (min·week−1) | 83.2 ± 159.3 | 0.0; 0.0–120.0 |
| TV3 (min·week−1) | 1191.4 ± 738.5 | 1260.0; 630.0–1680.0 |
| MVPA4 (min·week−1) | 111.7 ± 117.2 | 72.0; 23.3–165.0 |
| Sedentary behavior 4 (min·week−1) | 4039.1 ± 708.0 | 4109.5; 3581.3–4565.3 |
| Social Environment Factor | Main Effect Walkability | Main Effect Income (Ref. = Low) | Main Effect Soc. Env. Factor | Income × Walkability | Income × Soc. Env. Factor | Walkability × Soc. Env. Factor | Walkability × Income × Soc. Env. Factor |
|---|---|---|---|---|---|---|---|
| B ± SE | B ± SE | B ± SE | B ± SE | B ± SE | B ± SE | B ± SE | |
| 2.31 ± 1.70 | 0.43 ± 0.75 | −1.82 ± 1.08 ¥ | |||||
| Interactions neighbors | 0.20 ± 0.46 | −0.65 ± 0.62 | −0.18 ± 0.68 | 0.96 ± 0.92 | |||
| Social trust &cohesion | 0.67 ± 0.61 | −0.24 ± 0.89 | −1.71 ± 0.85 * | 2.20 ± 1.21 ¥ |
| Independent Variables | Walking Transport 1 | Walking Recreation 1 | Overall SB 2 | TV Viewing 3 |
|---|---|---|---|---|
| Multivariable Model | Multivariable Model | Multivariable Model | Multivariable Model | |
| B ± SE | B ± SE | B ± SE | B ± SE | |
| Main effects | ||||
| Talking to neighbors | 0.68 ± 0.23 * | 0.80 ± 0.27 * | ||
| Neighborhood social diversity | 0.98 ± 0.54 ¥ | −0.44 ± 0.28 | ||
| Interactions | ||||
| Walkability × talking to neighbors | −0.56 ± 0.30 ¥ | |||
| Walkability × social interactions among neighbors | −0.65 ± 0.36 ¥ | |||
| Walkability × social diversity | 2.31 ± 0.90 * | |||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Holle, V.; Van Cauwenberg, J.; De Bourdeaudhuij, I.; Deforche, B.; Van de Weghe, N.; Van Dyck, D. Interactions between Neighborhood Social Environment and Walkability to Explain Belgian Older Adults’ Physical Activity and Sedentary Time. Int. J. Environ. Res. Public Health 2016, 13, 569. https://doi.org/10.3390/ijerph13060569
Van Holle V, Van Cauwenberg J, De Bourdeaudhuij I, Deforche B, Van de Weghe N, Van Dyck D. Interactions between Neighborhood Social Environment and Walkability to Explain Belgian Older Adults’ Physical Activity and Sedentary Time. International Journal of Environmental Research and Public Health. 2016; 13(6):569. https://doi.org/10.3390/ijerph13060569
Chicago/Turabian StyleVan Holle, Veerle, Jelle Van Cauwenberg, Ilse De Bourdeaudhuij, Benedicte Deforche, Nico Van de Weghe, and Delfien Van Dyck. 2016. "Interactions between Neighborhood Social Environment and Walkability to Explain Belgian Older Adults’ Physical Activity and Sedentary Time" International Journal of Environmental Research and Public Health 13, no. 6: 569. https://doi.org/10.3390/ijerph13060569
APA StyleVan Holle, V., Van Cauwenberg, J., De Bourdeaudhuij, I., Deforche, B., Van de Weghe, N., & Van Dyck, D. (2016). Interactions between Neighborhood Social Environment and Walkability to Explain Belgian Older Adults’ Physical Activity and Sedentary Time. International Journal of Environmental Research and Public Health, 13(6), 569. https://doi.org/10.3390/ijerph13060569