
Prediction of Massive Transfusion in Trauma Patients with Shock Index, Modified Shock Index, and Age Shock Index


 ,
,  and
and
Abstract
:1. Background
2. Methods
2.1. Ethics Statement
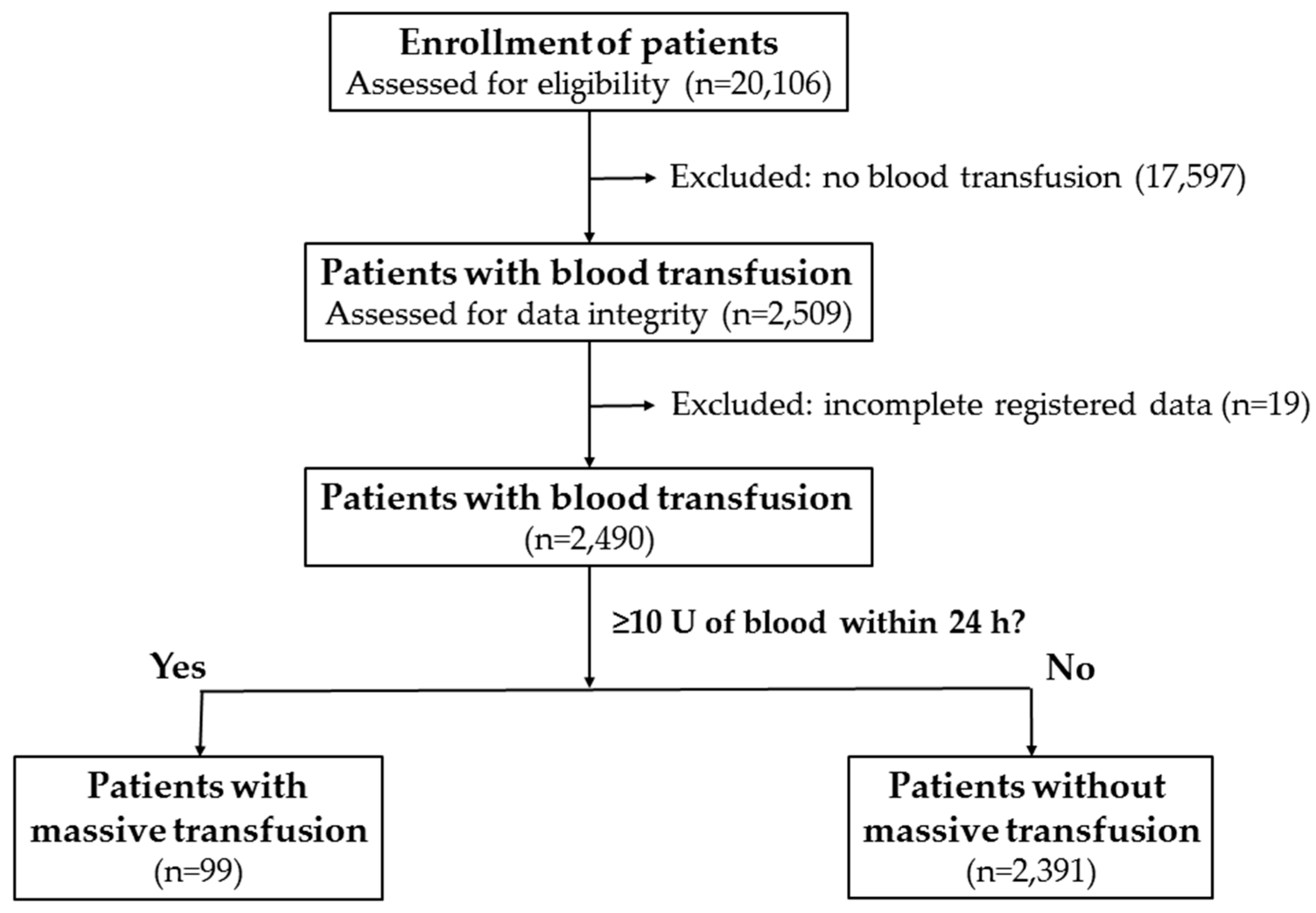
2.2. Study Design
3. Results
3.1. Demographics and Injury Characteristics of Patients Receiving MT
3.2. Injury Severity and Outcome of Patients Receiving MT
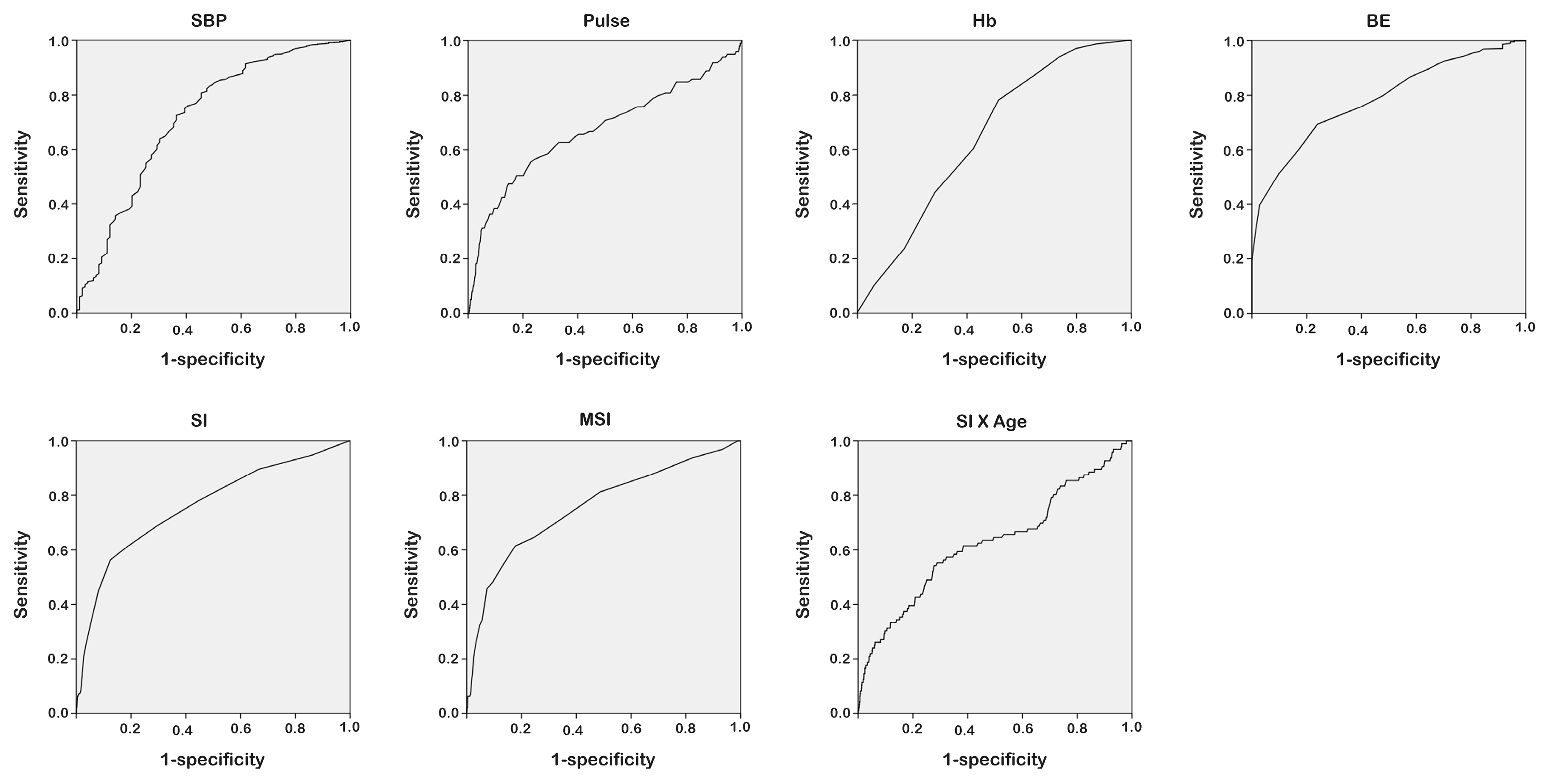
3.3. Association of Physiological Response and Parameters with MT
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Callcut, R.A.; Cotton, B.A.; Muskat, P.; Fox, E.E.; Wade, C.E.; Holcomb, J.B.; Schreiber, M.A.; Rahbar, M.H.; Cohen, M.J.; Knudson, M.M.; et al. Defining when to initiate massive transfusion: A validation study of individual massive transfusion triggers in PROMMTT patients. J. Trauma Acute Care Surg. 2013, 74, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Brockamp, T.; Nienaber, U.; Mutschler, M.; Wafaisade, A.; Peiniger, S.; Lefering, R.; Bouillon, B.; Maegele, M. Predicting on-going hemorrhage and transfusion requirement after severe trauma: A validation of six scoring systems and algorithms on the TraumaRegister DGU. Crit. Care 2012, 16, R129. [Google Scholar] [CrossRef] [PubMed]
- Moffat, B.; Vogt, K.N.; Inaba, K. The Shock Index: Is it ready for primetime? Crit. Care 2013, 17, 196. [Google Scholar] [CrossRef] [PubMed]
- Holcomb, J.B.; del Junco, D.J.; Fox, E.E.; Wade, C.E.; Cohen, M.J.; Schreiber, M.A.; Alarcon, L.H.; Bai, Y.; Brasel, K.J.; Bulger, E.M.; et al. The prospective, observational, multicenter, major trauma transfusion (PROMMTT) study: Comparative effectiveness of a time-varying treatment with competing risks. JAMA Surg. 2013, 148, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Mitra, B.; Mori, A.; Cameron, P.A.; Fitzgerald, M.; Street, A.; Bailey, M. Massive blood transfusion and trauma resuscitation. Injury 2007, 38, 1023–1029. [Google Scholar] [CrossRef] [PubMed]
- Malone, D.L.; Hess, J.R.; Fingerhut, A. Massive transfusion practices around the globe and a suggestion for a common massive transfusion protocol. J. Trauma 2006, 60, S91–S96. [Google Scholar] [CrossRef] [PubMed]
- Schuster, K.M.; Davis, K.A.; Lui, F.Y.; Maerz, L.L.; Kaplan, L.J. The status of massive transfusion protocols in United States trauma centers: Massive transfusion or massive confusion? Transfusion 2010, 50, 1545–1551. [Google Scholar] [CrossRef] [PubMed]
- Olaussen, A.; Blackburn, T.; Mitra, B.; Fitzgerald, M. Review article: Shock index for prediction of critical bleeding post-trauma: A systematic review. Emerg. Med. Aust. 2014, 26, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Olaussen, A.T.P.; Fitzgerald, M.C.; Jennings, P.A.; Hocking, J.; Mitra, B. Prediction of critical haemorrhage following trauma: A narrative review. J. Emerg. Med. Trauma Acute Care 2016, 1, 3. [Google Scholar] [CrossRef]
- Allgower, M.; Burri, C. Shock index. Dtsch. Med. Wochenschr. 1967, 92, 1947–1950. [Google Scholar] [PubMed]
- Birkhahn, R.H.; Gaeta, T.J.; Terry, D.; Bove, J.J.; Tloczkowski, J. Shock index in diagnosing early acute hypovolemia. Am. J. Emerg. Med. 2005, 23, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Vandromme, M.J.; Griffin, R.L.; Kerby, J.D.; McGwin, G., Jr.; Rue, L.W., 3rd; Weinberg, J.A. Identifying risk for massive transfusion in the relatively normotensive patient: Utility of the prehospital shock index. J. Trauma 2011, 70, 384–390. [Google Scholar] [PubMed]
- Mitra, B.; Fitzgerald, M.; Chan, J. The utility of a shock index >/= 1 as an indication for pre-hospital oxygen carrier administration in major trauma. Injury 2014, 45, 61–65. [Google Scholar] [CrossRef] [PubMed]
- McNab, A.; Burns, B.; Bhullar, I.; Chesire, D.; Kerwin, A. An analysis of shock index as a correlate for outcomes in trauma by age group. Surgery 2013, 154, 384–387. [Google Scholar] [CrossRef] [PubMed]
- DeMuro, J.P.; Simmons, S.; Jax, J.; Gianelli, S.M. Application of the shock index to the prediction of need for hemostasis intervention. Am. J. Emerg. Med. 2013, 31, 1260–1263. [Google Scholar] [CrossRef] [PubMed]
- Mutschler, M.; Nienaber, U.; Munzberg, M.; Wolfl, C.; Schoechl, H.; Paffrath, T.; Bouillon, B.; Maegele, M. The shock index revisited—A fast guide to transfusion requirement? A retrospective analysis on 21,853 patients derived from the TraumaRegister DGU. Crit. Care 2013, 17, R172. [Google Scholar] [PubMed]
- Sisak, K.; Manolis, M.; Hardy, B.M.; Enninghorst, N.; Bendinelli, C.; Balogh, Z.J. Acute transfusion practice during trauma resuscitation: Who, when, where and why? Injury 2013, 44, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.C.; Liu, J.H.; Fang, Z.A.; Shan, G.L.; Xu, J.; Qi, Z.W.; Zhu, H.D.; Wang, Z.; Yu, X.Z. Modified shock index and mortality rate of emergency patients. World J. Emerg. Med. 2012, 3, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Ali, S.; Agarwal, A.; Srivastava, R.N. Correlation of shock index and modified shock index with the outcome of adult trauma patients: A prospective study of 9860 patients. N. Am. J. Med. Sci. 2014, 6, 450–452. [Google Scholar] [CrossRef] [PubMed]
- Zarzaur, B.L.; Croce, M.A.; Fischer, P.E.; Magnotti, L.J.; Fabian, T.C. New vitals after injury: Shock index for the young and age × shock index for the old. J. Surg. Res. 2008, 147, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Acker, S.N.; Ross, J.T.; Partrick, D.A.; Tong, S.; Bensard, D.D. Pediatric specific shock index accurately identifies severely injured children. J. Pediatr. Surg. 2015, 50, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Paladino, L.; Subramanian, R.A.; Nabors, S.; Sinert, R. The utility of shock index in differentiating major from minor injury. Eur. J. Emerg. Med. 2011, 18, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Torabi, M.; Mirafzal, A.; Rastegari, A.; Sadeghkhani, N. Association of triage time shock index, modified shock index, and age shock index with mortality in emergency severity index level 2 patients. Am. J. Emerg. Med. 2016, 34, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Physical Status: The Use and Interpretation of Anthropometry; WHO: Geneva, Switzerland, 1995; Volume 854, pp. 1–452.
- Obesity: Preventing and Managing the Global Epidemic; WHO: Geneva, Switzerland, 2000; Volume 894, i–xii, pp. 1–253.
- Akobeng, A.K. Understanding diagnostic tests 3: Receiver operating characteristic curves. Acta Paediatr. 2007, 96, 644–647. [Google Scholar] [CrossRef] [PubMed]
- Sohn, C.H.; Kim, W.Y.; Kim, S.R.; Seo, D.W.; Ryoo, S.M.; Lee, Y.S.; Lee, J.H.; Oh, B.J.; Won, H.S.; Shim, J.Y.; et al. An increase in initial shock index is associated with the requirement for massive transfusion in emergency department patients with primary postpartum hemorrhage. Shock 2013, 40, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.; Eo, E.; Ahn, K.; Noh, H.; Cheon, Y. Initial base deficit as predictors for mortality and transfusion requirement in the severe pediatric trauma except brain injury. Pediatr. Emerg. Care 2009, 25, 579–581. [Google Scholar] [CrossRef] [PubMed]
- Mutschler, M.; Nienaber, U.; Brockamp, T.; Wafaisade, A.; Fabian, T.; Paffrath, T.; Bouillon, B.; Maegele, M. Renaissance of base deficit for the initial assessment of trauma patients: A base deficit-based classification for hypovolemic shock developed on data from 16,305 patients derived from the TraumaRegister DGU(R). Crit. Care 2013, 17, R42. [Google Scholar] [CrossRef] [PubMed]
- Hess, J.R.; Hiippala, S. Optimizing the use of blood products in trauma care. Crit. Care 2005, S10–S14. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, S.; Demirci, O.; Arteaga, G.; Kashyap, R.; Smischney, N.J. Evaluation of preintubation shock index and modified shock index as predictors of postintubation hypotension and other short-term outcomes. J. Crit. Care 2015, 30. [Google Scholar] [CrossRef] [PubMed]
- Chuang, J.F.; Rau, C.S.; Wu, S.C.; Liu, H.T.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C.; Hsieh, C.H. Use of the reverse shock index for identifying high-risk patients in a five-level triage system. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 12. [Google Scholar] [CrossRef] [PubMed]
- Lai, W.H.; Rau, C.S.; Hsu, S.Y.; Wu, S.C.; Kuo, P.J.; Hsieh, H.Y.; Chen, Y.C.; Hsieh, C.H. Using the reverse shock index at the injury scene and in the emergency department to identify high-risk patients: A cross-sectional retrospective study. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Lai, W.H.; Wu, S.C.; Rau, C.S.; Kuo, P.J.; Hsu, S.Y.; Chen, Y.C.; Hsieh, H.Y.; Hsieh, C.H. Systolic blood pressure lower than heart rate upon arrival at and departure from the emergency department indicates a poor outcome for adult trauma patients. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Reisner, A.T.; Gribok, A.; Reifman, J. Exploration of prehospital vital sign trends for the prediction of trauma outcomes. Prehosp. Emerg. Care 2009, 13, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Olaussen, A.; Peterson, E.L.; Mitra, B.; O’Reilly, G.; Jennings, P.A.; Fitzgerald, M. Massive transfusion prediction with inclusion of the pre-hospital shock index. Injury 2015, 46, 822–826. [Google Scholar] [CrossRef] [PubMed]
- Ogura, T.; Nakamura, Y.; Nakano, M.; Izawa, Y.; Nakamura, M.; Fujizuka, K.; Suzukawa, M.; Lefor, A.T. Predicting the need for massive transfusion in trauma patients: The Traumatic Bleeding Severity Score. J. Trauma Acute Care Surg. 2014, 76, 1243–1250s. [Google Scholar] [CrossRef] [PubMed]
- Ogura, T.; Nakano, M.; Izawa, Y.; Nakamura, M.; Fujizuka, K.; Lefor, A.T. Analysis of risk classification for massive transfusion in severe trauma using the gray zone approach. Am. J. Emerg. Med. 2015, 33, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- Yucel, N.; Lefering, R.; Maegele, M.; Vorweg, M.; Tjardes, T.; Ruchholtz, S.; Neugebauer, E.A.; Wappler, F.; Bouillon, B.; Rixen, D. Trauma Associated Severe Hemorrhage (TASH)-Score: Probability of mass transfusion as surrogate for life threatening hemorrhage after multiple trauma. J. Trauma 2006, 60, 1228–1237. [Google Scholar] [CrossRef] [PubMed]
- Mitra, B.; Olaussen, A.; Cameron, P.A.; O’Donohoe, T.; Fitzgerald, M. Massive blood transfusions post trauma in the elderly compared to younger patients. Injury 2014, 45, 1296–1300. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | MT n = 99 | No MT n = 2391 | Odds Ratio (95% CI) | p | |||
|---|---|---|---|---|---|---|---|
| Age | 42.6 | ±18.5 | 49.4 | ±19.4 | - | 0.001 | |
| Sex | |||||||
| Male | 78 | (78.8) | 1530 | (64.0) | 2.1 | (1.28–3.41) | 0.003 |
| Female | 21 | (21.2) | 861 | (36.0) | 0.5 | (0.29–0.78) | 0.003 |
| BMI | |||||||
| BMI < 18.5 | 5 | (5.1) | 196 | (8.2) | 0.6 | (0.24–1.48) | 0.346 |
| 18.5 ≤ BMI < 25 | 41 | (41.4) | 1206 | (50.4) | 0.7 | (0.46–1.04) | 0.082 |
| 25 ≤ BMI < 30 | 30 | (30.3) | 636 | (26.6) | 1.2 | (0.77–1.86) | 0.418 |
| BMI ≥ 30 | 9 | (9.1) | 180 | (7.5) | 1.2 | (0.61–2.48) | 0.699 |
| Co-morbidity | |||||||
| HTN | 7 | (7.1) | 557 | (23.3) | 0.3 | (0.12–0.54) | p < 0.001 |
| DM | 6 | (6.1) | 298 | (12.5) | 0.5 | (0.20–1.04) | 0.059 |
| CAD | 1 | (1.0) | 58 | (2.4) | 0.4 | (0.06–2.99) | 0.516 |
| CHF | 0 | (0.0) | 11 | (0.5) | - | 1.000 | |
| ESRD | 0 | (0.0) | 18 | (0.8) | - | 0.639 | |
| Alcohol ≥ 50 | 14 | (14.1) | 226 | (9.5) | 1.6 | (0.88–2.82) | 0.161 |
| ISS (median, IQR) | 26 | (18–38) | 13 | (9–20) | - | p < 0.001 | |
| <16 | 15 | (15.2) | 1483 | (62.0) | 0.1 | (0.06–0.19) | p < 0.001 |
| 16–24 | 26 | (26.3) | 505 | (21.1) | 1.3 | (0.84–2.10) | 0.259 |
| ≥25 | 58 | (58.6) | 403 | (16.9) | 7.0 | (4.61–10.56) | p < 0.001 |
| Mortality (crude) | 30 | (30.3) | 64 | (2.7) | 15.8 | (9.63–25.94) | p < 0.001 |
| Mortality (adjusted) | - | - | 5.4 | (2.91–9.84) | p < 0.001 | ||
| Hospital LOS (days) | 21.6 | ±19.2 | 12.8 | ±12.2 | - | p < 0.001 | |
| ICU (n, %) | 84 | (84.8) | 872 | (36.5) | 9.8 | (5.60–17.00) | p < 0.001 |
| ICU LOS (days) | 9.7 | ±9.8 | 7.3 | ±8.2 | - | 0.035 | |
| Variables | MT | No MT | p | ||
|---|---|---|---|---|---|
| HR (beats/min) | 104.8 | ±29.8 | 89.3 | ±20.7 | p < 0.001 |
| SBP (mmHg) | 110.7 | ±41.4 | 139.9 | ±34.8 | p < 0.001 |
| Hb (g/dL) | 11.4 | ±3.0 | 13.0 | ±2.1 | p < 0.001 |
| BD (mmol/L) | −8.8 | ±6.3 | −3.3 | ±5.2 | p < 0.001 |
| SI (bpm/mmHg) | 1.1 | ±0.5 | 0.7 | ±0.3 | p < 0.001 |
| MSI (bpm/mmHg) | 1.4 | ±0.8 | 0.9 | ±0.4 | p < 0.001 |
| Age SI (years × bpm/mmHg) | 43.1 | ±26.3 | 31.7 | ±15.2 | p < 0.001 |
| Variables | Cut-off | Sensitivity | Specificity | AUC |
|---|---|---|---|---|
| HR (beats/min) | 109.50 | 0.475 | 0.853 | 0.671 |
| SBP (mmHg) | 120.5 | 0.725 | 0.636 | 0.716 |
| Hb (g/dl) | 11.50 | 0.782 | 0.485 | 0.645 |
| BD (mmol/L) | −4.50 | 0.693 | 0.761 | 0.784 |
| SI (bpm/mmHg) | 0.950 | 0.563 | 0.876 | 0.760 |
| MSI (bpm/mmHg) | 1.150 | 0.615 | 0.823 | 0.756 |
| Age SI (years × bpm/mmHg) | 36.95 | 0.542 | 0.723 | 0.627 |
| Variables | SI | MSI | Age SI | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cut-off | Sensitivity | Specificity | AUC | p | Cut-off | Sensitivity | Specificity | AUC | p | Cut-Off | Sensitivity | Specificity | AUC | p | |
| Male | 0.950 | 0.584 | 0.862 | 0.757 | p < 0.001 | 1.150 | 0.636 | 0.805 | 0.761 | p < 0.001 | 22.550 | 0.844 | 0.283 | 0.626 | p < 0.001 |
| Female | 0.750 | 0.632 | 0.745 | 0.753 | p < 0.001 | 1.150 | 0.526 | 0.853 | 0.719 | 0.001 | 41.550 | 0.526 | 0.830 | 0.651 | 0.024 |
| HTN (+) | 0.750 | 0.500 | 0.874 | 0.672 | 0.148 | 0.750 | 0.833 | 0.504 | 0.653 | 0.198 | 40.250 | 0.667 | 0.699 | 0.588 | 0.458 |
| HTN (−) | 0.950 | 0.589 | 0.852 | 0.749 | p < 0.001 | 1.150 | 0.644 | 0.789 | 0.748 | p < 0.001 | 36.550 | 0.544 | 0.749 | 0.652 | p < 0.001 |
| DM (+) | 0.750 | 0.667 | 0.859 | 0.708 | 0.081 | 0.950 | 0.667 | 0.785 | 0.710 | 0.078 | 34.350 | 0.833 | 0.495 | 0.636 | 0.256 |
| DM (−) | 0.950 | 0.578 | 0.866 | 0.759 | p < 0.001 | 1.150 | 0.622 | 0.810 | 0.756 | p < 0.001 | 36.550 | 0.556 | 0.732 | 0.633 | p < 0.001 |
| CAD (+) | 0.950 | 0.500 | 0.927 | 0.661 | 0.435 | 0.750 | 1.000 | 0.464 | 0.723 | 0.282 | 40.250 | 1.000 | 0.609 | 0.773 | 0.187 |
| CAD (−) | 0.950 | 0.564 | 0.873 | 0.762 | p < 0.001 | 1.150 | 0.617 | 0.819 | 0.757 | p < 0.001 | 36.950 | 0.532 | 0.733 | 0.628 | p < 0.001 |
| Alcohol (+) | 1.050 | 0.643 | 0.815 | 0.780 | p < 0.001 | 1.050 | 0.929 | 0.473 | 0.750 | 0.002 | 55.050 | 0.571 | 0.869 | 0.680 | 0.024 |
| Alcohol (−) | 0.950 | 0.549 | 0.894 | 0.753 | p < 0.001 | 1.150 | 0.585 | 0.847 | 0.752 | p < 0.001 | 36.550 | 0.524 | 0.722 | 0.616 | p < 0.001 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rau, C.-S.; Wu, S.-C.; Kuo, S.C.H.; Pao-Jen, K.; Shiun-Yuan, H.; Chen, Y.-C.; Hsieh, H.-Y.; Hsieh, C.-H.; Liu, H.-T. Prediction of Massive Transfusion in Trauma Patients with Shock Index, Modified Shock Index, and Age Shock Index. Int. J. Environ. Res. Public Health 2016, 13, 683. https://doi.org/10.3390/ijerph13070683
Rau C-S, Wu S-C, Kuo SCH, Pao-Jen K, Shiun-Yuan H, Chen Y-C, Hsieh H-Y, Hsieh C-H, Liu H-T. Prediction of Massive Transfusion in Trauma Patients with Shock Index, Modified Shock Index, and Age Shock Index. International Journal of Environmental Research and Public Health. 2016; 13(7):683. https://doi.org/10.3390/ijerph13070683
Chicago/Turabian StyleRau, Cheng-Shyuan, Shao-Chun Wu, Spencer C. H. Kuo, Kuo Pao-Jen, Hsu Shiun-Yuan, Yi-Chun Chen, Hsiao-Yun Hsieh, Ching-Hua Hsieh, and Hang-Tsung Liu. 2016. "Prediction of Massive Transfusion in Trauma Patients with Shock Index, Modified Shock Index, and Age Shock Index" International Journal of Environmental Research and Public Health 13, no. 7: 683. https://doi.org/10.3390/ijerph13070683
APA StyleRau, C. -S., Wu, S. -C., Kuo, S. C. H., Pao-Jen, K., Shiun-Yuan, H., Chen, Y. -C., Hsieh, H. -Y., Hsieh, C. -H., & Liu, H. -T. (2016). Prediction of Massive Transfusion in Trauma Patients with Shock Index, Modified Shock Index, and Age Shock Index. International Journal of Environmental Research and Public Health, 13(7), 683. https://doi.org/10.3390/ijerph13070683