
Evaluation of the Effectiveness of Tai Chi versus Brisk Walking in Reducing Cardiovascular Risk Factors: Protocol for a Randomized Controlled Trial

 ,
, {kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
- (1)
- Have systolic blood pressure (SBP) > 140 mmHg or diastolic blood pressure (DBP) > 90 mmHg or are taking blood pressure medication, and
- (2)
- Meet at least two but not more than three of the following CVD risk factors that are defined according to the American Heart Association [4]:
- (a)
- Males older than 45 years
- (b)
- Females older than 55 years or postmenopausal
- (c)
- Smoker
- (d)
- Fasting cholesterol level > 6.2 mmol/L
- (e)
- Have diabetes or taking medicine to control blood sugar
- (f)
- Physically inactive (get <30 min of physical activity for at least 3 days a week)
- (g)
- Body mass index (BMI) >25 kg/m2 or waist circumference ≥90 cm (men) or ≥80 cm (women)
- (1)
- Have developed cardiovascular disease
- (2)
- Suffered from severe sensory or cognitive impairment
- (3)
- Cannot walk independently
- (4)
- Have musculoskeletal disorders or other disabling diseases that may limit the practice of Tai Chi
- (5)
- Have previous training and practiced Tai Chi within six months prior to the commencement of the study
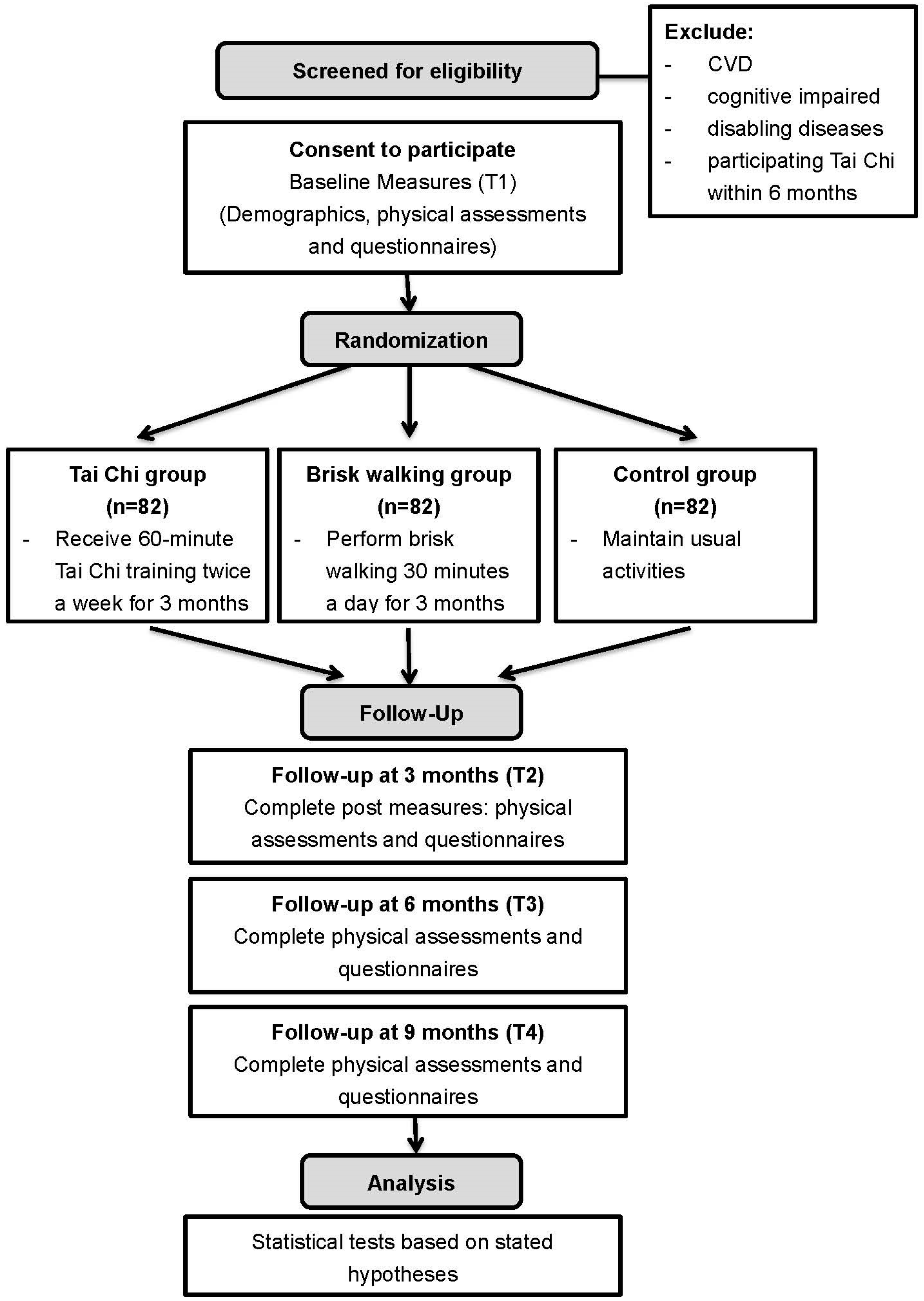
2.2. Study Design
Sample Size and Randomization
2.3. Intervention Protocol
2.3.1. Tai Chi Group
2.3.2. Walking Group
2.3.3. Control Group
2.4. Outcome Measurements
2.4.1. Primary Outcomes
- (a)
- BP: Two measurements of BP will be measured from the seated position after the participant has rested for 10 min. The average of the two values will be used for study purposes. SBP and DBP will be recorded. Only one digital blood pressure monitor will be used for all BP measurements for all participants. Coefficients of variation (CV) of SBP and DBP were reported <10% in a previous study [22]. CV is a unit-less measure that depicts the size of the SD relative to its mean.
2.4.2. Secondary Outcomes
- (a)
- After an 8- to 10-h fasting, blood samples will be taken by using a finger-stick for the following measurements using auto-analyzers:
- (i)
- Fasting blood sugar (FBS)
- (ii)
- Glycated hemoglobin (HbA1c)
- (iii)
- (b)
- BMI will be calculated as weight (kg) divided by the square of height (m). Height and weight (measured to the nearest 0.1 kg) will be measured with the subject wearing light clothing without shoes
- (c)
- Waist circumference will be measured to within 1 mm by using a plastic measuring tape at midway between the lowest rib and the iliac crest with the subject standing at the end of gentle expiration. CV of waist circumference was reported <0.13 in a previous study [29].
- (d)
- Frequency and duration of self-practice of Tai Chi/brisk walking from a self-recorded logbook
- (e)
- Perceived stress scale (PSS-10)
- (f)
- Quality of life: Short-form 12 health survey (SF-12v2)
2.5. Data Collection Procedure
2.6. Data Analysis
- (1)
- For demographic data, frequency and percentage will be used to summarize and present categorical variables, whereas mean and SD will be used for continuous variables. Normality of continuous variables will be examined using skewness and kurtosis statistics and normal probability plot. The baseline characteristics among the three groups will be compared using chi-square test and one-way analysis of variance (ANOVA).
- (2)
- Generalized estimating equations (GEE) models with appropriate link function and distribution assumption, will be used to compare the changes in outcome variables across time among the three groups with adjustment for those baseline characteristics showing statistically significant differences among the groups. In the GEE model for each outcome, two dummy variables will be set to correspond the three groups with the control as reference. Another three dummy variables will be set to represent the four time points (T1 to T4) with the baseline (T1) as the reference. The interaction-terms of group by time will also be included in the GEE models to assess the differential changes of the outcomes across time and between group. All primary and secondary outcomes will be compared between the three groups on the basis of the intention-to-treat (ITT) principle. The GEE model can account for intra-correlated repeated measures data and accommodate missing data caused by dropouts, provided the data is missing at random [34], and thus is particularly suitable for ITT analysis, without the need for imputation of missing data.
2.7. Ethical Considerations
2.8. Dissemination
3. Discussion
Strengths and Limitations of This Study
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Cardiovascular Disease. Updated 2013. Available online: http://www.who.int/cardiovascular_diseases/en/ (accessed on 14 October 2013).
- Centre for Health Protection. Number of Deaths by Leading Causes of Death; Updated 2013. Available online: http://www.chp.gov.hk/en/data/4/10/27/380.html (accessed on 23 September 2013).
- International Diabetes Federation. The IDF Consensus Worldwide Definition of the Metabolic Syndrome. Updated 2006. Available online: http://www.idf.org/webdata/docs/MetS_def_update2006.pdf (accessed on 14 October 2013).
- American Heart Association. Health Heart Screenings. Available online: http://www.heart.org/HEARTORG/Conditions/Heart-Health-Screenings_UCM_428687_Article.jsp (accessed on 14 October 2013).
- Rosengren, A.; Hawken, S.; Ôunpuu, S.; Sliwa, K.; Zubaid, M.; Almahmeed, W.A.; Blackett, K.N.; Sitthiamorn, C.; Sato, H.; Yusuf, S.; et al. Association of psychosocial risk factors with risk of acute myocardial infarction in 11,119 cases and 13,648 controls from 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 953–962. [Google Scholar] [CrossRef]
- Department of Health. Behavioural Risk Factor Survey; Department of Health: Hong Kong, China, 2010. [Google Scholar]
- Roux, L.; Pratt, M.; Tengs, T.O.; Yore, M.M.; Yanagawa, T.L.; Van Den Bos, J.; Rutt, C.; Brownson, R.C.; Powell, K.E.; Heath, G.; et al. Cost effectiveness of community-based physical activity interventions. Am. J. Prev. Med. 2008, 35, 578–588. [Google Scholar] [CrossRef] [PubMed]
- Murtagh, E.M.; Murphy, M.H.; Boone-Heinonen, J. Walking: The first steps in cardiovascular disease prevention. Curr. Opin. Cardiol. 2010, 25, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Donesky-Cuenco, D.; Janson, S.; Neuhaus, J.; Neilands, T.B.; Carrieri-Kohlman, V. Adherence to a home-walking prescription in patients with chronic obstructive pulmonary disease. Heart Lung 2007, 36, 348–363. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.; Lee, A.; Lee, D.T.; Suen, L.K.; Tam, W.W.; Chair, S.Y.; Griffiths, P. The sustaining effects of Tai chi Qigong on physiological health for COPD patients: A randomized controlled trial. Complement. Ther. Med. 2013, 21, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.; Wang, C.; Ho, R.T.; Ziea, E.T.; Wong, V.C.T. Tai Chi exercise for patients with heart disease: A systematic review of controlled clinical trials. Altern. Ther. Health Med. 2012, 18, 16–22. [Google Scholar] [PubMed]
- Zhang, Y.; Fu, F.H. Effects of 14-week Tai Ji Quan exercise on metabolic control in women with type 2 diabetes. Am. J. Chin. Med. 2008, 36, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.L.; O’Grady, M.; Easley, K.A.; Guo, Y.; Kressig, R.W.; Kutner, M. The influence of intense Tai Chi training on physical performance and hemodynamic outcomes in transitionally frail, older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Field, T. Tai Chi research review. Complement. Ther. Clin. Pract. 2011, 17, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Li, J.X.; Hong, Y.; Chan, K.M. Tai Chi: Physiological characteristics and beneficial effects on health. Br. J. Sports Med. 2001, 35, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Piliae, R.E.; Haskell, W.L.; Froelicher, E.S. Hemodynamic responses to a community-based Tai Chi exercise intervention in ethnic Chinese adults with cardiovascular disease risk factors. Eur. J. Cardiovasc. Nurs. 2006, 5, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Pittler, M.H.; Taylor-Piliae, R.E.; Ernst, E. Tai Chi for cardiovascular disease and its risk factors: A systematic review. J. Hypertens. 2007, 25, 1974–1975. [Google Scholar] [CrossRef] [PubMed]
- Yeh, G.Y.; Wang, C.; Wayne, P.M.; Phillips, R. Tai chi exercise for patients with cardiovascular conditions and risk factors: A systematic review. J. Cardiopulm. Rehabil. Prev. 2009, 29, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Hartley, L.; Flowers, N.; Lee, M.S.; Ernst, E.; Rees, K. Tai Chi for primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Audette, J.F.; Jin, Y.S.; Newcomer, R.; Stein, L.; Duncan, G.; Frontera, W.R. Tai Chi versus brisk walking in elderly women. Age Ageing 2006, 35, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Asia Pacific Cohort Studies Collaboration. Systolic blood pressure, diabetes and the risk of cardiovascular diseases in the Asia-Pacific region. J. Hypertens. 2007, 25, 1205–1213. [Google Scholar]
- Tsai, J.; Wang, W.; Chan, P.; Lin, J.L.; Wang, C.H.; Tomlinson, B.; Hsieh, M.H.; Yang, H.Y.; Liu, J.C. The beneficial effects of Tai Chi Chuan on blood pressure and lipid profile and anxiety status in a randomized controlled trial. J. Altern. Complement. Med. 2003, 9, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Roussel, M.; Garnier, S.; Lemoine, S.; Gaubert, I.; Charbonnier, L.; Auneau, G.; Mauriège, P. Influence of a walking program on the metabolic risk profile of obese postmenopausal women. Menopause 2009, 16, 566–575. [Google Scholar] [CrossRef] [PubMed]
- Social Psychology Network. Research Randomizer. Updated 2007. Available online: http://www.randomizer.org (accessed on 14 October 2013).
- Lindemann, U.; Hammer, W.; Muche, R.; Nikolaus, T.; Becker, C. Postural control in the elderly: Effect of a twelve week Tai Chi-Qigong intervention in healthy elderly. Eur. J. Geriatr. 2003, 5, 182–186. [Google Scholar]
- Department of Health. Exercise Prescription Doctor’s Handbook; 2012. Available online: http://exerciserx.cheu.gov.hk/files/DoctorsHanbook_fullversion.pdf (accessed on 14 October 2013).
- United States: Department of Health. Physical Activity and Health: A Report of the Surgeon General; DIANE Publishing: Darby, PA, USA, 1996. [Google Scholar]
- Song, R.; Ahn, S.; Roberts, B.L.; Lee, E.O.; Ahn, Y.H. Adhering to a Tai Chi program to improve glucose control and quality of life for individuals with type 2 diabetes. J. Altern. Complement. Med. 2009, 15, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.N.; Hong, A.W.L.; Tomlinson, B.; Lau, E.; Lam, C.W.K.; Sanderson, J.E.; Woo, J. Effects of Tai Chi and resistance training on cardiovascular risk factors in elderly Chinese subjects: A 12-month longitudinal, randomized, controlled intervention study. Clin. Endocrinol. 2005, 63, 663–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, D.Y.; Lam, T.; Chan, S.S. Three versions of perceived stress scale: Validation in a sample of Chinese cardiac patients who smoke. BMC Public Health 2010, 10, 513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor-Pilae, R.E.; Haskell, W.L.; Waters, C.M.; Froelicher, E.S. Change in perceived psychosocial status following a 12-week Tai Chi exercise programme. J. Adv. Nurs. 2006, 54, 313–329. [Google Scholar] [CrossRef] [PubMed]
- Lam, E.T.; Lam, C.L.; Fong, D.Y.; Huang, W.W. Is the SF-12 version 2 health survey a valid and equivalent substitute for the SF-36 version 2 health survey for the Chinese? J. Eval. Clin. Pract. 2013, 19, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, J.D.; Willett, J.B. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Chen, K.M. Tai Chi. In Complementary/Alternative Therapies in Nursing, 4th ed.; Synder, M., Lindquist, R., Eds.; Springer Publishing Company: New York, NY, USA, 2002; pp. 234–241. [Google Scholar]
- Birdee, G.S.; Wayne, P.M.; Davis, R.B.; Phillips, R.S.; Yeh, G.Y. Tai Chi and Qigong for health: Patterns of use in the United States. J. Altern. Complement. Med. 2009, 15, 969–973. [Google Scholar] [CrossRef] [PubMed]
- Jahnke, R.; Larkey, L.; Rogers, C.; Etnier, J. A comprehensive review of health benefits of Qigong and Tai Chi. Am. J. Health Promot. 2010, 24, e1–e25. [Google Scholar] [CrossRef] [PubMed]
- Klein, P.; Adams, W. Comprehensive therapeutic benefits of Taiji: A critical review. Am. J. Phys. Med. Rehabil. 2004, 83, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Piliae, R. Tai Chi as an adjunct to cardiac rehabilitation exercise training. J. Cardiopulm. Rehabil. 2003, 23, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Motivala, S.S.; Sollers, J.; Thayer, J.; Irwin, M.R. Tai Chi Chih acutely decreases sympathetic nervous system activity in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1177–1180. [Google Scholar] [CrossRef] [PubMed]
- Burini, D.; Farabollini, B.; Iacucci, S.; Rimatori, C.; Riccardi, G.; Capecci, M.; Provinciali, L.; Ceravolo, M.G. A randomized controlled cross-over trial of aerobic training versus Qigong in advanced Parkinson’s disease. Eur. Medicophys. 2006, 42, 231–238. [Google Scholar]
- Song, R.; Lee, E.; Lam, P.; Bae, S. Effects of Tai Chi exercise on pain, balance, muscle strength, and perceived difficulties in physical functioning in older women with osteoarthritis: A randomized clinical trial. J. Rheumatol. 2003, 30, 2039–2044. [Google Scholar] [PubMed]
- Mustian, K.M.; Katula, J.A.; Zhao, H. A pilot study to assess the influence of Tai Chi Chuan on functional capacity among breast cancer survivors. J. Support Oncol. 2006, 4, 139–145. [Google Scholar] [PubMed]

© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, A.W.K.; Sit, J.W.H.; Chair, S.Y.; Leung, D.Y.P.; Lee, D.T.F.; Wong, E.M.L.; Fung, L.C.W. Evaluation of the Effectiveness of Tai Chi versus Brisk Walking in Reducing Cardiovascular Risk Factors: Protocol for a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2016, 13, 682. https://doi.org/10.3390/ijerph13070682
Chan AWK, Sit JWH, Chair SY, Leung DYP, Lee DTF, Wong EML, Fung LCW. Evaluation of the Effectiveness of Tai Chi versus Brisk Walking in Reducing Cardiovascular Risk Factors: Protocol for a Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2016; 13(7):682. https://doi.org/10.3390/ijerph13070682
Chicago/Turabian StyleChan, Aileen W. K., Janet W. H. Sit, Sek Ying Chair, Doris Y. P. Leung, Diana T. F. Lee, Eliza M. L. Wong, and Lawrence C. W. Fung. 2016. "Evaluation of the Effectiveness of Tai Chi versus Brisk Walking in Reducing Cardiovascular Risk Factors: Protocol for a Randomized Controlled Trial" International Journal of Environmental Research and Public Health 13, no. 7: 682. https://doi.org/10.3390/ijerph13070682
APA StyleChan, A. W. K., Sit, J. W. H., Chair, S. Y., Leung, D. Y. P., Lee, D. T. F., Wong, E. M. L., & Fung, L. C. W. (2016). Evaluation of the Effectiveness of Tai Chi versus Brisk Walking in Reducing Cardiovascular Risk Factors: Protocol for a Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 13(7), 682. https://doi.org/10.3390/ijerph13070682