Nutrition in the First 1000 Days: Ten Practices to Minimize Obesity Emerging from Published Science


Abstract
:1. Introduction
2. Practice One: Both Mother and Father Behavior Are Important
3. Practice Two: Systematize Body Composition Measurement to Monitor Growth
4. Practice Three: Exclusive Breastfeeding for the Best Start in Life
5. Practice Four: Window to Introduce Complementary Feeding
6. Practice Five: Fruit and Vegetable Liking Begins Early
7. Practice Six: Respect for the Child’s Appetite
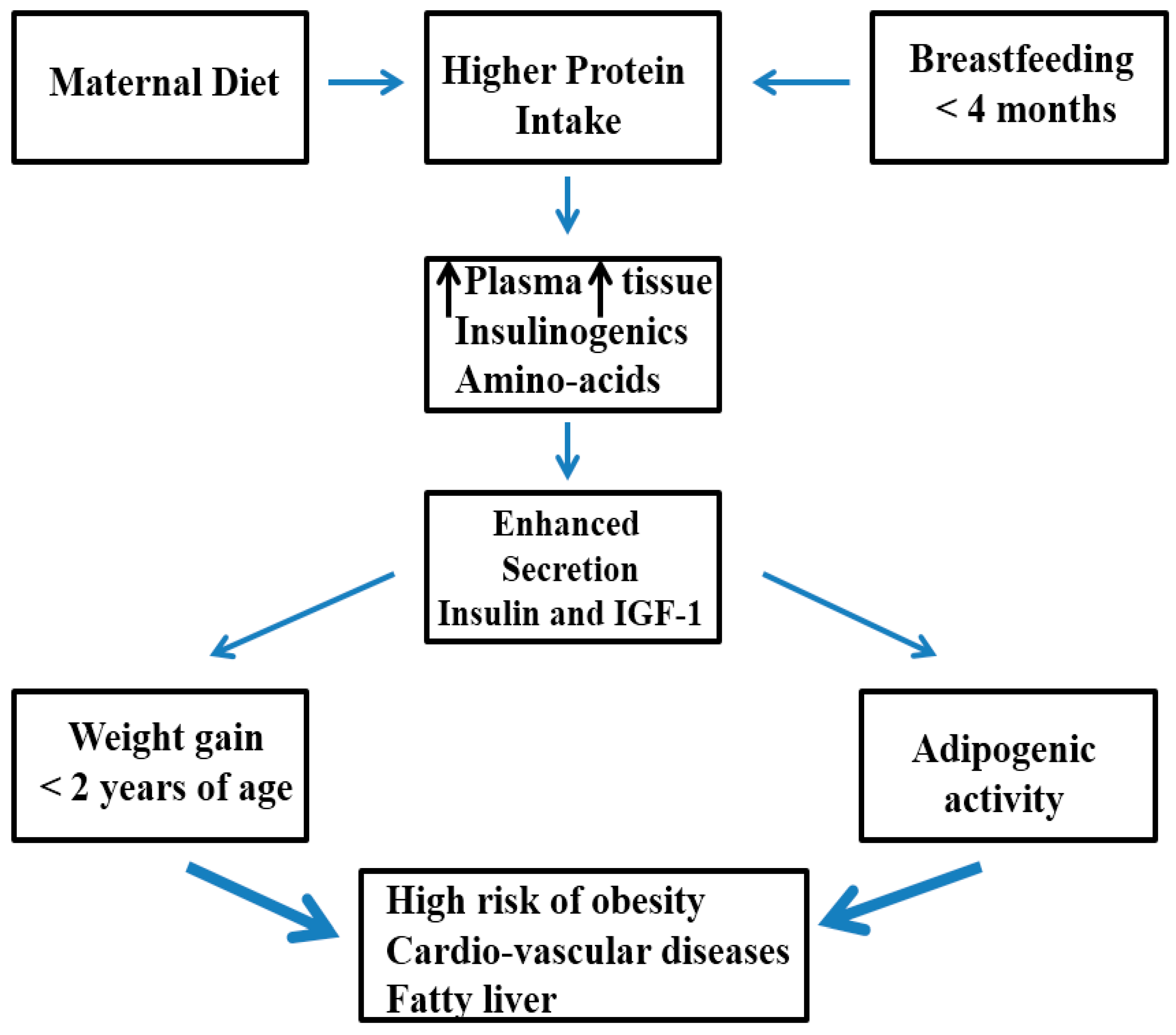
8. Practice Seven: Limit Animal Protein Intake
9. Practice Eight: Promote Qualitative and Adequate Fat Intake
10. Practice Nine: Parents Be a Role Model
11. Practice Ten: Promoting Physical Activity and Good Sleep
12. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- De Onis, M.; Blössner, M.; Borghi, E. Global prevalence and trends of overweight and obesity among preschool children. Am. J. Clin. Nutr. 2010, 92, 1257–1264. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, P.; Bedogni, G.; Pietrobelli, A.; Cianfarani, S.; Agostoni, C. Predictors of blood pressure at 7–13 years: The “new millennium baby” study. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Rudolf, M. Predicting babies’ risk of obesity. Arch. Dis. Child. 2011, 96, 995–997. [Google Scholar] [CrossRef] [PubMed]
- Fraser, A.; Macdonald-Wallis, C.; Tilling, K.; Boyd, A.; Golding, J.; Davey Smith, G.; Henderson, J.; Macleod, J.; Molloy, L.; Ness, A.; et al. Cohort profile: The Avon longitudinal study of parents and children: ALSPAC mothers cohort. Int. J. Epidemiol. 2013, 42, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Center for Longitudinal Studies. Millennium Cohort Study (MCS). 2010. Available online: http://www.cls.ioe.ac.uk/studies.asp?sectionZ000100020001 (accessed on 11 July 2017).
- Blake-Lamb, T.L.; Locks, L.M.; Perkins, M.E.; Woo Baidal, J.A.; Cheng, E.R.; Taveras, E.M. Interventions for childhood obesity in the first 1000 days: A systematic review. Am. J. Prev. Med. 2016, 50, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Woo Baidal, J.A.; Cheng, E.R.; Blake-Lamb, T.L.; Perkins, M.; Taveras, E.M. Risk factors for childhood obesity in the first 1000 days: A systematic review. Am. J. Prev. Med. 2016, 50, 761–779. [Google Scholar] [CrossRef] [PubMed]
- Feeding Guidelines for Infant and Young Toddlers: A Responsive Parenting Approach. Available online: http://healthyeatingresearch.org/research/feeding-guidelines-for-infants-and-young-toddlers-a-responsive-parenting-approach/ (accessed on 11 August 2017).
- Waters, E.; de Silva-Sanigorski, A.; Hall, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2011, 3. [Google Scholar] [CrossRef]
- Ciampa, P.J.; Kumar, D.; Barkin, S.L.; Sanders, L.M.; Yin, H.S.; Perrin, E.M.; Rothman, R.L. Interventions aimed at decreasing obesity in children younger than 2 years: A systematic review. Arch. Pediatr. Adolesc. Med. 2010, 164, 1098–1104. [Google Scholar] [CrossRef] [PubMed]
- Laws, R.; Campbell, K.J.; van der Pligt, P.; Russell, G.; Ball, K.; Lynch, J.; Crawford, D.; Taylor, R.; Askew, D.; Denney-Wilson, E. The impact of interventions to prevent obesity or improve obesity related behaviours in children (0–5 years) from socioeconomically disadvantaged and/or indigenous families: A systematic review. BMC Public Health 2014, 14, 779. [Google Scholar] [CrossRef] [PubMed]
- Redsell, S.A.; Edmonds, B.; Swift, J.A.; Siriwardena, A.N.; Weng, S.; Nathan, D.; Glazebrook, C. Systematic review of randomized controlled trials of interventions that aim to reduce the risk, either directly or indirectly, of overweight and obesity in infancy and early childhood. Matern. Child Nutr. 2016, 12, 24–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mennella, J.A. Ontogeny of taste preferences: Basic biology and implication for health. Am. J. Clin. Nutr. 2014, 99, S704–S711. [Google Scholar] [CrossRef] [PubMed]
- Gianni, M.L.; Orsi, A.; Amato, O.; Piemontese, P.; Liotto, N.; Morlacchi, L.; Mosca, F. Implementation of nutrition strategies decreases post-natal growth restriction in preterm infants. PLoS ONE 2012, 7, e51166. [Google Scholar] [CrossRef]
- Navarro, J.I.; Sigulem, D.M.; Ferraro, A.A.; Polanco, J.J.; Barros, A.J. The double task of preventing malnutrition and overweight: A quasi-experimental community-based trial. BMC Public Health 2013, 13, 212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linares, J.; Corvalan, C.; Galleguillos, B.; Kain, J.; Gonzalez, L.; Uauy, R.; Garmendia, M.L.; Mericq, V. The effects of pre-pregnanacy BMI and maternal factors on the timing of adiposity rebound in offspring. Obesity 2016, 24, 1313–1319. [Google Scholar] [CrossRef] [PubMed]
- Ganu, R.S.; Harris, R.A.; Collins, K.; Aagaard, K.M. Maternal diet. A modulator for epigenomic regulation during development in non human primates and humans. Int. J. Obes. 2012, 2, S14–S18. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, F.; Parker, M.G.; Luo, Z.-C.; Wang, X.; Zhang, H.-J.; Wang, X.; Gillman, M.W.; Zhang, J. Maternal BMI, gestational diabetes, and weight gain in relation to childhood obesity: The mediation of placental weight. Obesity 2016, 24, 938–946. [Google Scholar] [CrossRef] [PubMed]
- Yampolsky, M.; Salafia, C.M.; Shlakter, O.; Haas, D.; Eucker, B.; Thorp, J. Modeling the variability of shapes of a human placenta. Placenta 2008, 29, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Hindmarsh, P.C.; Geary, M.P.; Rodeck, C.H.; Kingdom, J.C.; Cole, T.J. Factors predicting ante- and dpost-natal growth. Pediatr. Res. 2008, 63, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Mayhew, T.M.; Ohadike, C.; Baker, P.N.; Crocker, I.P.; Mitchell, C.; Ong, S.S. Stereological investigation of placental morphology in pregnancies complicated by pre-eclampsia with and without intrauterine growth restriction. Placenta 2003, 24, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Hivert, M.F.; Rifas-Shiman, S.L.; Gillman, M.W.; Oken, E. Greater early and mid-pregnancy gestational weight gains are associated with excess adiposity in mid-childhood. Obesity 2016, 24, 1546–1553. [Google Scholar] [CrossRef] [PubMed]
- Hinkle, S.N.; Schieve, L.A.; Stein, A.D.; Swan, D.W.; Ramakrishnan, U.; Sharma, A.J. Association between maternal prepregnancy body mass index and child neurodevelopment at 2 years of age. Int. J. Obes. 2012, 36, 1312–1319. [Google Scholar] [CrossRef] [PubMed]
- Hinkle, S.N.; Sharma, A.J.; Kim, S.Y.; Schieve, L.A. Maternal prepregnancy weight status and associations with children’ development and disabilities at kindergarten. Int. J. Obes. 2013, 37, 1344–1351. [Google Scholar] [CrossRef] [PubMed]
- Bilbo, S.D.; Schwarz, J.M. Early-life programming of later-life brain and behavior: A critical role for the immune system. Front. Behav. Neurosci. 2009, 3, 14. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, A.L.B.; Kaar, J.L.; Crune, T.L.; Starling, A.P.; Siega-Riz, A.M.; Ringham, B.M.; Glueck, D.H.; Noris, J.M.; Barbour, L.A.; Friedman, J.E.; et al. Maternal diet quality in pregnancy and neonatal adiposity: The Healthy Start Study. Int. J. Obes. 2016, 40, 1056–1062. [Google Scholar] [CrossRef] [PubMed]
- Fields, D.A.; Demerath, E.W.; Pietrobelli, A.; Chandler-Laney, P.C. Body composition at 6 months of life: Comparison of air displacement plethysmography and dual-energy X-ray absorptiometry. Obesity 2012, 20, 2302–2306. [Google Scholar] [CrossRef] [PubMed]
- Aris, I.M.; Bernard, J.Y.; Chen, L.W.; Tint, M.T.; Pang, W.W.; Soh, S.E.; Saw, S.M.; Shek, L.P.; Godfrey, K.M.; Gluckman, P.D.; et al. Modifiable risk factor in the first 1000 days for subsequent risk of childhood overweight in an Asian cohort: Significance of parental overweight status. Int. J. Obes. 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- Li, H.T.; Zhou, Y.B.; Liu, J.M. The impact of cesarean section on offspring overweight and obesity: A systematic review and meta-analysis. Int. J. Obes. 2013, 37, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Gaskins, A.J.; Blaine, A.I.; Zhang, C.; Gillman, M.W.; Missmer, S.A.; Field, A.E.; Chavarro, J.E. Association between cesarean birth and risk of obesity in offspring in childhood, adolescence, and early adulthood. JAMA Pediatr. 2016, 170, e162385. [Google Scholar] [CrossRef] [PubMed]
- Huxley, R.; Neil, A.; Collins, R. Unraveling the fetal origins hypothesis: Is there really an inverse association between birth weight and subsequent blood pressure? Lancet 2002, 360, 659–665. [Google Scholar] [CrossRef]
- Lawlor, D.A.; Ronalds, G.; Clark, H.; Smith, G.D.; Leon, D.A. Birth weight is inversely associated with incident coronary heart disease and stroke among individual born in 1950s: Findings from the Aberdeen children of the 1950s prospective cohort study. Circulation 2005, 112, 1414–1418. [Google Scholar] [CrossRef] [PubMed]
- Rorley, R. Fetal origins of adult disease. Semin. Fetal Neonatal Med. 2006, 11, 73–78. [Google Scholar]
- Berni Canani, R.; di Costanzo, M.; Leone, L.; Bedogni, G.; Brambilla, P.; Cianfarani, S.; Nobili, V.; Pietrobelli, A.; Agostoni, C. Epigenetic mechanisms elicited by nutrition in early life. Nutr. Res. Rev. 2011, 24, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Simmons, R. Epigenetics and maternal nutrition: Nature vs. nurture. Proc. Nutr. Soc. 2010, 70, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Fomon, S.J.; Haschke, F.; Ziegler, E.E.; Nelson, S.E. Body composition of reference children from birth to age 10 years. Am. J. Clin. Nutr. 1982, 35, 1169–1175. [Google Scholar] [PubMed]
- Forbes, G.B. Body composition in infancy, childhood and adolescence. In Human Body Composition: Growth, Aging, and Activity; Springer: New York, NY, USA, 1987; pp. 125–196. [Google Scholar]
- Taylor, R.W.; Heath, A.-L.M.; Galland, B.C.; Cameron, S.L.; Lawrence, J.A.; Gray, A.R.; Tannock, G.W.; Lawley, B.; Haeley, D.; Sayers, R.M.; et al. Three-year follow-up of a randomized controlled trial to reduce excessive weight gain in the first two years of life: Protocol for the POI follow-up study. BMC Public Health 2016, 16, 771. [Google Scholar] [CrossRef] [PubMed]
- Toro-Ramos, T.; Paley, C.; Pi-Sunyer, F.X.; Gallagher, D. Body composition during fetal development and infancy through the age of 5 years. Eur. J. Clin. Nutr. 2015, 69, 1279–1289. [Google Scholar] [CrossRef] [PubMed]
- Fields, D.A.; Gilchrist, J.M.; Catalano, P.M.; Gianni, M.L.; Roggero, P.M.; Mosca, F. Longitudinal body composition data in exclusively breast-fed infants: A multicentre study. Obesity 2011, 19, 1887–1891. [Google Scholar] [CrossRef] [PubMed]
- Jordan, P.N.; Hall, K.D. Dynamic coordination of macronutrient balance during infant growth: Insights from mathematical model. Am. J. Clin. Nutr. 2008, 87, 692–703. [Google Scholar] [PubMed]
- Gishti, O.; Gaillard, R.; Manniesing, R.; Abrahamse-Berkeveld, M.; van der Beek, E.M.; Heppe, D.H.; Steegers, E.A.; Hofman, A.; Duijts, L.; Durmus, B.; et al. Fetal and infant growth patterns associated with total and abdominal fat distribution in school-age children. J. Clin. Endocrinol. Metab. 2014, 99, 2557–2566. [Google Scholar] [CrossRef] [PubMed]
- Heppe, D.H.; Kiefte-de Jong, J.C.; Durmus, B. Parental, fetal, and infant risk factors for preschool overweight: The generation R study. Pediatr. Res. 2013, 73, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Crume, T.L.; Ogden, L.; Maligie, M.; Sheffield, S.; Bischoff, K.J.; McDuffie, R.; Daniels, S.; Hamman, R.F.; Norris, J.M.; Dabelea, D. Long-term impact of neonatal breastfeeding on childhood adiposity and fat distribution among children exposed to diabetes in utero. Diabetes Care 2011, 34, 641–645. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Liu, L.; Zhu, Y.; Huamìng, G.; Wang, P.P. The association between breastfeeding and childhood obesity: A meta-analysis. BMC Public Health 2014, 14, 1267. [Google Scholar] [CrossRef] [PubMed]
- Horta, B.L.; Victoria, C.G. Long-Term Effects of Breastfeeding: A Systematic Review; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Kalliomaki, M.; Collado, M.C.; Salminen, S.; Isolauri, E. Early differences in fecal microbiota composition in children may predict overweight. Am. J. Clin. Nutr. 2008, 87, 534–538. [Google Scholar] [PubMed]
- Horta, B.L.; de Mola, C.L.; Victoria, C.G. Long term consequences of breastfeeding on cholesterol, obesity, systolic blood pressure and type two diabetes: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Harder, T.; Bergmann, R.; Kallischnigg, G.; Plagemann, A. Duration of breastfeeding and risk of overweight: A meta-analysis. Am. J. Epidemiol. 2005, 162, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B. Marketing of dietetic products for infants and young children in Europe three decades after adoption of the international code of marketing of breast milk-substitutes. Ann. Nutr. Metab. 2011, 59, 70–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lefebvre, C.M.; John, R.M. The effect of breastfeeding on childhood overweight and obesity: A systematic review of the literature. J. Am. Assoc. Nurse Pract. 2014, 26, 386–401. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Complementary Feeding: Report of the Global Consultation; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Pearce, J.; Langly-Evans, S.C. The types of food and feeding style introduced during complementary feeding and risk of childhood obesity: A systematic review. Int. J. Obes. 2013, 37, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Pearce, J.; Taylor, M.A.; Langley-Evans, S.C. Timing of the introduction of complementary feeding and risk of childhood obesity: A systematic review. Int. J. Obes. 2013, 37, 1295–1306. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wu, Y.; Xiong, G.; Chao, T.; Jin, Q.; Liu, R.; Hao, L.; Wei, S.; Yang, N.; Yang, X. Introduction of complementary feeding before 4 months of age increases the risk of childhood overweight or obesity: A meta-analysis of prospective cohort studies. Nutr. Res. 2016, 36, 759–770. [Google Scholar] [CrossRef] [PubMed]
- Qasem, W.; Fenton, T.; Friel, J. Age of introduction of first complementary feeding for infants: A systematic review. BMC Pediatr. 2015, 15, 107. [Google Scholar] [CrossRef] [PubMed]
- Huh, S.Y.; Rifas-Shiman, S.L.; Taveras, E.M.; Oken, E.; Gillman, M.W. Timing of solid food introduction and risk of obesity in preschool-aged children. Pediatrics 2011, 127, e544–e551. [Google Scholar] [CrossRef] [PubMed]
- Faith, M.S.; Heshka, S.; Keller, K.; Sherry, B.; Matz, P.E.; Pietrobelli, A.; Allison, D.B. Maternal-child feeding patterns and child body weight: Finding from a population-based sample. Arch. Pediatr. Adolesc. Med. 2003, 157, 926–932. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.M.; Henderson, M.S.; Tripicchio, G.; Rozin, P.; Heo, M.; Pietrobelli, A.; Berkowitz, R.I.; Keller, K.L.; Faith, M.S. Observed parent-child feeding dynamics in relation to child body mass index and adiposity. Pediatr. Obes. 2017. [Google Scholar] [CrossRef] [PubMed]
- Ashman, A.M.; Collins, C.E.; Hure, A.J.; Jensen, M.; Oldmeadow, C. Maternal diet during early childhood, but not pregnancy, predicts diet quality and fruit and vegetable acceptance in offspring. Matern. Child Nutr. 2016, 12, 579–590. [Google Scholar] [CrossRef] [PubMed]
- Mennella, J.A.; Reiter, A.R.; Daniles, L.M. Vegetable and fruit acceptance during infancy: Impact of ontogeny, genetics, and early experiences. Adv. Nutr. 2016, 7, 211S–219S. [Google Scholar] [CrossRef] [PubMed]
- Faith, M.S.; Dennison, B.A.; Edmunds, L.S.; Stratton, H. Fruit juice intake predicts increased adiposity gain children from low-income families: Weight status-by-environment interaction. Pediatrics 2006, 118, 2066–2075. [Google Scholar] [CrossRef] [PubMed]
- Silva Garcia, K.; Power, T.G.; Fisher, J.O.; O’Connor, T.M.; Hughes, S.O. Latina mothers’ influences on child appetite regulation. Appetite 2016, 103, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Faith, M.S.; Rose, E.; Matz, P.E.; Pietrobelli, A.; Epstein, L.H. Co-twin control design for testing behavioral economic theories of child nutrition: Methodological note. Int. J. Obes. 2006, 30, 1501–1505. [Google Scholar] [CrossRef] [PubMed]
- Powell, E.M.; Frankel, L.A.; Hernandez, D.C. The mediating role of child self-regulation of eating in the relationship between parental use of food as a reward and child emotional overeating. Appetite 2017, 113, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Luque, V.; Closa-monasterolo, R.; Escribano, J.; Ferrè, N. Early programming by protein intake: The effect of protein on adiposity development and the growth and functionality of vital organs. Nutr. Metab. Insights 2015, 8, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Haschke, F.; Grathwohl, D.; Detzel, P.; Steenhout, P.; Wagemans, N.; Erdmann, P. Postnatal high protein intake can contribute to accelerated wirht gaij of infants and increased obesity risk. In Preventive Aspects of Early Nutrition; Fewtrell, M.S., Haschke, F., Prescott, S.L., Eds.; Nestlè Nutrition Institute Workshop Series; Nestlè Ltd.: Vevey, Switzerland; S. Karger AG: Basel, Switzerland, 2016; Volume 85, pp. 101–109. [Google Scholar]
- Mennella, J.A.; Trabulsi, J.C.; Papas, M.A. Effects of cow milk versus extensive protein hydrolysate formulas on infant cognitive development. Amino Acids 2016, 48, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Braun, K.V.; Erler, N.S.; Kiefte-de Jong, J.C.; Jaddoe, V.W.; van den Hooven, E.H.; Franco, O.H.; Voortman, T. Dietary intake of protein in early childhood is associated with growth trajectories between 1 and 9 years of age. J. Nutr. 2016, 146, 2361–2367. [Google Scholar] [CrossRef] [PubMed]
- Eussen, S.R.; Pean, J.; Oliver, L.; Delaere, F.; Lluch, A. Theoretical impact of replacing whole cow’s milk by young-child formula on nutrient intakes of UK young children: Results of a simulation study. Ann. Nutr. Metab. 2015, 67, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Hauner, H.; Brunner, S.; Amann-Gassner, U. The role of dietary fatty acids for early human adipose tissue growth. Am. J. Clin. Nutr. 2013, 98, 549S–555S. [Google Scholar] [CrossRef] [PubMed]
- Hauner, H.; Much, D.; Vollhardt, C.; Brunner, S.; Schmid, D.; Sedlmeier, E.M.; Heimberg, E.; Schuster, T.; Zimmermann, A.; Schneider, K.-T.M. Effect of reducing the n-6/n-3 long-chain polyunsatured fatty acid (LCPUFA) ratio during pregnancy and lactation on infant adipose tissue growth within the first year of life (INFAT-study): An open label, randomized, control trial. Am. J. Clin. Nutr. 2012, 95, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Rodolph, M.C.; Young, B.E.; Lemas, D.J.; Palmer, C.E.; Hernandez, T.L.; Barbour, L.A.; Friedman, J.E.; Krebs, N.F.; MacLean, P.S. Early infant adipose deposition is positively associated with the n-6 to n-3 fatty acid ratio in human milk independent of maternal BMI. Int. J. Obes. 2017, 41, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Hurtado, J.A.; Iznaola, C.; Pena, M.; Ruiz, J.; Pena-Quintana, L.; Kajarabille, N.; Rodriguez-Santana, Y.; Sanjurjo, P.; Aldàmiz-Echevarrià, L.; Ochoa, J.; et al. Effects of maternal omega-3 supplementation on fatty acids and on visual and cognitive development. J. Pediatr. Gastroenterol. Nutr. 2015, 61, 472–480. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.; McDougald, D.M.; Steiner-Asiedu, M. Dietary trans fatty acid intake and maternal diet and infant adiposity. Eur. J. Clin. Nutr. 2010, 64, 1308–1315. [Google Scholar] [CrossRef] [PubMed]
- Michaelsen, K.F.; Larnkjaer, A.; Molgaard, C. Early diet, insulin-like growth factor-1, growth and later adiposity. World Rev. Nutr. Diet. 2013, 106, 113–118. [Google Scholar] [PubMed]
- Nguyen, P.K.; Lin, S.; Heidenreich, P. A systematic comparison of sugar content in low-fat vs. regular version of food. Nutr. Diabetes 2016, 6, e193. [Google Scholar] [CrossRef] [PubMed]
- Domingues-Montanari, S. Clinical and psychological effects of excessive screen time on children. J. Pediatr. Child Health 2017, 53, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Barlow, S.E.; Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007, 120, S164–S192. [Google Scholar] [CrossRef] [PubMed]
- Spear, B.A.; Barlow, S.E.; Ervin, C.; Ludwig, D.S.; Saelens, B.E.; Schetzina, K.E.; Taveras, E.M. Recommendations for treatment of child and adolescent overweight and obesity. Pediatrics 2007, 120, S254–S288. [Google Scholar] [CrossRef] [PubMed]
- Tripicchio, G.; Heo, M.; Diewald, L.; Noar, S.M.; Dooley, R.; Pietrobelli, A.; Burger, K.S.; Faith, M.S. Restricting advertisements for high-fat, high-sugar foods during children’s television programs: Attitudes in a U.S. population-based sample. Child. Obes. 2016, 12, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, A.C.; Greaney, M.L.; Wallington, S.F.; Mesa, T.; Salas, C.F. A review of early influences on physical activity and sedentary behaviors of preschool-age children in high-income countries. J. Spec. Pediatr. Nurs. 2017. [Google Scholar] [CrossRef] [PubMed]
- Saunders, T.J.; Gray, C.E.; Poitras, V.J.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Olds, T. Combinations of physical activity, sedentary behavior and sleep: Relationship with health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; Carson, V.; Grey, C.E.; Tremblay, M.S. Importance of all movement behaviors in a 24 h period for overall health. Int. J. Environ. Res. Public Health 2014, 11, 12575–12581. [Google Scholar] [CrossRef] [PubMed]
- National Sleep Foundation. Sleep in America Poll; National Sleep Foundation: Washington, DC, USA, 2006. [Google Scholar]
- Petrov, M.E.; Vander Wyst, K.B.; Whisner, C.M.; Jeong, M.; Denniston, M.; Moramarco, M.W.; Gallagher, M.R.; Reifsnider, E. Relationship of sleep duration and regularity with dietary intake among preschool aged children with obesity from low-income families. J. Dev. Behav. Pediatr. 2017, 38, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.; McDonald, L.; van Jaarsveld, C.H.; Llewellyn, C.; Fildes, A.; Schremptf, S.; Wardle, J. Sleep and energy intake in early childhood. Int. J. Obes. 2014, 38, 926–929. [Google Scholar] [CrossRef] [PubMed]
- Hansen, S.; Halldorsson, T.I.; Olsen, S.F.; Rytter, D.; Bech, B.H.; Granstrom, C.; Henriksen, T.B.; Chavarro, J.E. Birth by cesarean cection in relation to adult offspring overweight and biomarkers of cardiometabolic risk. Int. J. Obes. 2017. [Google Scholar] [CrossRef]
- Oddy, W.H.; Mori, T.A.; Huag, R.C.; Marsh, J.A.; Pennell, C.E.; Chivers, P.T.; Hands, B.P.; Jacoby, P.; Rzehak, P.; Koletzko, B.V.; et al. Early infant feeding and adiposity risk: From infancy to adulthood. Ann. Nutr. Metab. 2014, 64, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Taveras, E.M.; Rifas-Shiman, S.L.; Oken, E.; Gunderson, E.P.; Gillman, M.W. Short sleep duration in infancy and risk of childhood overweight. Arch. Adolesc. Med. 2008, 162, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Collings, P.J.; Brage, S.; Bingham, D.B.; Costa, S.; West, J.; McEachan, R.R.C.; Wright, J.; Barber, S.E. Physical activity, sedentary time, and fatness in a Biethnic sample of young children. Med. Sci. Sports Exerc. 2017, 49, 930–938. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Practice | List | Reference |
|---|---|---|
| Practice 1 | Both mother and father nutritional behavior matter | [6,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33] |
| Practice 2 | Systematize body composition measurements to monitor growth | [34,35,36,37,38,39,40,41] |
| Practice 3 | Exclusive breastfeeding for the best start in life | [42,43,44,45,46,47,48] |
| Practice 4 | Window to introduce complementary feeding | [49,50,52,53,54,55] |
| Practice 5 | Fruits and vegetables liking begins early | [7,8,9,12,32,49,52,56,57,58,59,60] |
| Practice 6 | Respect the child appetite | [56,61,62,63] |
| Practice 7 | Limit animal protein intake | [64,65,66,67] |
| Practice 8 | Promote qualitative and adequate fat intake | [69,70,71,72,73,74] |
| Practice 9 | Parents be a role model | [56,57,58,77,78,79] |
| Practice 10 | Promoting physical activity and good sleep | [80,81,82,83,84,85] |
| Behaviors Interrelate | Overweight and Obesity Risk | References |
|---|---|---|
| Parental overweight status | ||
| Maternal | 95% CI: 9.8–13.8 | |
| Paternal | 95% CI: 9.6–11.6 | [28] |
| Cesarean delivery | 95% CI: 1.10–4.27 (OR = 2.17) | [88] |
| Early infant feeding | ||
| Longer breastfeeding—1 year | Beta = −0.027, p < 0.001 | |
| 3 years | 95% CI: 1.43–2.94, p < 0.001 | [89] |
| 20 years | 95% CI: 1.12–1.93, p = 0.005 | |
| Short sleep duration in infancy | Beta = 0.16, 95% CI: 0.02–0.29 | [90] |
| Physical activity | ||
| Sedentary time | Beta = 0.042, 95% CI: −0.037 to 0.12 | [91] |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pietrobelli, A.; Agosti, M.; The MeNu Group. Nutrition in the First 1000 Days: Ten Practices to Minimize Obesity Emerging from Published Science. Int. J. Environ. Res. Public Health 2017, 14, 1491. https://doi.org/10.3390/ijerph14121491
Pietrobelli A, Agosti M, The MeNu Group. Nutrition in the First 1000 Days: Ten Practices to Minimize Obesity Emerging from Published Science. International Journal of Environmental Research and Public Health. 2017; 14(12):1491. https://doi.org/10.3390/ijerph14121491
Chicago/Turabian StylePietrobelli, Angelo, Massimo Agosti, and The MeNu Group. 2017. "Nutrition in the First 1000 Days: Ten Practices to Minimize Obesity Emerging from Published Science" International Journal of Environmental Research and Public Health 14, no. 12: 1491. https://doi.org/10.3390/ijerph14121491
APA StylePietrobelli, A., Agosti, M., & The MeNu Group. (2017). Nutrition in the First 1000 Days: Ten Practices to Minimize Obesity Emerging from Published Science. International Journal of Environmental Research and Public Health, 14(12), 1491. https://doi.org/10.3390/ijerph14121491