
Simultaneous Training for Children with Autism Spectrum Disorder and Their Parents with a Focus on Social Skills Enhancement

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Characteristics of Children
2.3. STSSE Procedure
2.4. STSSE Content
2.5. Evaluation Methods
2.5.1. SS-Scale for Education
2.5.2. CBCL Japanese Version
2.5.3. FFFS, Japanese First Version
2.5.4. The Confidence Degree Questionnaire (CDQ) for Families
2.5.5. The Mothers’ Comments
2.6. Ethical Considerations
2.7. Statistical Analysis
3. Results
3.1. Changes in SS-Scale for Education
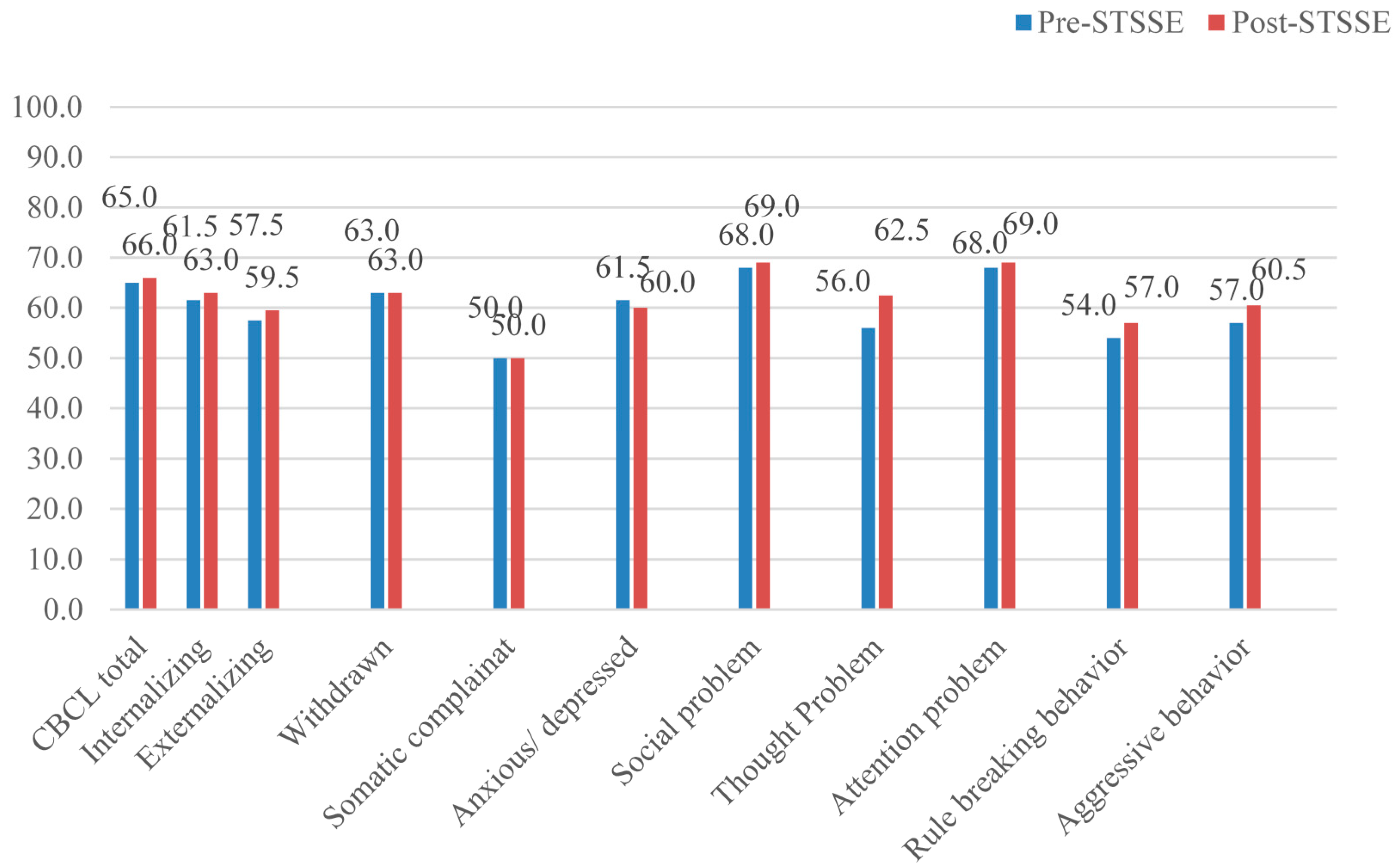
3.2. Changes in CBCL Scores
3.3. Changes in FFFS Scores
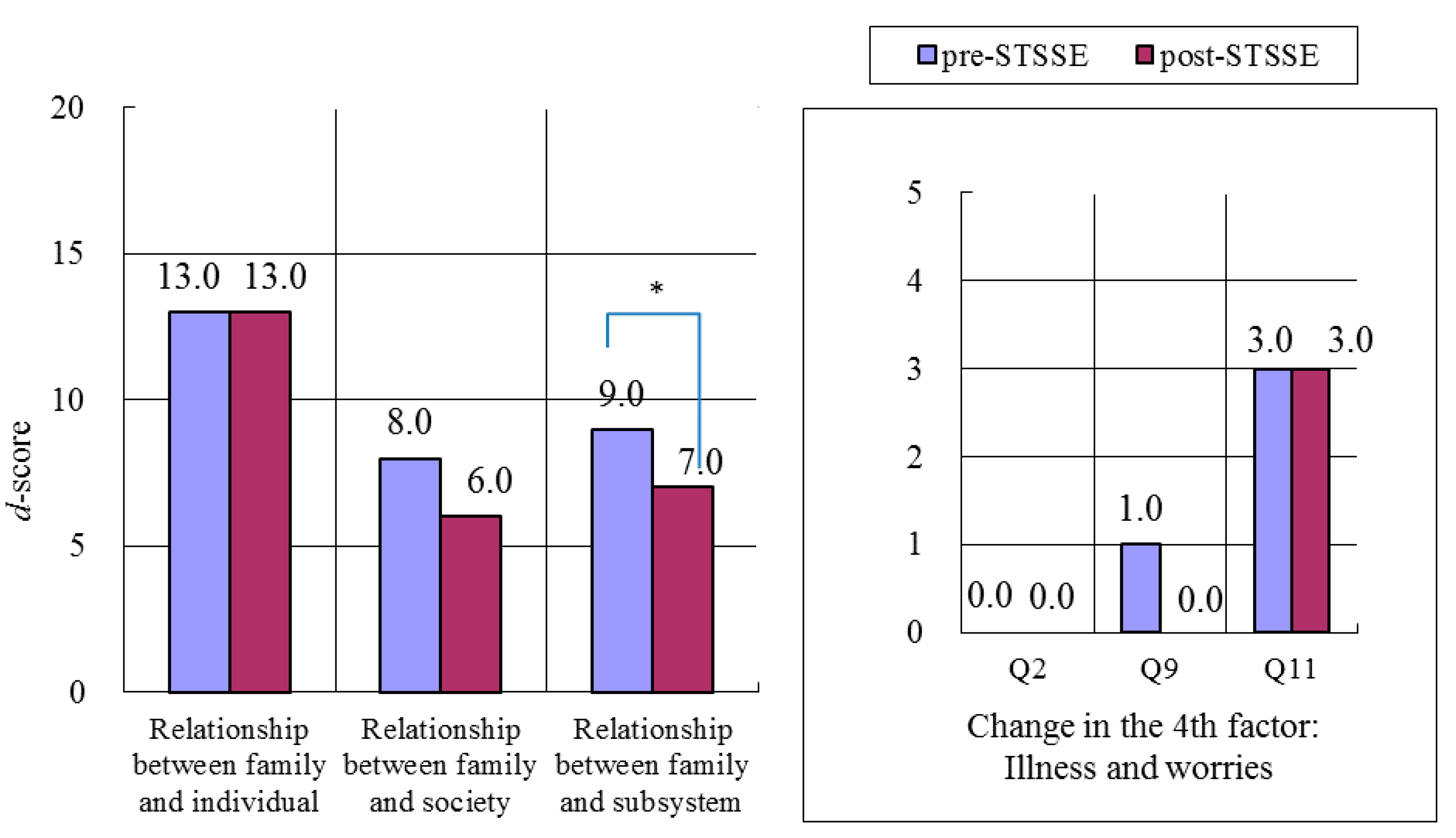
3.3.1. Mothers
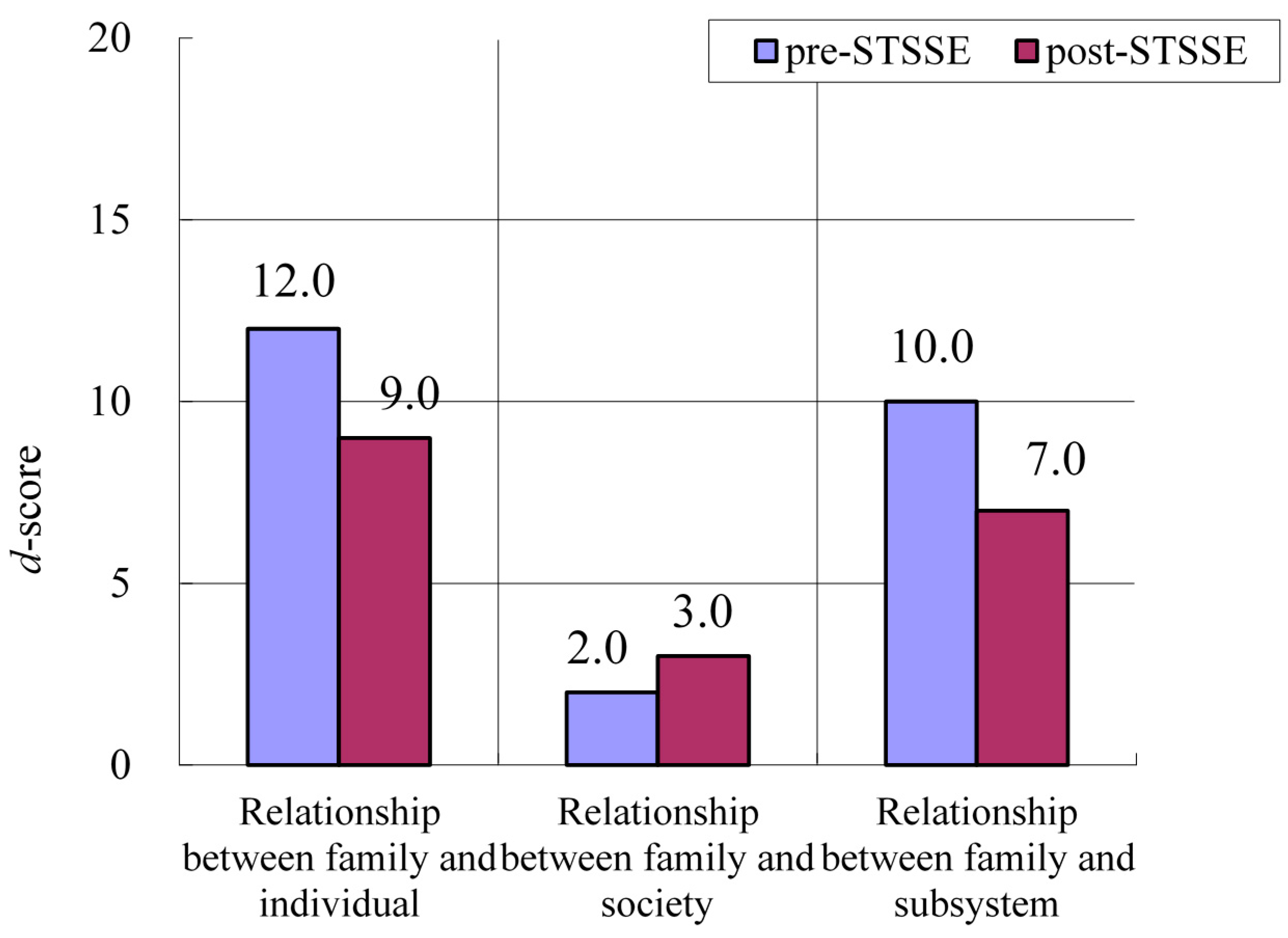
3.3.2. Fathers
3.4. Changes in CDQ Scores
3.4.1. Mothers
3.4.2. Fathers
3.5. The Mothers’ Comments
4. Discussion
4.1. Changes in Children
4.2. Changes in Parents
4.3. The Usefulness of STSSE
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Rubin, K.H.; Dwyer, K.M.; Kim, A.H.; Burgess, K.B.; Booth-Laforce, C.; Rose-Krasnor, L. Attachment, friendship, and psychosocial functioning in early adolescence. J. Early Adolesc. 2004, 24, 326–356. [Google Scholar] [CrossRef] [PubMed]
- Koenig, K.; White, S.; Pachler, M.; Lau, M.; Lewis, M.; Klin, A.; Scahill, L. Promoting social skill development in children with pervasive developmental disorders: A feasibility and efficacy study. J. Autism. Dev. Disord. 2010, 40, 1209–1218. [Google Scholar] [CrossRef] [PubMed]
- Elliott, S.N.; Gresham, F.M. Children’s social skills: Assessment and classification practices. J. Couns. Dev. 1987, 66, 96–99. [Google Scholar] [CrossRef]
- Barnhill, G.P. Social attributions and depression in adolescents with Asperger Syndrome. Focus. Autism. Other. Dev. Disabl. 2001, 16, 46–53. [Google Scholar] [CrossRef]
- Pelham, W.E., Jr.; Lang, A.R.; Atkeson, B.; Murphy, D.A.; Gnagy, E.M.; Greiner, A.R.; Vodde-Hamilton, M.; Greenslade, K.E. Effects of deviant child behavior on parental alcohol consumption: Stress-induced drinking in parents of ADHD children. Am. J. Addict. 1998, 7, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Dishion, T.J.; Andrews, D.W. Preventing escalation in problem behaviors with high-risk young adolescents: Immediate and 1-year outcomes. J. Consult. Clin. Psychol. 1995, 63, 538–548. [Google Scholar] [CrossRef] [PubMed]
- Okuno, H.; Nagai, T.; Sakai, S.; Mohri, I.; Yamamoto, T.; Yoshizaki, A.; Kato, K.; Tachibana, M.; Iwasaka, H.; Taniike, M. Effectiveness of modified parent training for mothers of children with Pervasive Developmental Disorder on parental confidence and children’s behavior. Brain Dev. 2011, 33, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Bierman, K.L. Improving the peer relationships of rejected children. In Advances in Clinical Psychology; Lahey, B.B., Kazdin, A.E., Eds.; Plenum Press: New York, NY, USA, 1989; Volume 12, pp. 53–84. [Google Scholar]
- Kazdin, A.E.; Esveldt, D.K.; French, N.H.; Unis, A.S. Effects of parent management training and problem-solving skills training combined in the treatment of antisocial child behavior. J. Am. Acad. Child Adolesc. Psychiatry 1987, 26, 416–424. [Google Scholar] [CrossRef] [PubMed]
- Lochman, J.E.; Dunn, S.E. An intervention and consultation model from a social cognitive perspective: A description of the anger coping program. School Psychol. Rev. 1993, 22, 458–471. [Google Scholar]
- Shure, M. I Can Problem Solve (ICPS): An Interpersonal Cognitive Problem-Solving Program for Children; Research Press: Champaign, IL, USA, 2001. [Google Scholar]
- Harris, S.L.; Handleman, J.S.; Arnold, M.S.; Gordon, R.F. The Douglass developmental disabilities center: Two models of service delivery. In Preschool Education Programs for Children and Their Families, 2nd ed.; Handleman, J.S., Harris, S.L., Eds.; Pro-Ed: Austin, TX, USA, 2000; pp. 233–260. [Google Scholar]
- Lvaas, O.I.; Smith, T. Early and intensive behavioral intervention in autism. In Evidence-Based Psychotherapies for Children and Youth; Kazdin, A.E., Weisz, J., Eds.; Guildford: New York, NY, USA, 2003; pp. 325–340. [Google Scholar]
- National Research Council. Educating children with autism. Committee on Educational Intervention for children with Autism. In Division of Behavioral and Social Sciences and Education; Lord, C., McGee, J.P., Eds.; National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- Romancyk, R.; Lockshin, S.; Matey, L. The children’s unit for treatment and evaluation. In Preschool Education Programs for Children and Their Families, 2nd ed.; Handelman, J.S., Harris, S.L., Eds.; Pro-Ed: Austin, TX, USA, 2000; pp. 49–94. [Google Scholar]
- DeRosier, M.E.; Swick, D.C.; Davis, N.O.; McMillen, J.S.; Matthews, R. The efficacy of a Social Skills Group Intervention for improving social behaviors in children with High Functioning Autism Spectrum disorders. J. Autism Dev. Disord. 2011, 41, 1033–1043. [Google Scholar] [CrossRef] [PubMed]
- Ventola, P.; Friedman, H.E.; Anderson, L.C.; Wolf, J.M.; Oosting, D.; Foss-Feig, J.; McDonald, N.; Volkmar, F.; Pelphrey, K.A. Improvements in social and adaptive functioning following short-duration PRT program: A clinical replication. J. Autism Dev. Disord. 2014, 44, 2862–2870. [Google Scholar] [CrossRef] [PubMed]
- Solomon, M.; Goodlin-Jones, B.L.; Anders, T.F. A social adjustment enhancement intervention for high functioning autism, Asperger’s syndrome, and pervasive developmental disorder NOS. J. Autism Dev. Disord. 2004, 34, 649–668. [Google Scholar] [CrossRef] [PubMed]
- Ekas, N.V.; Lickenbrock, D.M.; Whitman, T.L. Optimism, social support, and well-being in mothers of children with autism spectrum disorder. J. Autism. Dev. Disord. 2010, 40, 1274–1284. [Google Scholar] [CrossRef] [PubMed]
- Cox, M.J.; Paley, B. Families as systems. Annu. Rev. Psychol. 1997, 48, 243–267. [Google Scholar] [CrossRef] [PubMed]
- Tanaka Institute for Educational Research. Tanaka Binet Chinou Kensa V [Tanaka-Binet Intelligence Scale V]; Taken Publishing: Tokyo, Japan, 2003. [Google Scholar]
- Shimazu, M.; Ikuzawa, M.; Nakase, A. Manual of the Kyoto Scale of Psychological Development; Kyoto Kokusai Shakai Fukushi Center: Kyoto, Japan, 1983. [Google Scholar]
- Butter, E.M. Parent training for children with pervasive developmental disorders: A multi-site feasibility trial. Behav. Interv. 2007, 22, 179–199. [Google Scholar]
- Iwasaka, H.; Shimizu, T.; Iida, J.; Kawabata, Y.; Chikaike, M.; Onishi, T.; Kishimoto, T. Efficacy of a parenting program as attention deficit/hyperactivity disorder (AD/HD) therapy (in Japanese). Jido Seinen Seishin Igaku To Sono Kinsetsu Ryoiki 2002, 43, 483–497. [Google Scholar]
- Webster-Stratton, C. The Incredible Years Training Series. Available online: http://www.ncjrs.gov/pdffiles1/ojjdp/173422.pdf (accessed on 12 August 2015).
- Ueno, K.; Okada, S. Tokubetu Shienn Kyouiku (Jissenn) Social Skill Manual; Matuzawa Insatsu Kabushikigaisya: Tokyo, Japan, 2006. [Google Scholar]
- Achenbach, T.M.; Edelbrock, C. Manual for the Child Behavior Checklist and Revised Child Behavior Profile; University of Vermont Department of Psychiatry: Burlington, VT, USA, 1983. [Google Scholar]
- Hohashi, N.; Maeda, M.; Sugishita, C. Development of the Japanese language Feetham Family Functioning Survey (FFFS) and evaluation of its effectiveness (in Japanese). Jpn. J. Res. Fam. Nurs. 2000, 6, 2–10. [Google Scholar]
- Feetham, S.L.; Meister, S.; Bell, J.; Gilliss, C.L. The Nursing of Families: Theory, Research, Education, Practice, 4th ed.; SAGE Publications, Inc.: Newbury Park, CA, USA, 1993. [Google Scholar]
- Webster-Stratton, C.; Reid, J.; Hammond, M. Social skills and problem-solving training for children with early-onset conduct problems: Who benefits? J. Child Psychol. Psychiatry 2001, 42, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Mclntyre, L.L. Parent training for young children with developmental disabilities: Randomized controlled trial. Am. J. Ment Retard. 2008, 113, 356–368. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T. Infant and preschool developmental screening for early care (in Japanese). Nyuyoji Igaku Shinrigaku Kenkyu 1996, 5, 1–18. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mothers (n = 17) | n | Mean (± SD) | Range | |
|---|---|---|---|---|
| Age (years) | 40.7 ± 3.3 | 35.0–49.0 | ||
| Marital status | ||||
| Married | 17 | |||
| Living with partner | 17 | |||
| Educational level | ||||
| University education | 11 | |||
| Work status | ||||
| Working part or full time | 7 | |||
| Fathers (n = 9) | ||||
| Age (years) | 43.7 ± 4.2 | 37.0–52.0 | ||
| Educational level | ||||
| University education | 5 | |||
| Work status | ||||
| Working full-time | 9 | |||
| Sibling | ||||
| Sibling present | 10 | |||
| Age (years) | 1–29 | |||
| Gender | Male | 4 | ||
| Female | 8 | |||
| Sibling with developmental disorders | 1 | * | ||
| Sibling quarreling with child | 5 | |||
| Sibling having trouble at school | 9 | |||
| Case Number | Age (y/m) | Sex | Main Behavioral Problems | Test Battery | IQ/DQ | |
|---|---|---|---|---|---|---|
| FIQ/Total DQ | VIQ/PIQ, P-M.C-A,L-S, etc. | |||||
| 1 | 7 y 4 m | M | 2, 3, 4, 5, 6, 7, 8 | Tanaka Binet | 76 | |
| 2 | 8 y 3 m | F | 1, 2, 5, 7, 9 | KSPD | 96 | C-A100, L-S93 |
| 3 | 7 y 6 m | F | 1, 2, 5, 7 | KSPD | 90 | C-A92, L-S84 |
| 4 | 9 y 8 m | F | 5, 7 | WISC-III | 60 | VIQ63, PIQ64 |
| 5 | 8 y 3 m | F | 1, 3, 4 | WISC-III | 92 | VIQ96, PIQ89 |
| 6 | 9 y 10 m | M | 2 | WISC-III | 83 | VIQ76, PIQ57 |
| 7 | 7 y 6 m | M | 2, 5, 7 | WISC-III | 101 | VIQ104, PIQ99 |
| 8 | 9 y 6 m | F | 2, 3, 4, 7 | KSPD | 68 | C-A61, L-S76 |
| 9 | 9 y 8 m | M | 1, 4, 5, 10 | WISC-III | 76 | VIQ82, PIQ75 |
| 10 | 8 y 8 m | M | 1, 2, 3, 4, 5, 7, 9 | WISC-III | 90 | VIQ82, PIQ100 |
| 11 | 7 y 11 m | M | 2, 3, 4, 5, 7, 9 | WIPPSI | 79 | VIQ86, PIQ80 |
| 12 | 8 y 3 m | M | 5, 7 | KSPD | C-A86, L-S76 | |
| 13 | 10 y 1 m | M | 1, 2, 4, 7, 10 | WISC-III | 89 | VIQ105, PIQ73 |
| 14 | 8 y 6 m | F | 2, 5, 7 | WISC-III | 100 | VIQ85, PIQ114 |
| 15 | 8 y 3 m | M | 5 | WISC-III | 100 | VIQ97, PIQ103 |
| 16 | 7 y 6 m | M | 2, 3, 7, 9 | KSPD | 93 | C-A88, L-S98 |
| 17 | 7 y 8 m | M | 2, 3, 5, 6, 7, 9 | KSPD | 93 | C-A86, L-S100 |
| Section | Children | Parents |
|---|---|---|
| Session 1: Understanding the greeting method | ・Skill in addressing people (Keeping a suitable distance and maintaining eye contact, turn-taking in speaking) | ・Understanding the general features of ASD and the principles of social skill training ・Identifying good social behavior in the child and understanding ways to give praise ・Understanding the skill of initiating engagement and cooperating with friends at school, etc. |
| Session 2: Understanding how to extend play invitations | ・Skill at the time of starting a peer relationship (Adjusting speaking volume, suitable speech, and proper methods of refusal) | ・Learning how to encourage the behaviors needed by children and the required skills toward appropriate interactions with friends and relations |
| Session 3: Understanding how to ask for help | ・Skill in asking others for assistance when necessary ・Conveying gratitude with respect to speaking volume, suitable speech, and proper methods of refusal | ・Learning how to encourage the skill required to ask for assistance |
| Session 4: Understanding warm behavior | ・Affirmative influence ・Classification of “affable” and “cruel” words | ・Noticing and monitoring appropriate behaviors and rewards ・Rewarding the child for their appropriate behaviors through praise, attention, and physical contact |
| Session 5: Understanding warm behavior | ・Affirmative influence ・Learning scene-specific “heart-warming words” | ・Understanding the skills required for conversation with a good friend or relation |
| Session 6: Understanding conversation skills | ・Skills regarding turn-taking and eye contact in speaking | ・Utilizing self-control techniques for emotional management ・Understanding how to urge the child to use the skills aimed at acquiring self-control |
| Session 7: Understanding emotions | ・Matching expressions and feelings by learning about the relationship between an event and its associated emotions | |
| Session 8: Understanding emotions | ・Levels of feeling ・Learning about grades of feeling | |
| Session 9: Understanding emotions | ・Feelings of control ・Relaxation techniques | |
| Session 10: Farewell party | ・Participating in a game with a high level of difficulty ・Affirmative evaluation of participation | ・Reviewing all previous sessions and preparing an environment designed to reduce inappropriate behaviors ・Learning how to cooperate with school and society |
| CDQ Questions | Mother (n = 17) | Father (n = 9) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre–STSSE | Post–STSSE | p | Pre–STSSE | Post–STSSE | p | ||||||
| Median | IOR | Median | IOR | Median | IOR | Median | IOR | ||||
| Q1 | Do you watch your child’s growth without becoming impatient? | 3 | 3–4 | 4 | 3–4 | 0.83 | 4 | 4–4 | 4 | 3.5–4 | 0.41 |
| Q2 | Do you accept your child’s diagnosis of ASD? | 4 | 4–5 | 4 | 3.5–5 | 0.68 | 4 | 3.5–4.5 | 4 | 3.5–5 | 0.49 |
| Q3 | Do you let your child do what he/she can do by him/herself? | 4 | 4–5 | 4 | 4–5 | 1 | 4 | 4–5 | 4 | 3.5–4.5 | 0.16 |
| Q4 | Do you praise your child once or more a day? | 4 | 4–5 | 4 | 4–5 | 0.74 | 3 | 3–4.5 | 4 | 2.5–5 | 0.41 |
| Q5 | Do you prepare a place where your child can relax? | 4 | 4–5 | 4 | 4–5 | 0.41 | 3.5 | 3–4 | 4 | 3–5 | 0.32 |
| Q6 | Do you help your child to make friends? | 4 | 3–4.5 | 4 | 3–4 | 0.53 | 3 | 2–4 | 3 | 2–4 | 1 |
| Q7 | Can you cope with your child’s inappropriate behavior? | 4 | 3–4 | 4 | 3–4.5 | 0.09 | 4 | 2.5–4 | 3 | 2.5–4 | 1 |
| Q8 | Do you communicate adequately with the school about your child’s problems in school? | 4 | 3.5–4 | 4 | 4–5 | 0.07 | 4 | 2.5–4 | 3 | 2.5–4 | 0.68 |
| Q9 | Do you blame yourself less for having a child with ASD? | 4 | 3–4.5 | 4 | 3–4.5 | 1 | 4 | 3–4 | 3 | 2.5–4 | 0.24 |
| Q10 | Are you less worried about your child? | 3 | 2–4 | 3 | 2–4 | 0.43 | 3 | 3–4 | 3 | 2–4 | 0.32 |
| Q11 | Do you spend time on your own health or enjoyment? | 4 | 2.5–4.5 | 4 | 2.5–4.5 | 0.61 | 3 | 3–4 | 3 | 3–4 | 1 |
| Q12 | Do you quarrel less with your family due to your child’s behavior? | 3 | 2.5–4 | 4 | 3–4 | 0.01 * | 3 | 2–4 | 4 | 3–4 | 0.53 |
| Q13 | Do you ask your family members to assist your child? | 3 | 2–4 | 3 | 2–4 | 0.59 | 3 | 2.5–3.5 | 3 | 2–4 | 0.79 |
| Q14 | Do you consult your family or friends about your troubles and not worry by yourself? | 4 | 3–5 | 4 | 3–5 | 0.41 | 4 | 3–4 | 3 | 3–4 | 0.23 |
| Q15 | Do you share your feelings with families who have children with a similar problem? | 4 | 4–5 | 4 | 4–5 | 0.18 | 3 | 3–4 | 3 | 2.5–4 | 0.26 |
| Q16 | Do you utilize medical facilities, and school and consultative organizations if required? | 5 | 4–5 | 5 | 4–5 | 0.71 | 4 | 3.5–5 | 4 | 3–4 | 0.26 |
| Q17 | Do you understand your child’s behavior and ideas/feelings/thoughts? | 3 | 3–4 | 4 | 3–4 | 0.32 | 3 | 2.5–4 | 3 | 3–4 | 0.48 |
| Q18 | Do you feel happy being with your child? | 4 | 4–5 | 5 | 3.5–5 | 1 | 5 | 4–5 | 4 | 3.5–4.5 | 0.06 |
| Subject Number | Mothers’ Comments |
|---|---|
| 1 | When I made a feelings sheet, the word “sad” began appearing from my child. It was a good lesson for me as well, and I would like to continue. |
| 2 | Since attending STSSE, my child has been increasingly inviting friends to the house for short visits. I am glad to see that. |
| 3 | My daughter has come to understand the things that cannot be communicated with words only and is more accepting of the things I say. Her sister has reported to me that she was doing her homework without being told. |
| 4 | My daughter has come to be able to control her emotions. She has become able to process things well after her emotions explode. I am enjoying it as well. |
| 5 | I did not know what my daughter was thinking before, so it was good to understand her thoughts in this exercise. I realized that my daughter was also paying attention to me. There are limits to what parents can communicate to children. Neither my spouse nor I have friends, so that’s an issue that needs to be addressed. |
| 6 | My son has become better at how he deals with things after he becomes angry. |
| 7 | It was enjoyable for my son and I. My son now has fewer quarrels with his friends. |
| 8 | My daughter was able to raise her hand and answer at school. Although, it was only two times, it still made me happy. I want to continue practicing so that I can communicate my feelings with words using the basic pattern we learned at STSSE. |
| 9 | Even when trying to ask my son why he thought something, he had built an emotional wall and I could not get in. My son seems to have made a decision to not talk about what happens at school, and will not tell me. I received a call that there might be trouble with the sixth grade students at the school sports festival; my son always wanted to be in the first position. But on the day of the festival, everything was fine. In the running race, even though he was third, he lined up in the third place position smoothly without being told to do so. |
| 10 | I really felt that STSSE was effective for us as parents. I was even asked at my son’s school if I was doing something different. My son does not bite his fingernails as much. A major issue now is emotional control, and we are looking for solutions as a family. We parents learned something too. |
| 11 | I understood that my son needs to grow with praise. I also understood that in an organized environment, he can make friends. He still seems to make decisions with emotions either 0% or 100%, good or bad. |
| 12 | My son has come to understand troubled looks on people’s faces. I hope he will become able to express his emotions in words. We as parents no longer get angry as much. |
| 13 | With his disorder, my son does not understand the difference between himself and others; and I thought that by making a measure (scale) for each emotion and showing him visually, it would be easier for him to understand and to do self-analysis. |
| 14 | When I ask about school or other things that my daughter does not want to talk about, she will tell me and resolve her feelings a little if we move to another place to talk. I have learned the keys to using STSSE. As parents, we have come to give her more steady praise. |
| 15 | My son does not seem to be good at saying things that make others feel good, but he has begun saying things to me such as “this dinner is really good.” |
| 16 | My son said that the STSSE games were fun. Even now he still always wants to be number one. His handwriting is sloppy though because he wants to be the first to turn in his paper; this is something we are working on now. |
| 17 | My son has become a master of the multiplication table and seems to have confidence in himself. Not being understood by others causes stress in him, and I want him to be able to say things. I wish he were able to switch moods when something is bothering him. As a parent, I have become able to listen more to what my son says, and have become able to be a little more reassured. |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okuno, H.; Yamamoto, T.; Tatsumi, A.; Mohri, I.; Taniike, M. Simultaneous Training for Children with Autism Spectrum Disorder and Their Parents with a Focus on Social Skills Enhancement. Int. J. Environ. Res. Public Health 2016, 13, 590. https://doi.org/10.3390/ijerph13060590
Okuno H, Yamamoto T, Tatsumi A, Mohri I, Taniike M. Simultaneous Training for Children with Autism Spectrum Disorder and Their Parents with a Focus on Social Skills Enhancement. International Journal of Environmental Research and Public Health. 2016; 13(6):590. https://doi.org/10.3390/ijerph13060590
Chicago/Turabian StyleOkuno, Hiroko, Tomoka Yamamoto, Aika Tatsumi, Ikuko Mohri, and Masako Taniike. 2016. "Simultaneous Training for Children with Autism Spectrum Disorder and Their Parents with a Focus on Social Skills Enhancement" International Journal of Environmental Research and Public Health 13, no. 6: 590. https://doi.org/10.3390/ijerph13060590
APA StyleOkuno, H., Yamamoto, T., Tatsumi, A., Mohri, I., & Taniike, M. (2016). Simultaneous Training for Children with Autism Spectrum Disorder and Their Parents with a Focus on Social Skills Enhancement. International Journal of Environmental Research and Public Health, 13(6), 590. https://doi.org/10.3390/ijerph13060590