Association between Obesity and Puberty Timing: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Screening and Extraction
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
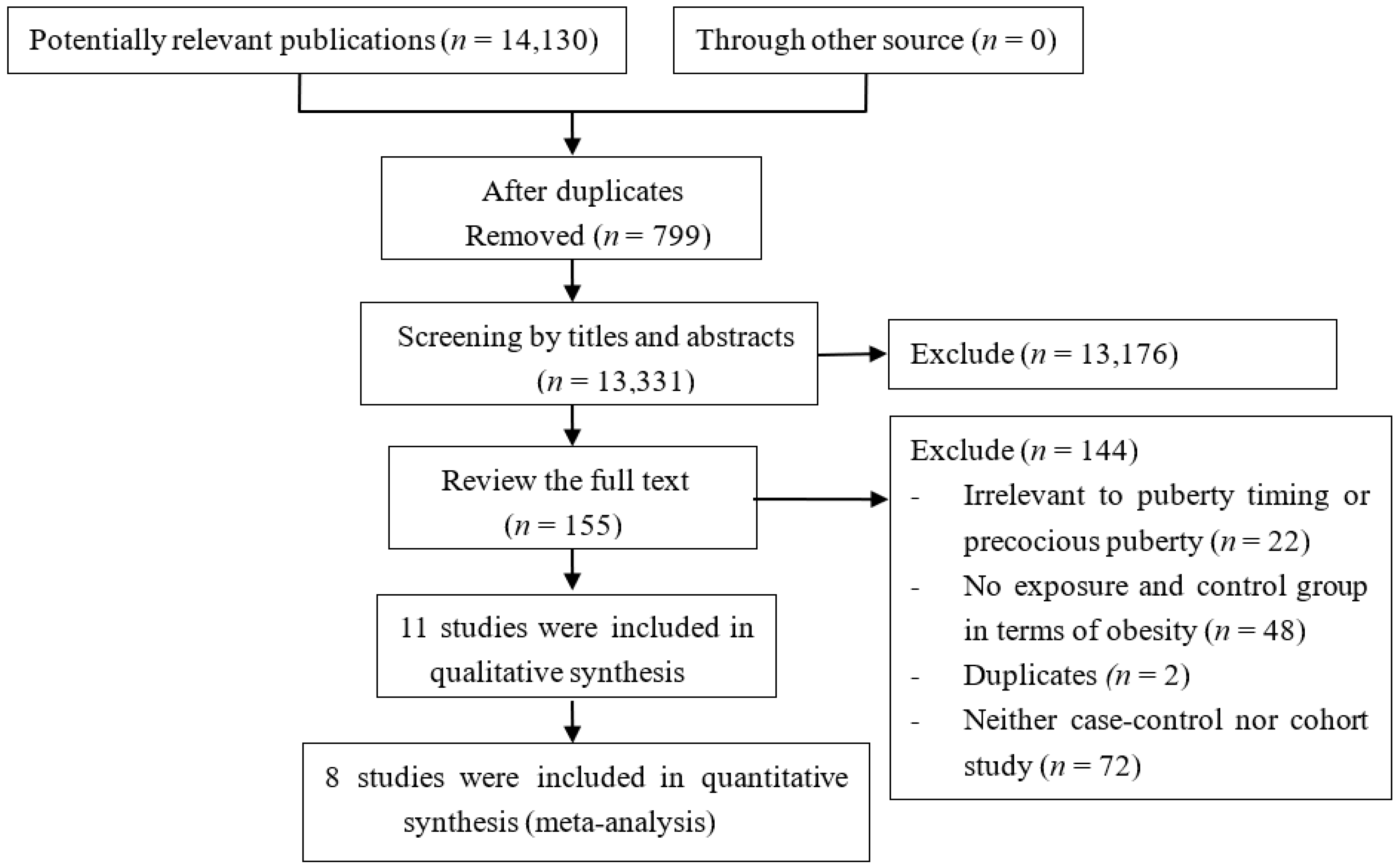
3.1. Search Results
3.2. Characteristics of Included Studies
3.3. Risk of Bias in Included Studies
3.4. Data Synthesis
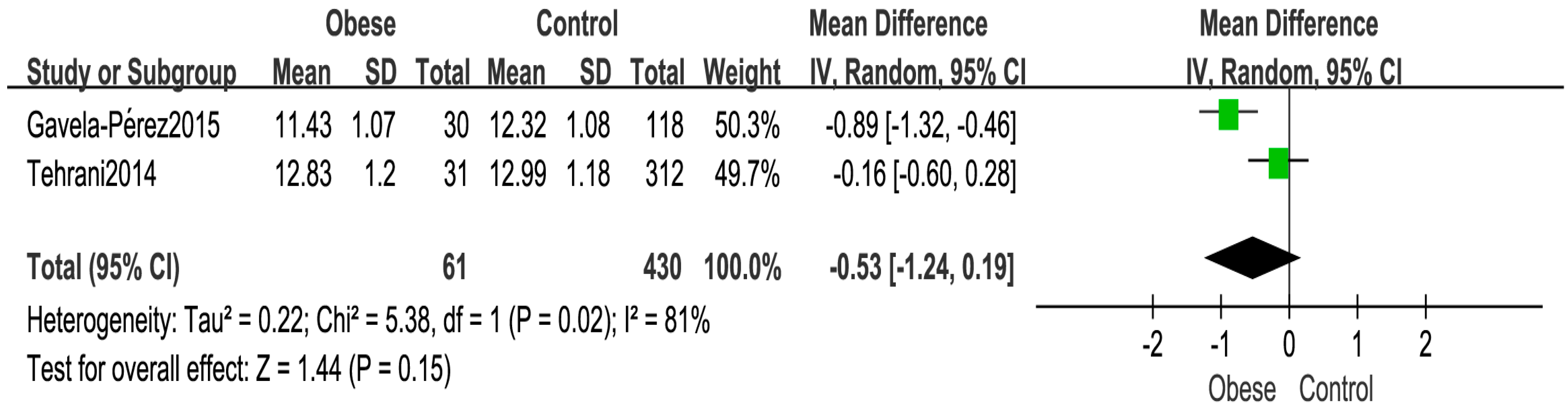
Age at Menarche
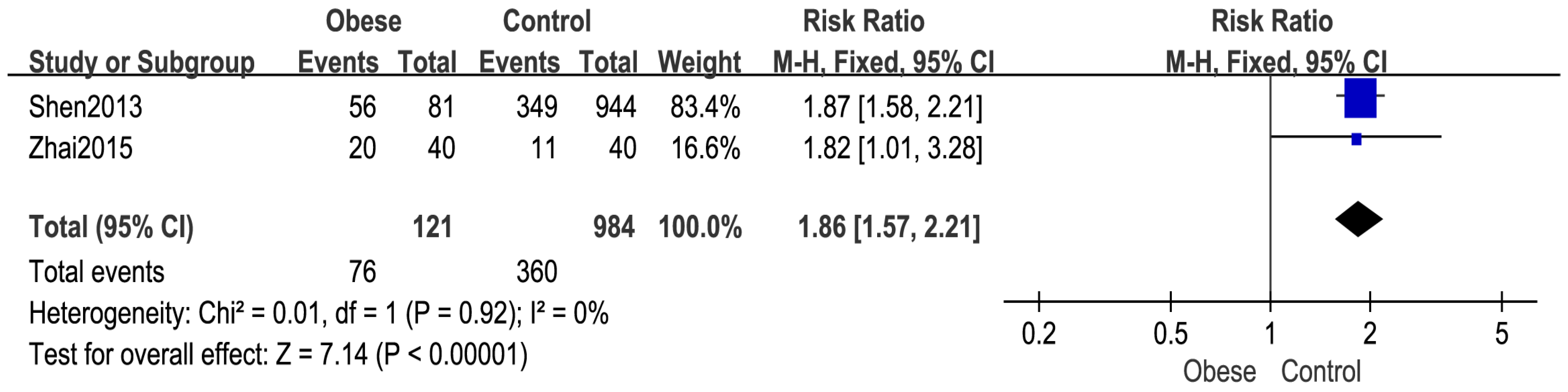
3.5. Number of Girls with Menarche
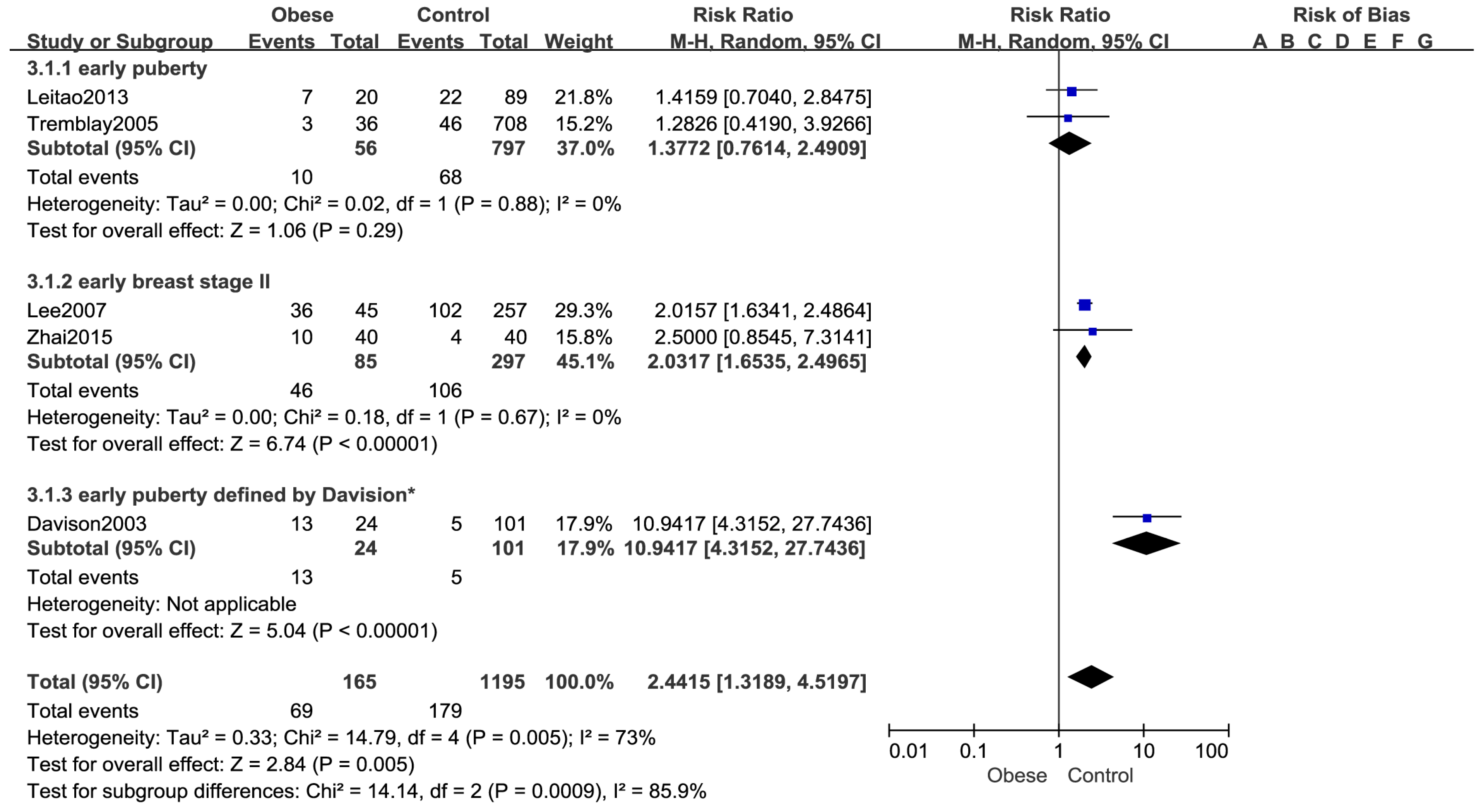
3.6. Number of Girls with Early Puberty
3.7. Breast Pubertal Development in Girls
3.8. Genitalia Development in Boys
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Patton, G.C.; Viner, R. Pubertal transitions in health. Lancet 2007, 369, 1130–1139. [Google Scholar] [CrossRef]
- Marshall, W.A.; Tanner, J.M. Variations in pattern of pubertal changes in girls. Arch. Dis. Child. 1969, 44, 291–303. [Google Scholar] [CrossRef] [PubMed]
- Marshall, W.A.; Tanner, J.M. Variations in the pattern of pubertal changes in boys. Arch. Dis. Child. 1970, 45, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.L.; Ong, K.K.; Dunger, D.B. Childhood obesity and the timing of puberty. J. Trends Endocrinol. Metable. 2009, 20, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Brooks-Gunn, J.; Petersen, A.C.; Eichorn, D. The study of maturational timing effects in adolescence. J. Youth Adolesc. 1985, 14, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Ersoy, B.; Balkan, C.; Gunay, T.; Onag, A. Egemen A. Effects of different socioeconomic conditions on menarche in Turkish female students. Early Hum. Dev. 2004, 76, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Lakshman, R.; Forouhi, N.; Luben, R.; Bingham, S.; Khaw, K.; Wareham, N.; Ong, K.K. Association between age at menarche andrisk of diabetes in adults: Results from the EPIC-Norfolk cohort study. Diabetologia 2008, 51, 781–786. [Google Scholar] [CrossRef] [PubMed]
- Velie, E.M.; Nechuta, S.; Osuch, J.R. Lifetime reproductive and anthropometric risk factors for breast cancer in postmenopausal women. Breast Dis. 2005–2006, 24, 17–35. [Google Scholar] [CrossRef]
- John, H.H. Examining in the evidence for recent secular changes in the timing of puberty in US children in light of increase in the prevalence of obesity. Mol. Cell. Endocrinol. 2006, 254–255, 13–21. [Google Scholar]
- Ong, K.K.; Emmett, P.; Northstone, K.; Golding, J.; Rogers, I.; Ness, A.R.; Wells, J.C.; Dunger, D.B. Infancy weight gain predicts childhood body fat and age at menarche in girls. J. Clin. Endocrinol. Metab. 2009, 94, 1527–1532. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Appugliese, D.; Kaciroti, N.; Corwyn, R.F.; Bradley, R.H.; Lumeng, J.C. Weight Status in Young Girls and the Onset of Puberty. Pediatrics 2007, 119, e624–e630. [Google Scholar] [CrossRef] [PubMed]
- Davison, K.K.; Susman, E.J.; Birch, L.L. Percent body fat at age 5 predicts earlier pubertal development among girls at age 9. Pediatrics 2003, 111, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Flom, J.D.; Cohn, B.A.; Tehranifar, P.; Houghton, L.C.; Wei, Y.; Protacio, A.; Cirillo, P.; Michels, K.B.; Terry, M.B. Earlier age at menarche in girls with rapid early life growth: Cohort and within sibling analyses. Ann. Epidemiol. 2017, 27, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Kelly, Y.; Zilanawala, A.; Sacker, A.; Hiatt, R.; Viner, R. Early puberty in 11-year-old girls: Millennium Cohort Study findings. Arch. Dis Child. 2017, 102, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Barcellos Gemelli, I.F.; Farias Edos, S.; Souza, O.F. Age at Menarche and Its Association with Excess Weight and Body Fat Percentage in Girls in the Southwestern Region of the Brazilian Amazon. J. Pediatr. Adolesc. Gynecol. 2016, 29, 482–488. [Google Scholar] [CrossRef] [PubMed]
- St. George, I.M.; Williams, S.; Silva, P.A. Body size and the menarche: The Dunedin Study. J. Adolesc. Health 1994, 15, 573–576. [Google Scholar] [CrossRef]
- Bau, A.M.; Ernert, A.; Schenk, L.; Wiegand, S.; Martus, P.; Grüters, A.; Krude, H. Is there a further acceleration in the age at onset of menarche? A cross-sectional study in 1840 school children focusing on ageand bodyweight at the onset of menarche. Eur. J. Endocrinol. 2009, 160, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Wronka, I. Association between BMI and age at menarche in girlsfrom different socio-economic groups. J. Anthropol. Anz. 2010, 68, 43–52. [Google Scholar] [CrossRef]
- Aksglaede, L.; Juul, A.; Olsen, L.W.; Sørensen, T.I. Age at puberty and the emerging obesity epidemic. PLoS ONE 2009, 4, e8450. [Google Scholar] [CrossRef] [PubMed]
- Herman-Giddens, M.E.; Slora, E.J.; Wasserman, R.C.; Bourdony, C.J.; Bhapkar, M.V.; Koch, G.G.; Hasemeier, C.M. Secondary sexual characteristics and menses in young girls seen in office practice: A study from the Pediatric Research in Office Settings network. J. Pediatri. 1997, 99, 505–512. [Google Scholar] [CrossRef]
- Mouritsen, A.; Aksglaede, L.; Soerensen, K.; Hagen, C.P.; Petersen, J.H.; Main, K.M.; Juul, A. The pubertal transition in 179 healthy Danish children: associations between pubarche, adrenarche, gonadarche, and body composition. Eur. J. Endocrinol. 2012, 168, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Denzer, C.; Weibel, A.; Muche, R.; Karges, B.; Sorgo, W.; Wabitsch, M. Pubertal development in obese children and adolescents. Int. J. Obes. (Lond.) 2007, 31, 1509–1519. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Wasserman, R.; Kaciroti, N.; Gebremariam, A.; Steffes, J.; Dowshen, S.; Harris, D.; Serwint, J.; Abney, D.; Smitherman, L.; et al. Timing of Puberty in Overweight Versus Obese Boys. Pediatrics 2016, 137, e20150164. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y. Is obesity associated with early sexual maturation? A comparison of the association in American boys versus girls. J. Pediatrics 2002, 110, 903–910. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peter, T.; Welc, V.; Loso, M. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-randomized Studies in Meta-Analyses. Available online: http://www.medicine.mcgill.ca/rtamblyn/Readings%5CThe%20Newcastle%20-%20Scale%20for%20assessing%20the%20quality%20of%20nonrandomised%20studies%20in%20meta-analyses.pdf (accessed on 18 October 2017).
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Sutton, A.J.; Duval, S.J.; Tweedie, R.L.; Abrams, K.R.; Jones, D.R. Empirical assessment of effect of publication bias on meta-analyses. BMJ 2000, 320, 1574–1577. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.; Zhu, D.; Zhang, M.; Qian, H.; Xu, Y. Effect on menarche contribute to body mass index changes from younger children to adolescent. Jiangsu J. Prev. Med. 2012, 24, 10–12. [Google Scholar]
- Gavela-Pérez, T.; Garcés, C.; Navarro-Sánchez, P.; López Villanueva, L.; Soriano-Guillén, L. Earlier menarcheal age in Spanish girls is related with an increase in body mass index between pre-pubertal school age and adolescence. Pediatr. Obes. 2015, 10, 410–415. [Google Scholar]
- Zhai, L.; Liu, J.; Zhao, J.; Liu, J.; Bai, Y.; Jia, L.; Yao, X. Association of Obesity with Onset of Pubertyand Sex Hormones in Chinese Girls: A 4-Year Longitudinal Study. PLoS ONE 2015, 10, e0134656. [Google Scholar] [CrossRef] [PubMed]
- Ramezani Tehrani, F.; Mirmiran, P.; Gholami, R.; Moslehi, N.; Azizi, F. Factors Influencing Menarcheal Age: Results from the Cohort of Tehran Lipid and Glucose Study. Int. J. Endocrinol. Metab. 2014, 12, e16130. [Google Scholar] [CrossRef] [PubMed]
- Leitão, R.B.; Rodrigues, L.P.; Neves, L.; Carvalho, G.S. Development of adiposity, obesity and age at menarche: An 8-year follow-up study in Portuguese schoolgirls. Int. J. Adolesc. Med. Health 2013, 25, 55–63. [Google Scholar] [CrossRef]
- Tremblay, L.; Frigon, J.Y. The interaction role of obesity and puberty timing on the psychosocial adjustment of adolescent girls: Longitudinal data. Int. J. Obes. (Lond.) 2005, 29, 1204–1211. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Kaciroti, N.; Appugliese, D.; Corwyn, R.F.; Bradley, R.H.; Lumeng, J.C. Body mass index and timing of pubertal initiation in boys. Arch. Pediatr. Adolesc. Med. 2010, 164, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Sloboda, D.M.; Hart, R.; Doherty, D.A.; Pennell, C.E.; Hickey, M. Age at menarche: Influences of prenatal and postnatal growth. J. Clin. Endocrinol. Metab. 2007, 92, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- CDC Growth Charts: United States. Available online: https://www.cdc.gov/nchs/data/ad/ad314.pdf (accessed on 21 August 2017).
- Shimizu, H.; Oh, S.; Okada, S.; Mori, M. Leptin resistance and obesity. Endocr. J. 2007, 54, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Holly, J.M.; Smith, C.P.; Dunger, D.B.; Howell, R.J.; Chard, T.; Perry, L.A.; Savage, M.O.; Cianfarani, S.; Rees, L.H.; Wass, J.A. Relationship between the pubertal fall in sex hormone binding globulin and insulin-like growth factor binding protein-I. A synchronized approach to pubertal development? Clin. Endocrinol. (Oxf.) 1989, 31, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Blank, S.K.; McCartney, C.R.; Chhabra, S.; Helm, K.D.; Eagleson, C.A.; Chang, R.J.; Marshall, J.C. Modulation of gonadotropin-releasing hormone pulse generator sensitivity to progesterone inhibition in hyperandrogenic adolescent girls—Implications for regulation of pubertal maturation. J. Clin. Endocrinol. Metable 2009, 94, 2360–2366. [Google Scholar]
- Chan, J.L.; Matarese, G.; Shetty, G.K.; Raciti, P.; Kelesidis, I.; Aufiero, D.; De Rosa, V.; Perna, F.; Fontana, S.; Mantzoros, C.S. Differential regulation of metabolic, neuroendocrine, and immune function by leptin in humans. Proc. Natl. Acad. Sci. USA 2006, 103, 8481–8486. [Google Scholar] [CrossRef] [PubMed]
- Ahima, R.S.; Dushay, J.; Flier, S.N.; Prabakaran, D.; Flier, J.S. Leptin accelerates the onset of puberty in normal female mice. J. Clin. Investig. 1997, 99, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Zhou, X. Influence and mechanism of obesity on the onset of pubertal development in obese children. Chin. J. Appl. Clin. Pediatr. 2014, 29, 574–577. [Google Scholar]
- Oh, C.M.; Oh, I.H.; Choi, K.S.; Choe, B.K.; Yoon, T.Y.; Choi, J.M. Relationship between body mass index and early menarche of adolescent girls in Seoul. J. Prev. Med. Public Health 2012, 45, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Frisch, R.E.; Revelle, R. Height and weight at menarche and a hypothesis of critical body weights and adolescent events. Science 1970, 169, 397–399. [Google Scholar] [CrossRef] [PubMed]
- Frisch, R.E.; Revelle, R. The height and weight of girls and boys at the time of initiation of the adolescent growth spurt in height and weight and the relationship to menarche. J. Hum. Biol. 1971, 43, 140–159. [Google Scholar]
- Lundeen, E.A.; Norris, S.A.; Martorell, R.; Suchdev, P.S.; Mehta, N.K.; Richter, L.M.; Stein, A.D. Early Life Growth Predicts Pubertal Development in South African Adolescents. J. Nutr. 2016, 146, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, C.T.; Skakkebaek, N.E.; Richardson, D.W.; Darling, J.A.; Hunter, W.M.; Jørgensen, M.; Nielsen, A.; Ingerslev, O.; Keiding, N.; Müller, J. Onset of the release of spermatozoa (spermarche) in boys in relation to age, testicular growth, pubic hair, and height. J. Clin. Endocrinol. Metab. 1986, 62, 532–535. [Google Scholar] [CrossRef] [PubMed]
- Qiang, M.; Sun, M.; Liu, Z.; Xing, Y.; Zhao, S. Effects of childhood obesity on early puberty: A follow-up study. Chin. J. Publ. Health 1997, 13, 409–410. [Google Scholar]
- Holmgren, A.; Niklasson, A.; Nierop, A.F.; Gelander, L.; Aronson, A.S.; Sjöberg, A.; Lissner, L.; Albertsson-Wikland, K. Pubertal height gain is inversely related to peak BMI in childhood. Pediatr. Res. 2017, 81, 448–454. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Sample Size Obesity/Control 1 | Gender | Age Interval (years) | Defined Criteria for Obesity | Study Design | Primary Outcome | Quality Score |
|---|---|---|---|---|---|---|---|---|
| Shen 2013 [28] | China | 81/944 | Girls | 7.02–12.02 | BMI ≥ 95th percentile | Cohort | No. of girls that had menarche | 8 |
| Gavela-Pérez 2015 [29] | Spain | 30/118 | Girls | 7.23–14.61 | According to Cole [36] | Cohort | Age at menarche | 8 |
| Zhai 2015 [30] | China | 40/40 | Girls | 8.5–12.5 | Percentage of body fat using skin-fold thickness: ≥25% | Cohort | No. of girls that had menarche No. of girls with breast stage 2 No. of girls with early puberty 2 | 9 |
| Ramezani Tehrani 2014 [31] | Iran | 31/312 | Girls | 12–18 | BMI > 95th percentile | Cohort | Age at menarche | 8 |
| Lee 2007 [11] | US | 5/257 | Girls | 3–12 | BMI ≥ 95th percentile | Cohort | No. of girls with early puberty 3 | 9 |
| Leitao 2013 [32] | Portugal | 20/89 | Girls | 7–15 | ≥30 % body fat | Cohort | No. of girls with early puberty 4 | 9 |
| Tremblay 2005 [33] | Canada | 36/708 | Girls | 11–13 | BMI ≥ 95th percentile | Cohort | No. of girls with early puberty 5 | 8 |
| Davison 2003 [12] | US | 24/101 | Girls | 5–9 | According to 2000 growth charts from the Centers for Disease Control and Prevention [37] | Cohort | No. of girls with early puberty 6 | 7 |
| Study | Country | Sample Size | Gender | Age Interval (years) | The Basis of Grouping | Study Design | Outcome Measures | Results | Quality Score |
|---|---|---|---|---|---|---|---|---|---|
| Lee 2010 [34] | US | 401 | Boys | 2–11.5 | Highest BMI z score trajectories group (mean BMI z score of 1.84 (0.50) at age 11.5 years Intermediate BMI z score trajectories group (mean BMI z score of 0.41 (0.70) at age 11.5 years Lowest BMI z score trajectories group (mean BMI z score of −0.76 (0.63) at age 11.5 years | Cohort | Tanner genitalia stage | Boys in the highest BMI trajectory had a greater relative risk of being prepubertal 1 compare with boys in the lowest BMI trajectory (RR: 2.63, 95% CI: 1.05–6.61) | 8 |
| Deborah 2006 [35] | Australia | 776 | Girls | 1–13 | According to the median of BMI (16.3) in this study. Expose group: BMI ≥ 16.3 Control group: BMI <16.3 | Cohort | Age at menarche | Eight-year-old girls with a BMI above the median had significantly earlier menarche compared with those with BMI below the median (HR: 1.65, 95% CI: 1.33–2.05) | 8 |
| Flom 2017 [13] | US | 788 | Girls | From birth to menarche occurred | Expose group: BMI ≥ 85th percentile Control group: BMI < 85th percentile | Cohort | Age at menarche | Overweight/obese status at the age of 7 year was associated with increased risk of early menarche 2 (OR = 1.79, 95% CI: 1.20–2.67) | 9 |
| Study | Selection | Comparability | Outcome | Score 1 | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the Expose Cohort | Selection of the Non-Exposed Cohort | Ascertainment of Exposure | Demonstration That Outcome of Interest Was not Present at Start of Study | Comparability of Cohorts on the Basis of the Design or Analysis | Assessment of Outcome | Was follow-up Long Enough for Outcomes to Occur | Adequacy of Follow up of Cohorts | ||
| Shen 2013 [28] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Gavela-Pérez 2015 [29] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Zhai 2015 [30] | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| Ramezani Tehrani 2014 [31] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Lee 2007 [11] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
| Leitao 2013 [32] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
| Tremblay 2005 [33] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| Davison 2003 [12] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 7 |
| Lee 2010 [34] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| Deborah 2006 [35] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| Flom 2017 [13] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, W.; Liu, Q.; Deng, X.; Chen, Y.; Liu, S.; Story, M. Association between Obesity and Puberty Timing: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2017, 14, 1266. https://doi.org/10.3390/ijerph14101266
Li W, Liu Q, Deng X, Chen Y, Liu S, Story M. Association between Obesity and Puberty Timing: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2017; 14(10):1266. https://doi.org/10.3390/ijerph14101266
Chicago/Turabian StyleLi, Wenyan, Qin Liu, Xu Deng, Yiwen Chen, Shudan Liu, and Mary Story. 2017. "Association between Obesity and Puberty Timing: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 14, no. 10: 1266. https://doi.org/10.3390/ijerph14101266
APA StyleLi, W., Liu, Q., Deng, X., Chen, Y., Liu, S., & Story, M. (2017). Association between Obesity and Puberty Timing: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 14(10), 1266. https://doi.org/10.3390/ijerph14101266