
Health-Related Quality of Life and Function after Paediatric Injuries in India: A Longitudinal Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
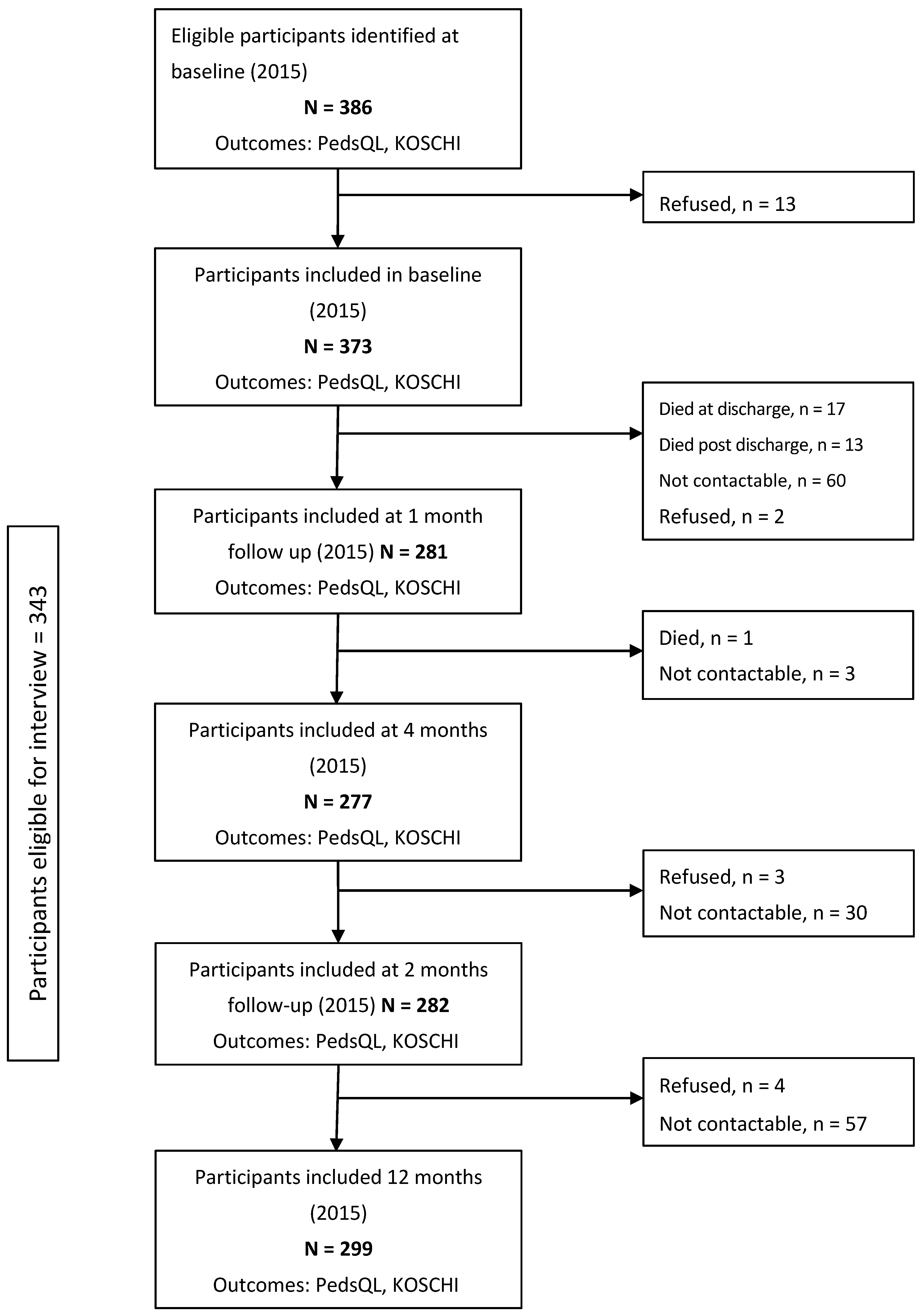
2.2. Study Participants and Eligibility Criteria
2.3. Recruitment Procedures and Follow-Up
2.4. Measures
2.5. The King’s Outcome Scale for Childhood Head Injury
2.6. The Paediatric Quality of Life Inventory
2.7. Statistical Analysis
3. Results
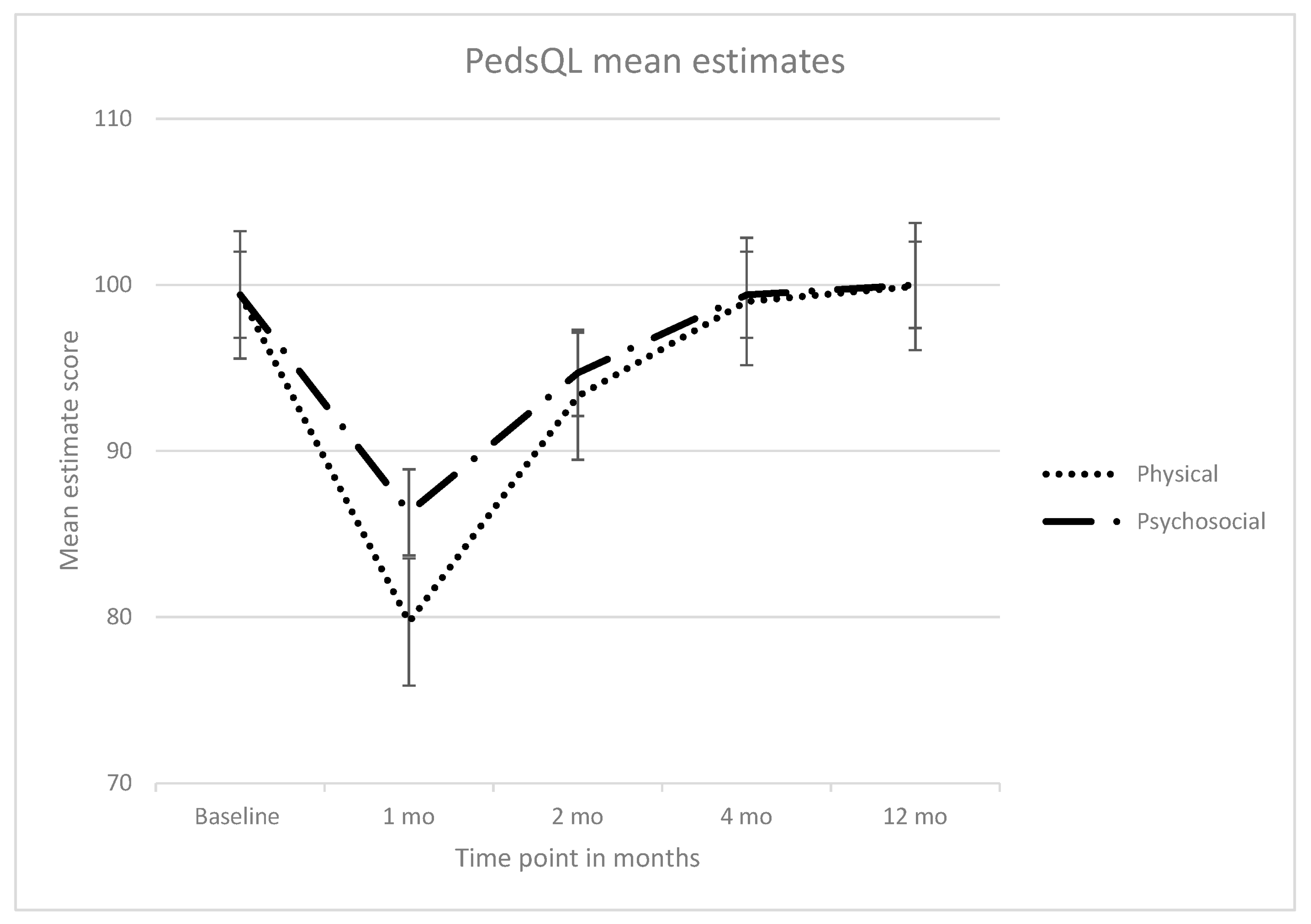
Functional and Health-Related Quality of Life Outcomes
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organisation. World Report on Child Injury Prevention; World Health Organisation: Geneva, Switzerland, 2008. [Google Scholar]
- Mokdad, A.H.; Forouzanfar, M.H.; Daoud, F.; Mokdad, A.A.; El Bcheraoui, C.; Moradi-Lakeh, M.; Kyu, H.H.; Barber, R.M.; Wagner, J.; Cercy, K.; et al. Global burden of diseases, injuries, and risk factors for young people’s health during 1990–2013: A systematic analysis for the global burden of disease study 2013. Lancet 2016, 387, 2383–2401. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-adjusted life years (dalys) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the global burden of disease study 2010. Lancet 2012, 380, 2197–2223. [Google Scholar] [CrossRef]
- Gore, F.M.; Bloem, P.J.N.; Patton, G.C.; Ferguson, J.; Joseph, V.; Coffey, C.; Sawyer, S.M.; Mathers, C.D. Global burden of disease in young people aged 10–24 years: A systematic analysis. Lancet 2011, 377, 2093–2102. [Google Scholar] [CrossRef]
- Mohan, D.; Kumar, A.; Varghese, M. Childhood injuries in rural north india. Int. J. Inj. Control Saf. Promot. 2010, 17, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Jagnoor, J.; Keay, L.; Ganguli, A.; Dandona, R.; Thakur, J.S.; Boufous, S.; Cumming, R.; Ivers, R.Q. Fall related injuries: A retrospective medical review study in north india. Injury 2012, 43, 1996–2000. [Google Scholar] [CrossRef] [PubMed]
- Rivara, F.P.; Oldham, K.T. Pediatric trauma care: Defining a research agenda. J. Trauma Acute Care Surg. 2007, 63, S52–S53. [Google Scholar] [CrossRef] [PubMed]
- Willis, C.D.; Gabbe, B.J.; Butt, W.; Cameron, P.A. Assessing outcomes in paediatric trauma populations. Injury 2006, 37, 1185–1196. [Google Scholar] [CrossRef] [PubMed]
- Jagnoor, J.; Prinja, S.; Lakshmi, P.; Aggarwal, S.; Gabbe, B.; Ivers, R.Q. The impact of road traffic injury in north india: A mixed-methods study protocol. BMJ Open 2015, 5, e008884. [Google Scholar] [CrossRef] [PubMed]
- McCaffrey, N.; Gill, L.; Kaambwa, B.; Cameron, I.D.; Patterson, J.; Crotty, M.; Ratcliffe, J. Important features of home-based support services for older australians and their informal carers. Health Soc. Care Commun. 2015, 23, 654–664. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation (WHO). International Statistical Classification of Disease and Health Related Problems 10th Revision (icd-10) for 2016; World Health Organisation: Genva, Switzerland, 2016. [Google Scholar]
- World Health Organization. The Icd-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- Crouchman, M.; Rossiter, L.; Colaco, T.; Forsyth, R. A practical outcome scale for paediatric head injury. Arch. Dis. Child. 2001, 84, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Janssens, L.; Gorter, J.W.; Ketelaar, M.; Kramer, W.L.; Holtslag, H.R. Health-related quality-of-life measures for long-term follow-up in children after major trauma. Qual. Life Res. 2008, 17, 701–713. [Google Scholar] [CrossRef] [PubMed]
- Gabbe, B.J.; Simpson, P.M.; Sutherland, A.M.; Palmer, C.S.; Williamson, O.D.; Butt, W.; Bevan, C.; Cameron, P.A. Functional and health-related quality of life outcomes after pediatric trauma. J. Trauma Acute Care Surg. 2011, 70, 1532–1538. [Google Scholar] [CrossRef] [PubMed]
- Pedsql 4.0 Tranlsations. Available online: http://www.pedsql.org/PedsQL-Translation-Tables.pdf (accessed on 29 August 2017).
- Jagnoor, J.; Bassani, D.G.; Keay, L.; Ivers, R.Q.; Thakur, J.; Gururaj, G.; Jha, P.; Collaborators, M.D.S. Unintentional injury deaths among children younger than 5 years of age in india: A nationally representative study. Inj. Prev. 2011. [Google Scholar] [CrossRef] [PubMed]
- Winthrop, A.L.; Brasel, K.J.; Stahovic, L.; Paulson, J.; Schneeberger, B.; Kuhn, E.M. Quality of life and functional outcome after pediatric trauma. J. Trauma Acute Care Surg. 2005, 58, 468–474. [Google Scholar] [CrossRef]
- Schneeberg, A.; Ishikawa, T.; Kruse, S.; Zallen, E.; Mitton, C.; Bettinger, J.A.; Brussoni, M. A longitudinal study on quality of life after injury in children. Health Qual. Life Outcomes 2016, 14, 120. [Google Scholar] [CrossRef] [PubMed]
- Awasthi, S.; Agnihotri, K.; Chandra, H.; Singh, U.; Thakur, S. Assessment of health-related quality of life in school-going adolescents: Validation of pedsql instrument and comparison with whoqol-bref. IMSEAR 2012, 25, 74–79. [Google Scholar] [PubMed]
- Pieper, P.; Bear, M. Child and proxy perspectives of the child’s health-related quality of life 1 month after a mild traumatic brain injury. J. Trauma Nurs. 2011, 18, 11–17. [Google Scholar] [CrossRef]
- Varni, J.W.; Limbers, C.A.; Burwinkle, T.M. Impaired health-related quality of life in children and adolescents with chronic conditions: A comparative analysis of 10 disease clusters and 33 disease categories/severities utilizing the pedsqlTM 4.0 generic core scales. Health Qual. Life Outcomes 2007, 5, 43. [Google Scholar] [CrossRef] [PubMed]
- Parmeswaran, G.G.; Kalaivani, M.; Gupta, S.K.; Goswami, A.K.; Nongkynrih, B. Unintentional childhood injuries in urban delhi: A community-based study. Ind. J. Commun. Med. 2017, 42, 8–12. [Google Scholar]
- Harvey, A.; Towner, E.; Peden, M.; Soori, H.; Bartolomeos, K. Injury prevention and the attainment of child and adolescent health. Bull. World Health Organ. 2009, 87, 390–394. [Google Scholar] [CrossRef] [PubMed]
- Jagnoor, J.; Suraweera, W.; Keay, L.; Ivers, R.Q.; Thakur, J.; Gururaj, G.; Jha, P. Childhood and adult mortality from unintentional falls in india. Bull. World Health Organ. 2011, 89, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, C.N.; Lindaman, F.C. Children can’t fly: A program to prevent childhood morbidity and mortality from window falls. Am. J. Public Health 1977, 67, 1143–1147. [Google Scholar] [CrossRef] [PubMed]
- Mathangi Ramakrishnan, K.; Jayaraman, V.; Andal, A.; Shanker, J.; Ramachandran, P. Paediatric rehabilitation in a developing country—India in relation to aetiology, consequences and outcome in a group of 459 burnt children. Pediatr. Rehabil. 2004, 7, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Dalal, A.K. Social interventions to moderate discriminatory attitudes: The case of the physically challenged in India. Psychol. Health Med. 2006, 11, 374–382. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation; The World Bank. World Report on Disabiltiy; The World Health Organisation: Geneva, Switzerland, 2011. [Google Scholar]



{kind=link}
{kind=link}
| Characteristic | n (%) |
|---|---|
| Age group | |
| 2–4 years | 105 (27.2) |
| 5–7 years | 82 (21.2) |
| 8–12 years | 103 (26.7) |
| 13–16 years | 96 (24.9) |
| Gender | |
| Male | 276 (71.5) |
| Female | 110 (28.5) |
| Education (n = 247) ^ | |
| Not at school | 53 (21.5) |
| Primary | 108 (43.7) |
| Middle–Secondary | 78 (34.8) |
| Any comorbidities | |
| Yes | 6 (1.5) |
| No | 380 (98.5) |
| Injury intent | |
| Unintentional | 377 (97.7) |
| Intentional self-harm | 1 (0.3) |
| Assault | 8 (2.1) |
| Place of injury | |
| Home/residential institution | 214 (55.4) |
| Street/highway | 128 (33.2) |
| Other | 44 (11.4) |
| Activity at time of injury | |
| Domestic work/personal hygiene/vital activities | 302 (78.2) |
| Paid work | 15 (3.9) |
| Other | 69 (17.9) |
| Mechanism of injury | |
| Road traffic injury | 138 (35.8) |
| Falls | 187 (48.5) |
| Burn | 22 (5.7) |
| Drowning | - |
| Poisoning | 2 (0.5) |
| Mechanical | 24 (6.2) |
| Others | 13 (3.4) |
| * Severity | |
| Mild (LOS 0–1 day) | 111 (30.1) |
| Moderate (LOS 2–7 days) | 199 (53.9) |
| Severe (LOS 8+ days) | 59 (16.0) |
| Surgery | |
| Surgery performed | 7 (1.8) |
| No surgery | 379 (98.2) |
| Cases referred | |
| Yes | 296 (77.0%) |
| No | 90 (23.0%) |
| Disposition at discharge | |
| Admitted | 354 (91.7%) |
| Left against medical advice | 1 (0.3%) |
| Died | 15 (3.9%) |
| Unknown | 16 (4.1%) |
| Characteristic | n (%) |
|---|---|
| Mode of transportation | |
| Pedestrian | 46 (33.3) |
| Bicycle | 23 (16.7) |
| Two-wheeler | 46 (33.3) |
| Car | 7 (5.1) |
| Bus/truck | 7 (5.1) |
| Other | 8 (5.8) |
| Unknown | 1(0.7) |
| Type of road | |
| Lane | 5 (3.6) |
| Street | 35 (25.3) |
| Main road | 94 (68.1) |
| Unknown/others | 4 (2.9) |
| Role of the injured | |
| Driver/operator | 43 (31.2) |
| Passenger | 65 (47.1) |
| Other | 29 (21.0) |
| Unknown | 1 (0.7) |
| Use of helmet if on two-wheeler (n = 46) | |
| Yes | 5 (10.9) |
| No | 40 (87.0) |
| Missing | 1 (2.2) |
| Use of seatbelt if in car (n = 7) | |
| No | 7 (1.8) |
| Person/object hit in the crash | |
| Vehicle | 97 (70.3) |
| Road surface (pothole) | 19 (13.8) |
| Other | 22 (15.9) |
| Characteristics of Fall Injuries | n (%) |
|---|---|
| Type of fall | |
| Fall from Height | |
| Electric Pole | 8 (4.3) |
| Stairs/steps/ladder | 28 (15.0) |
| Roof/building structure | 69 (36.9) |
| Tree | 15 (8.0) |
| Others | 9 (4.8) |
| Fall from bed/chair/furniture | 9 (4.8) |
| Fall on same level | |
| Slipping/tripping/stumbling | 32 (17.1) |
| Other fall on same level from collision with, or pushing by, another person | 7 (4.2) |
| Other | 10 (5.0) |
| Reason for fall | |
| Slippery surface | 93 (49.7) |
| Stumbling over object | 24 (12.8) |
| Poor visibility | 26 (13.9) |
| Dizziness | 6 (3.2) |
| Others | 35 (18.7) |
| Unspecified | 3 (1.6) |
| Outcome Measure | Baseline | 1 Month | 2 Months | 4 Months | 12 Months |
|---|---|---|---|---|---|
| KOSCHI, n | n = 373 | n = 282 | n = 282 | n = 277 | n = 299 |
| Severe disability * | - | 2 | 2 | 0 | 0 |
| Moderate disability * | 1 | 12 | 6 | 3 | 0 |
| Good recovery | 1 | 45 | 15 | 15 | 0 |
| Intact recovery | 1 | 84 | 112 | 121 | 10 |
| Baseline | 1 Month | 2 Months | 4 Months | 12 Months | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| PedsQL Physical | ||||||||||
| Age (years) | N | Mean (SD) * | N | Mean (SD) * | N | mean (SD) * | N | Mean (SD) * | N | Mean (SD) * |
| 2–4 | 104 | 99.6 (2.5) | 75 | 88.5 (27.2) | 75 | 94.7 (19.0) | 77 | 99.8 (1.4) | 79 | 100 (0) |
| 5–7 | 79 | 99.4 (3.3) | 63 | 82.5 (32.4) | 63 | 94.0 (17.4) | 62 | 99.2 (6.4) | 68 | 100 (0) |
| 8–12 | 101 | 99.0 (4.6) | 81 | 73.5 (33.7) | 84 | 91.4 (23.4) | 78 | 97.8 (12.9) | 83 | 100 (0) |
| 13–16 | 89 | 99.6 (2.7) | 61 | 74.5 (31.7) | 59 | 93.6 (15.6) | 60 | 99.2 (6.5) | 69 | 99.6 (3.4) |
| PedsQL Psychosocial | ||||||||||
| 2–4 | 101 | 99.9 (0.9) | 75 | 91.8 (21.1) | 75 | 96.4 (14.6) | 77 | 100 (0) | 79 | 100 (0) |
| 5–7 | 78 | 99.5 (3.0) | 63 | 87.9 (24.1) | 63 | 95.6 (13.3) | 62 | 99.2 (6.4) | 68 | 100 (0) |
| 8–12 | 101 | 99.0 (3.9) | 81 | 83.7 (26.2) | 85 | 92.6 (21.2) | 77 | 98.9 (6.4) | 83 | 100 (0) |
| 13–16 | 88 | 99.4 (3.8) | 62 | 81.7 (23.6) | 59 | 94.5 (12.9) | 60 | 99.4 (4.3) | 69 | 100 (0) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jagnoor, J.; Prinja, S.; Christou, A.; Baker, J.; Gabbe, B.; Ivers, R. Health-Related Quality of Life and Function after Paediatric Injuries in India: A Longitudinal Study. Int. J. Environ. Res. Public Health 2017, 14, 1144. https://doi.org/10.3390/ijerph14101144
Jagnoor J, Prinja S, Christou A, Baker J, Gabbe B, Ivers R. Health-Related Quality of Life and Function after Paediatric Injuries in India: A Longitudinal Study. International Journal of Environmental Research and Public Health. 2017; 14(10):1144. https://doi.org/10.3390/ijerph14101144
Chicago/Turabian StyleJagnoor, Jagnoor, Shankar Prinja, Aliki Christou, Jannah Baker, Belinda Gabbe, and Rebecca Ivers. 2017. "Health-Related Quality of Life and Function after Paediatric Injuries in India: A Longitudinal Study" International Journal of Environmental Research and Public Health 14, no. 10: 1144. https://doi.org/10.3390/ijerph14101144
APA StyleJagnoor, J., Prinja, S., Christou, A., Baker, J., Gabbe, B., & Ivers, R. (2017). Health-Related Quality of Life and Function after Paediatric Injuries in India: A Longitudinal Study. International Journal of Environmental Research and Public Health, 14(10), 1144. https://doi.org/10.3390/ijerph14101144