Chronic Stress in Young German Adults: Who Is Affected? A Prospective Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
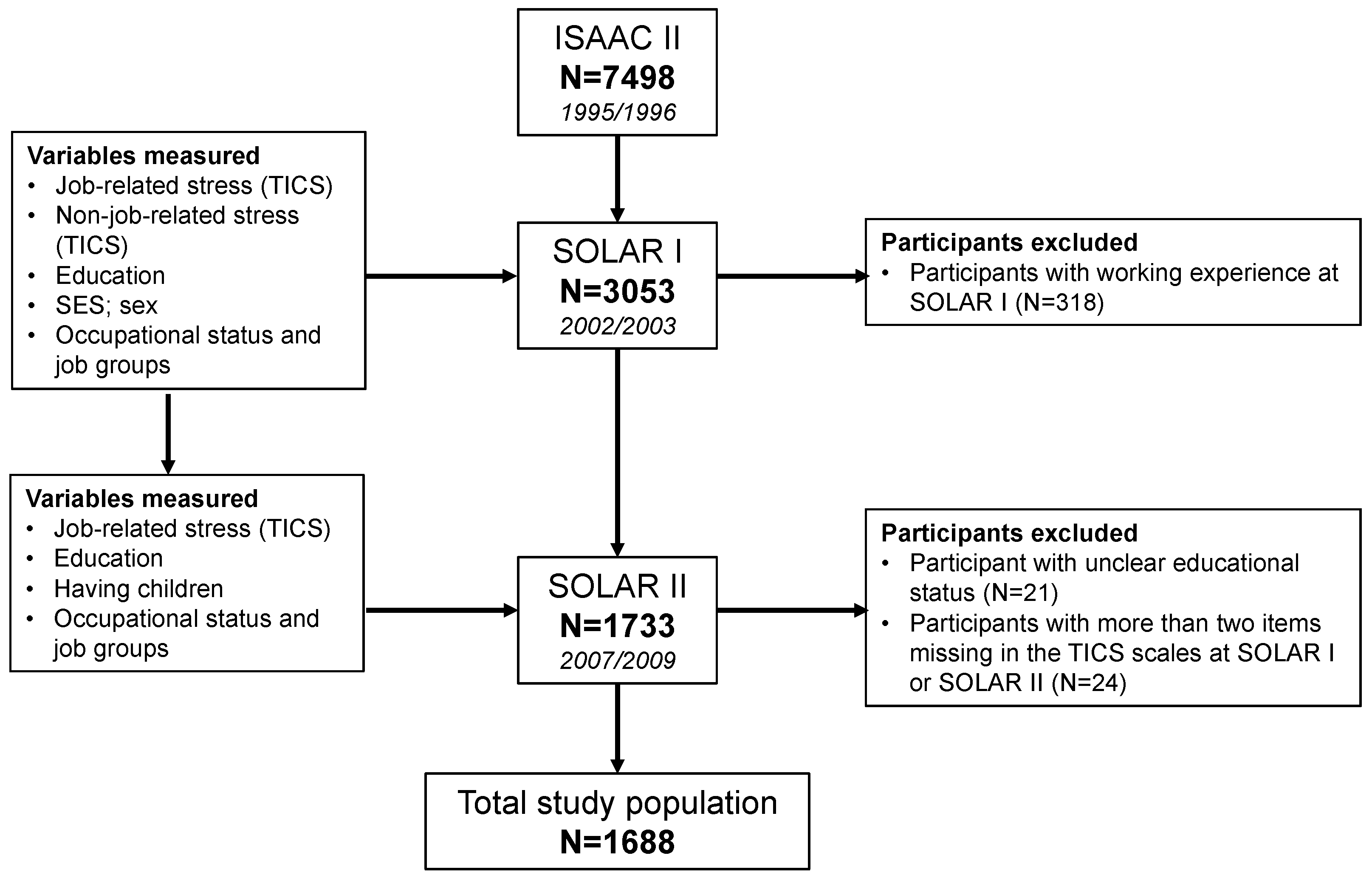
2.1. Population
2.2. Occupational Status and Job Groups
2.3. Sociodemographics Covariates
2.4. Non-Job-Related Chronic Stress
- social overload (e.g., “Situations in which I cannot resolve conflicts that I have with others”.);
- lack of social recognition (e.g., “Times where I get little approval for my work”.);
- chronic worrying (e.g., “Times when I worry a lot and cannot stop”.);
- stressful memories (e.g., “Intrusive remembrances of an unpleasant experience”.).
2.5. Work-/University-Related Chronic Stress as Outcome
- work discontent (e.g., “Times when I have to perform tasks that I am not at all willing to do”.);
- work overload (e.g., “I have too many tasks to perform”.).
2.6. Statistical Analysis
3. Results
3.1. Descriptives
3.2. GEE Models
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Michie, S. Causes and management of stress at work. Occup. Environ. Med. 2002, 59, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Gilbert-Ouimet, M.; Trudel, X.; Brisson, C.; Milot, A.; Vézina, M. Adverse effects of psychosocial work factors on blood pressure: Systematic review of studies on demand-control-support and effort-reward imbalance models. Scand. J. Work Environ. Health 2014, 40, 109–132. [Google Scholar] [CrossRef] [PubMed]
- Hassoun, L.; Herrmann-Lingen, C.; Hapke, U.; Neuhauser, H.; Scheidt-Nave, C.; Meyer, T. Association between chronic stress and blood pressure: Findings from the german health interview and examination survey for adults 2008–2011. Psychosom. Med. 2015, 77, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Bonzini, M.; Veronesi, G.; Conti, M.; Coggon, D.; Ferrario, M.M. Is musculoskeletal pain a consequence or a cause of occupational stress? A longitudinal study. Int. Arch. Occup. Environ. Health 2015, 88, 607–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melchior, M.; Caspi, A.; Milne, B.J.; Danese, A.; Poulton, R.; Moffitt, T.E. Work stress precipitates depression and anxiety in young, working women and men. Psychol. Med. 2007, 37, 1119–1129. [Google Scholar] [CrossRef] [PubMed]
- Schulz, P.; Schlotz, W. Trier inventory for the assessment of chronic stress (tics): Scale construction, statistical testing, and validation of the scale work overload. Diagnostica 1999. [Google Scholar] [CrossRef]
- Becker, P.; Schulz, P.; Schlotz, W. Persönlichkeit, chronischer stress und körperliche gesundheit: Eine prospektive studie zur überprüfung eines systemischen anforderungs-ressourcen-modells. Zeitschrift für Gesundheitspsychologie 2004, 12, 11–23. [Google Scholar] [CrossRef]
- Schlotz, W.; Phillips, D.I. Birth weight and perceived stress reactivity in older age. Stress Health 2013, 29, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Hahn, S.E.; Smith, C.S. Daily hassles and chronic stressors: Conceptual and measurement issues. Stress Health 1999, 15, 89–101. [Google Scholar] [CrossRef]
- Barling, J.; Kelloway, E.K.; Frone, M.R. Handbook of Work Stress; Sage Publications: Thousand Oaks, CA, USA, 2004. [Google Scholar]
- Marinaccio, A.; Ferrante, P.; Corfiati, M.; Di Tecco, C.; Rondinone, B.M.; Bonafede, M.; Ronchetti, M.; Persechino, B.; Iavicoli, S. The relevance of socio-demographic and occupational variables for the assessment of work-related stress risk. BMC Public Health 2013, 13, 1157. [Google Scholar] [CrossRef] [PubMed]
- Mauno, S.; Ruokolainen, M.; Kinnunen, U. Does aging make employees more resilient to job stress? Age as a moderator in the job stressor-well-being relationship in three finnish occupational samples. Aging Mental Health 2013, 17, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Ștefănescu-Mihăilă, R.O. Social investment, economic growth and labor market performance: Case study—Romania. Sustainability 2015, 7, 2961–2979. [Google Scholar] [CrossRef]
- Hapke, U.; Maske, U.; Scheidt-Nave, C.; Bode, L.; Schlack, R.; Busch, M. Chronic stress among adults in germany: Results of the german health interview and examination survey for adults (degs1). Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 2013, 56, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Froneberg, B.; Timm, S. Country Profile of Occupational Health System in Germany; WHO Regional Office for Europe: Copenhagen, Denmark, 2012. [Google Scholar]
- Pidgeon, A.M.; McGrath, S.; Magya, H.B.; Stapleton, P.; Lo, B.C. Psychosocial moderators of perceived stress, anxiety and depression in university students: An international study. Open J. Soc. Sci. 2014, 2, 23. [Google Scholar] [CrossRef]
- Tavolacci, M.P.; Ladner, J.; Grigioni, S.; Richard, L.; Villet, H.; Dechelotte, P. Prevalence and association of perceived stress, substance use and behavioral addictions: A cross-sectional study among university students in france, 2009–2011. BMC Public Health 2013, 13, 724. [Google Scholar] [CrossRef] [PubMed]
- Bewick, B.; Koutsopoulou, G.; Miles, J.; Slaa, E.; Barkham, M. Changes in undergraduate students’ psychological well-being as they progress through university. Stud. Higher Educ. 2010, 35, 633–645. [Google Scholar] [CrossRef]
- Vaez, M.; Kristenson, M.; Laflamme, L. Perceived quality of life and self-rated health among first-year university students. Soc. Indic. Res. 2004, 68, 221–234. [Google Scholar] [CrossRef]
- Stewart-Brown, S.; Evans, J.; Patterson, J.; Petersen, S.; Doll, H.; Balding, J.; Regis, D. The health of students in institutes of higher education: An important and neglected public health problem? J. Public Health 2000, 22, 492–499. [Google Scholar] [CrossRef]
- Hammen, C.; Dalton, E.D.; Thompson, S.M. Measurement of chronic stress. In Encyclopedia of Clinical Psychology; Wiley-Blackwell: Hoboken, NJ, USA, 2015. [Google Scholar]
- Petrowski, K.; Paul, S.; Albani, C.; Brähler, E. Factor structure and psychometric properties of the trier inventory for chronic stress (tics) in a representative german sample. BMC Med. Res. Methodol. 2012, 12, 42. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, S.; Peters, A.; Kellberger, J.; Ellenberg, D.; Genuneit, J.; Nowak, D.; Vogelberg, C.; von Mutius, E.; Weinmayr, G.; Radon, K. Study on occupational allergy risks (solar II) in germany: Design and methods. BMC Public Health 2011, 11, 298. [Google Scholar] [CrossRef] [PubMed]
- Weiland, S.; Björkstén, B.; Brunekreef, B.; Cookson, W.; Von Mutius, E.; Strachan, D. Phase ii of the international study of asthma and allergies in childhood (ISAAC II): Rationale and methods. Eur. Respir. J. 2004, 24, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Wolf, C. The isco-88 international standard classification of occupations in cross-national survey research. Bull. Sociol. Methodol. 1997, 54, 23–40. [Google Scholar]
- Hubbard, A.E.; Ahern, J.; Fleischer, N.L.; Van der Laan, M.; Lippman, S.A.; Jewell, N.; Bruckner, T.; Satariano, W.A. To gee or not to gee: Comparing population average and mixed models for estimating the associations between neighborhood risk factors and health. Epidemiology 2010, 21, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Touloumis, A.; Agresti, A.; Kateri, M. Gee for multinomial responses using a local odds ratios parameterization. Biometrics 2013, 69, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Zorn, C.J. Generalized estimating equation models for correlated data: A review with applications. Am. J. Political Sci. 2001, 45, 470–490. [Google Scholar] [CrossRef]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef] [PubMed]
- Little, R.J.; Rubin, D.B. Statistical Analysis with Missing Data; John Wiley & Sons: Hoboken, NJ, USA, 2014. [Google Scholar]
- Lourenço, S.; Carnide, F.; Benavides, F.G.; Lucas, R. Psychosocial work environment and musculoskeletal symptoms among 21-year-old workers: A population-based investigation (2011–2013). PLoS ONE 2015, 10, e0130010. [Google Scholar] [CrossRef] [PubMed]
- Macan, T.H.; Shahani, C.; Dipboye, R.L.; Phillips, A.P. College students’ time management: Correlations with academic performance and stress. J. Educ. Psychol. 1990, 82, 760. [Google Scholar] [CrossRef]
- Misra, R.; McKean, M. College students’ academic stress and its relation to their anxiety, time management, and leisure satisfaction. Am. J. Health Stud. 2000, 16, 41. [Google Scholar]
- Regehr, C.; Glancy, D.; Pitts, A. Interventions to reduce stress in university students: A review and meta-analysis. J. Affect. Disord. 2013, 148, 1–11. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.D.; Kutney-Lee, A.; Cimiotti, J.P.; Sloane, D.M.; Aiken, L.H. Nurses’ widespread job dissatisfaction, burnout, and frustration with health benefits signal problems for patient care. Health Aff. 2011, 30, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Blegen, M.A. Nurses’ job satisfaction: A meta-analysis of related variables. Nurs. Res. 1993, 42, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Scheidt-Nave, C.; Kamtsiuris, P.; Gößwald, A.; Hölling, H.; Lange, M.; Busch, M.A.; Dahm, S.; Dölle, R.; Ellert, U.; Fuchs, J. German health interview and examination survey for adults (degs)-design, objectives and implementation of the first data collection wave. BMC Public Health 2012, 12, 730. [Google Scholar] [CrossRef] [PubMed]
- De Smet, P.; Sans, S.; Dramaix, M.; Boulenguez, C.; De Backer, G.; Ferrario, M.; Cesana, G.; Houtman, I.; Isacsson, S.; Kittel, F. Gender and regional differences in perceived job stress across europe. Eur. J. Public Health 2005, 15, 536–545. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| SOLAR I | SOLAR II | |||
|---|---|---|---|---|
| % | (n) | % | (n) | |
| Occupation (NA = 5) | ||||
| Employed | 0 | 0 | 22 | 376 |
| Student | 89 | 1497 | 52 | 879 |
| Apprentice | 10 | 168 | 19 | 314 |
| Unemployed | 0 | 0 | 4 | 60 |
| Other | 1 | 23 | 2 | 42 |
| Self-employed | 0 | 0 | 1 | 12 |
| Clerks | - | - | 10 | 163 |
| Professionals and technicians | - | - | 19 | 328 |
| Health professions | - | - | 12 | 209 |
| Plant machine operators | - | - | 15 | 260 |
| Elementary occupations | - | - | 6 | 93 |
| Sex | ||||
| Female | 59 | 991 | - | - |
| Having children (NA = 10) | ||||
| Yes | - | - | 3 | 52 |
| Parental socio economic status ** (NA = 19) | ||||
| High | 64 | 1063 | - | - |
| Low | 36 | 606 | - | - |
| Education (NA = 33) | ||||
| Elementary | 74 | 1220 | 0 | 8 |
| Secondary | 26 | 432 | 26 | 432 |
| Advanced technical | 0 | 3 | 12 | 199 |
| Higher | 0 | 0 | 62 | 1043 |
| Work discontent †† (NA = 17) | ||||
| Low | 52 | 872 | 68 | 1137 |
| Average | 29 | 483 | 19 | 326 |
| High | 19 | 316 | 13 | 215 |
| Median (SD) | 13 | (3.3) | 12 | (3.4) |
| Work overload †† (NA = 17) | ||||
| Low | 55 | 920 | 53 | 882 |
| Average | 28 | 475 | 27 | 449 |
| High | 17 | 276 | 21 | 348 |
| Median (SD) | 20 | (5.6) | 20 | (6.0) |
| Social overload (NA = 15) | ||||
| Low | 39 | 659 | - | - |
| Average | 43 | 724 | - | - |
| High | 17 | 290 | - | - |
| Median (SD) | 14 | (3.4) | - | - |
| Lack of social recognition (NA = 11) | ||||
| Low | 56 | 943 | - | - |
| Average | 30 | 499 | - | - |
| High | 14 | 231 | - | - |
| Median (SD) | 17 | (4.1) | - | - |
| Chronic worrying (NA = 17) | ||||
| Low | 51 | 853 | - | - |
| Average | 28 | 474 | - | - |
| High | 21 | 344 | - | - |
| Median (SD) | 15 | (4.5) | - | - |
| Stressful memories (NA = 12) | ||||
| Low | 53 | 882 | - | - |
| Average | 26 | 436 | - | - |
| High | 21 | 358 | - | - |
| Median (SD) | 13 | (4.6) | - | - |
| Univariate | Model 1 # | Model 2 # | Model 3 # | |
|---|---|---|---|---|
| OR (95% CI) | aOR (95% CI) | aOR (95% CI) | aOR (95% CI) | |
| Follow-up | ||||
| SOLAR I | 1 | - | 1 | 1 |
| SOLAR II | 1.12 (1.04, 1.20) * | 1.51 (1.23, 1.85) * | 1.50 (1.23, 1.84) * | 1.55 (1.22, 1.95) * |
| Occupation | ||||
| Employed | 1 | 1 | 1 | 1 |
| Student | 1.01 (0.89, 1.16) | 1.30 (1.08, 1.57) * | 1.30 (1.08, 1.57) * | 1.33 (1.07, 1.67) * |
| Vocational trainee | 0.96 (0.82, 1.13) | 1.11 (0.92, 1.33) | 1.10 (0.92, 1.33) | 1.07 (0.86, 1.34) |
| Unemployed | 0.71 (0.49, 1.03) | 0.70 (0.47, 1.05) | 0.70 (0.47, 1.05) | 0.62 (0.39, 1.00) |
| Other | 1.10 (0.77, 1.57) | 1.09 (0.73, 1.62) | 1.08 (0.73, 1.61) | 1.07 (0.69, 1.67) |
| Self-employed | 2.08 (1.10, 3.94) * | 2.32 (1.16, 4.62) * | 2.34 (1.16, 4.69) * | 2.55 (1.16, 5.58) * |
| Clerk ** | ||||
| Yes | 1.04 (0.88, 1.24) | - | 0.98 (0.82, 1.16) | 1.04 (0.87, 1.25) |
| Professionals and technicians ** | ||||
| Yes | 0.99 (0.87, 1.13) | - | 0.95 (0.83, 1.09) | 0.94 (0.82, 1.08) |
| Health professions ** | ||||
| Yes | 1.19 (1.02, 1.38) * | - | 1.20 (1.03, 1.41) * | 1.17 (1.01, 1.37) * |
| Plant machine operators ** | ||||
| Yes | 0.81 (0.70, 0.93) * | - | 0.91 (0.79, 1.06) | 0.92 (0.79, 1.08) |
| Elementary occupations ** | ||||
| Yes | 1.00 (0.83, 1.22) | - | 1.07 (0.87, 1.32) | 1.01 (0.81, 1.27) |
| Sex | ||||
| Male | 1 | 1 | 1 | 1 |
| Female | 1.77 (1.59, 1.97) * | 1.78 (1.59, 1.99) * | 1.77 (1.58, 1.97) * | 1.35 (1.22, 1.53) * |
| Having children ** | ||||
| Yes | 1.54 (1.19, 1.99) * | 1.41 (1.08, 1.83) * | 1.42 (1.09, 1.86) * | 1.46 (1.10, 1.93) * |
| Parental socio economic status | ||||
| High | 1 | 1 | 1 | 1 |
| Low | 0.93 (0.83, 1.03) | 0.93 (0.83, 1.04) | 0.94 (0.84, 1.05) | 0.88 (0.79, 0.99) * |
| Education | ||||
| Elementary | 1 | 1 | 1 | 1 |
| Secondary | 0.95 (0.86, 1.06) | 0.88 (0.76, 1.01) | 0.89 (0.77, 1.03) | 0.87 (0.75, 1.01) |
| Advanced technical | 1.17 (0.99, 1.39) | 0.87 (0.67, 1.13) | 0.88 (0.68, 1.14) | 0.86 (0.65, 1.15) |
| Higher | 1.08 (0.99, 1.18) | 0.74 (0.60, 0.92) * | 0.75 (0.60, 0.93) * | 0.77 (0.60, 0.98) * |
| Social overload †† | ||||
| Average | 1.50 (1.34, 1.67) * | - | - | 1.24 (1.10, 1.41) * |
| High | 2.48 (2.16, 2.85) * | - | - | 1.42 (1.20, 1.68) * |
| Lack of social recognition †† | ||||
| Average | 1.46 (1.30, 1.64) * | - | - | 1.08 (0.96, 1.23) |
| High | 2.10 (1.82, 2.42) * | - | - | 1.16 (0.99, 1.40) |
| Chronic worrying †† | ||||
| Average | 2.26 (1.99, 2.56) * | - | - | 1.82 (1.58, 2.09) * |
| High | 4.04 (3.50, 4.66) * | - | - | 2.89 (2.41, 3.46) * |
| Stressful memories †† | ||||
| Average | 1.82 (1.61, 2.07) * | - | - | 1.20 (1.04, 1.38) * |
| High | 2.59 (2.28, 2.95) * | - | - | 1.13 (0.95, 1.35) |
| Univariate | Model 1 # | Model 2 # | Model 3 # | |
|---|---|---|---|---|
| OR (95% CI) | aOR (95% CI) | aOR (95% CI) | aOR (95% CI) | |
| Follow-Up | ||||
| SOLAR I | 1 | 1 | 1 | 1 |
| SOLAR II | 0.68 (0.63, 0.74) * | 1.11 (0.90, 1.38) | 1.11 (0.90, 1.38) | 1.08 (0.86, 1.36) |
| Occupation | ||||
| Employed | 1 | 1 | 1 | 1 |
| Student | 1.25 (1.06, 1.46) * | 1.08 (0.87, 1.35) | 1.10 (0.88, 1.37) | 1.06 (0.84, 1.34) |
| Apprentice | 0.97 (0.80, 1.18) | 0.98 (0.80, 1.22) | 0.99 (0.80, 1.22) | 0.91 (0.72, 1.14) |
| Unemployed | 2.04 (1.48, 2.82) * | 2.08 (1.50, 2.88) * | 2.10 (1.52, 2.91) * | 2.15 (1.50, 3.09) * |
| Other | 1.52 (1.07, 2.18) * | 1.49 (1.01, 2.19) * | 1.50 (1.02, 2.21) * | 1.46 (0.95, 2.26) |
| Self-employed | 0.69 (0.21, 2.20) | 0.71 (0.24, 2.14) | 0.70 (0.24, 2.05) | 0.61 (0.19, 1.98) |
| Clerk ** | ||||
| Yes | 0.82 (0.69, 0.97) * | - | 0.79 (0.66, 0.95) * | 0.81 (0.68, 0.98) * |
| Professionals and technicians ** | ||||
| Yes | 0.91 (0.80, 1.03) | - | 0.90 (0.79, 1.02) | 0.90 (0.79, 1.04) |
| Health professions ** | ||||
| Yes | 0.86 (0.73, 1.01) | - | 0.84 (0.71, 1.00) | 0.80 (0.67, 0.95) * |
| Plant machine operators ** | ||||
| Yes | 0.84 (0.72, 0.97) * | - | 0.81 (0.70, 0.95) * | 0.82 (0.70, 0.96) * |
| Elementary occupations ** | ||||
| Yes | 0.98 (0.79, 1.21) | - | 0.99 (0.80, 1.24) | 0.94 (0.74, 1.19) |
| Sex | ||||
| Men | 1 | 1 | 1 | 1 |
| Women | 1.11 (1.01, 1.23) * | 1.12 (1.01, 1.25) * | 1.11 (1.00, 1.23) | 0.89 (0.80, 1.00) |
| Having children ** | ||||
| Yes | 1.10 (0.86, 1.40) | 0.91 (0.70, 1.19) | 0.89 (0.68, 1.18) | 0.89 (0.67, 1.18) |
| Parental socioeconomic status | ||||
| High | 1 | 1 | 1 | 1 |
| Low | 1.00 (0.91, 1.11) | 0.96 (0.86, 1.07) | 0.95 (0.85, 1.06) | 0.91 (0.81, 1.02) |
| Education | ||||
| Elementary | 1 | 1 | 1 | 1 |
| Secondary | 0.75 (0.67, 0.84) * | 0.72 (0.62, 0.83) * | 0.71 (0.62, 0.82) * | 0.70 (0.60, 0.81) * |
| Advanced technical | 0.73 (0.60, 0.88) * | 0.64 (0.49, 0.84) * | 0.65 (0.49, 0.85) * | 0.60 (0.45, 0.81) * |
| Higher | 0.54 (0.48, 0.60) * | 0.48 (0.38, 0.61) * | 0.48 (0.38, 0.61) * | 0.47 (0.37, 0.61) * |
| Social overload †† | ||||
| Average | 1.48 (1.33, 1.64) * | - | - | 1.09 (0.96, 1.23) |
| High | 2.02 (1.77, 2.31) * | - | - | 1.17 (0.98, 1.38) |
| Lack of social recognition †† | ||||
| Average | 1.60 (1.43, 1.79) * | - | - | 1.38 (1.22, 1.57) * |
| High | 2.53 (2.20, 2.89) * | - | - | 1.94 (1.64, 2.30) * |
| Chronic worrying †† | ||||
| Average | 1.65 (1.47, 1.86) * | - | - | 1.41 (1.23, 1.62) * |
| High | 2.26 (1.99, 2.56) * | - | - | 1.72 (1.45, 2.05) * |
| Stressful memories †† | ||||
| Average | 1.53 (1.36, 1.72) * | - | - | 1.19 (1.04, 1.36) * |
| High | 1.92 (1.70, 2.16) * | - | - | 1.11 (0.94, 1.31) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrera, R.; Berger, U.; Genuneit, J.; Gerlich, J.; Nowak, D.; Schlotz, W.; Vogelberg, C.; Von Mutius, E.; Weinmayr, G.; Windstetter, D.; et al. Chronic Stress in Young German Adults: Who Is Affected? A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2017, 14, 1325. https://doi.org/10.3390/ijerph14111325
Herrera R, Berger U, Genuneit J, Gerlich J, Nowak D, Schlotz W, Vogelberg C, Von Mutius E, Weinmayr G, Windstetter D, et al. Chronic Stress in Young German Adults: Who Is Affected? A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2017; 14(11):1325. https://doi.org/10.3390/ijerph14111325
Chicago/Turabian StyleHerrera, Ronald, Ursula Berger, Jon Genuneit, Jessica Gerlich, Dennis Nowak, Wolff Schlotz, Christian Vogelberg, Erika Von Mutius, Gudrun Weinmayr, Doris Windstetter, and et al. 2017. "Chronic Stress in Young German Adults: Who Is Affected? A Prospective Cohort Study" International Journal of Environmental Research and Public Health 14, no. 11: 1325. https://doi.org/10.3390/ijerph14111325
APA StyleHerrera, R., Berger, U., Genuneit, J., Gerlich, J., Nowak, D., Schlotz, W., Vogelberg, C., Von Mutius, E., Weinmayr, G., Windstetter, D., Weigl, M., & Radon, K. (2017). Chronic Stress in Young German Adults: Who Is Affected? A Prospective Cohort Study. International Journal of Environmental Research and Public Health, 14(11), 1325. https://doi.org/10.3390/ijerph14111325