A Cluster Randomized Trial to Promote Healthy Menu Items for Children: The Kids’ Choice Restaurant Program

Abstract
:1. Introduction
1.1. Diet, Obesity and the Restaurant Food Environment
1.2. Evidence for Promoting Healthy Menu Items to Children and Families
1.3. Present Study
2. Materials and Methods
2.1. Study Design and Setting
2.2. Restaurant and Manager Recruitment and Allocation to Condition
2.3. Intervention Description
2.3.1. Theoretical Framework
2.3.2. Intervention Conditions
2.3.3. Implementation
2.4. Evaluation Protocol and Measures
2.4.1. Process Evaluation-Intervention Implementation
2.4.2. Short-Term Efficacy-Sales of New and Existing Child Menu Items
2.4.3. Manager Interview
2.5. Statistical Analyses
3. Results
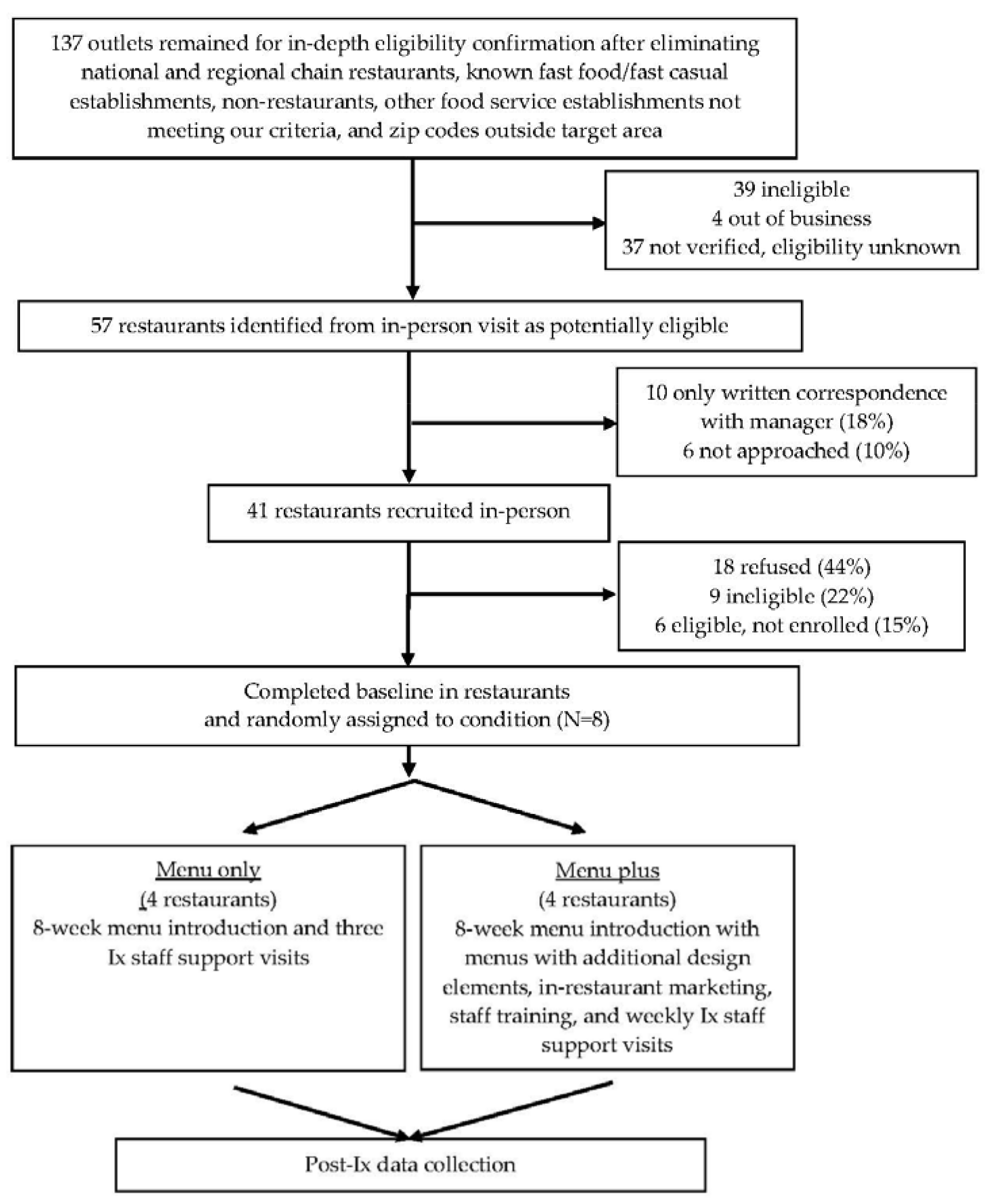
3.1. Recruitment and Retention of Restaurants
3.2. Restaurant Characteristics
3.3. Intervention Implementation
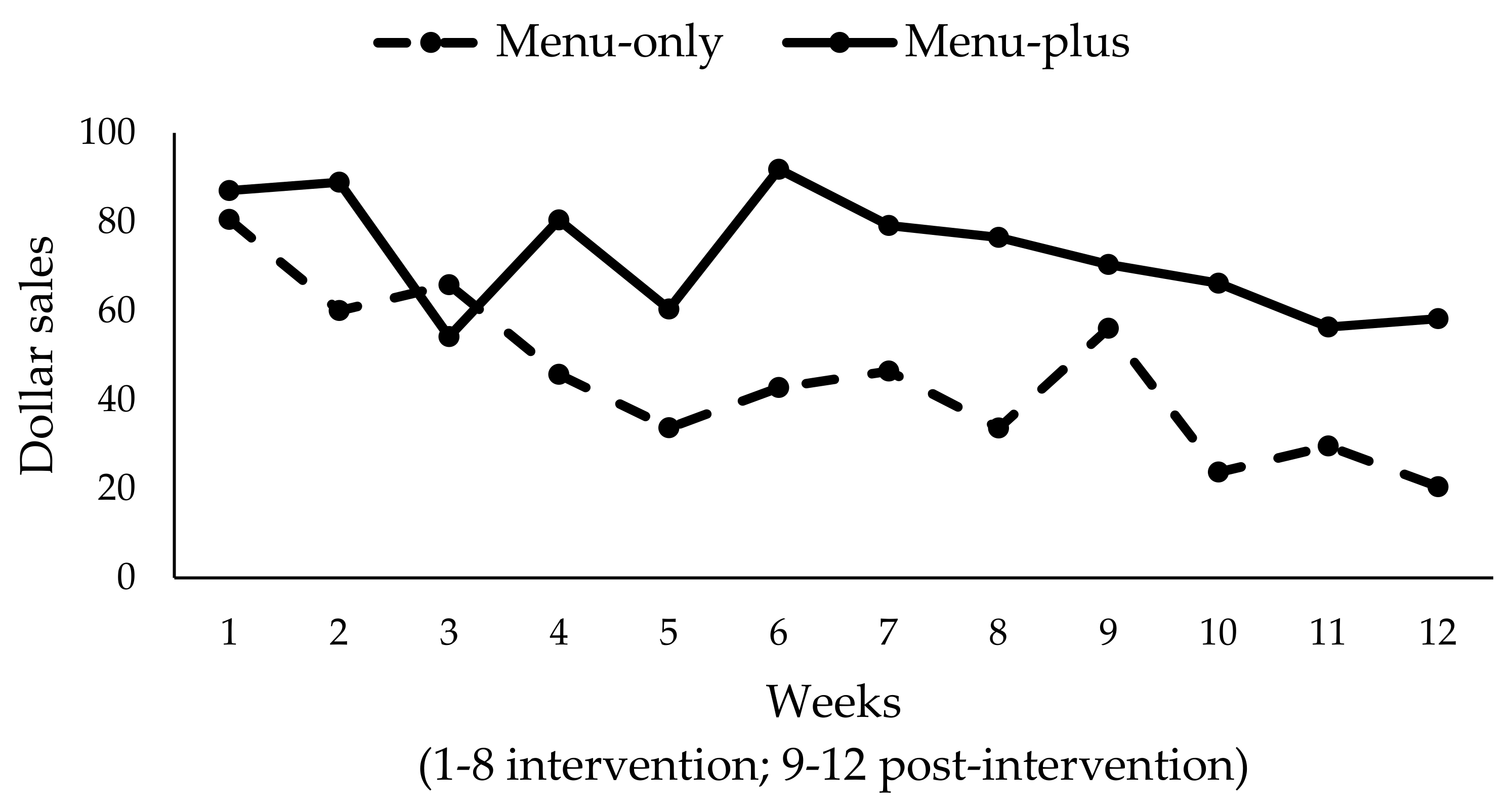
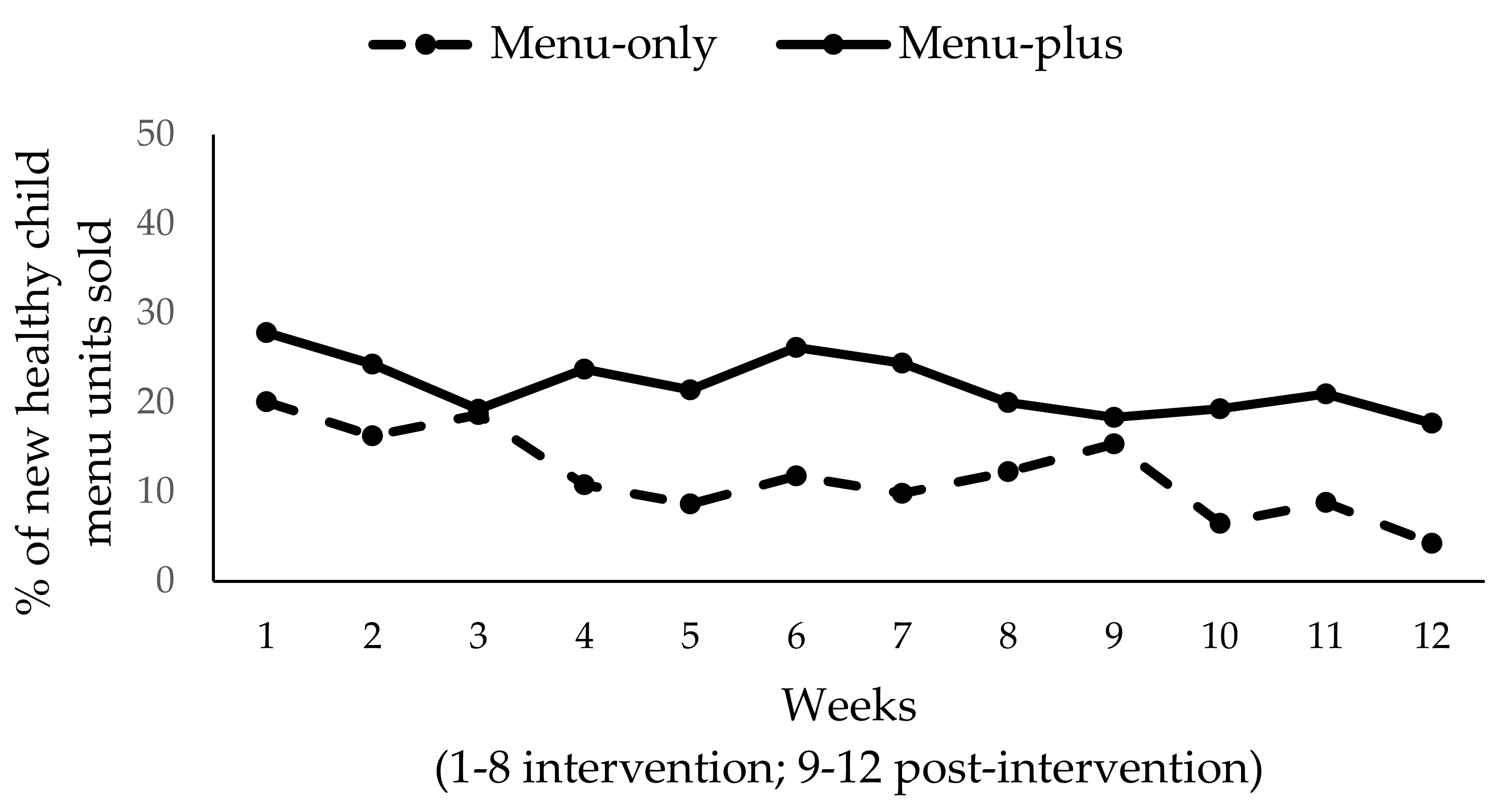
3.4. Primary Outcome Evaluation: Short-Term Efficacy on Sales of New Healthy Child Menu Items
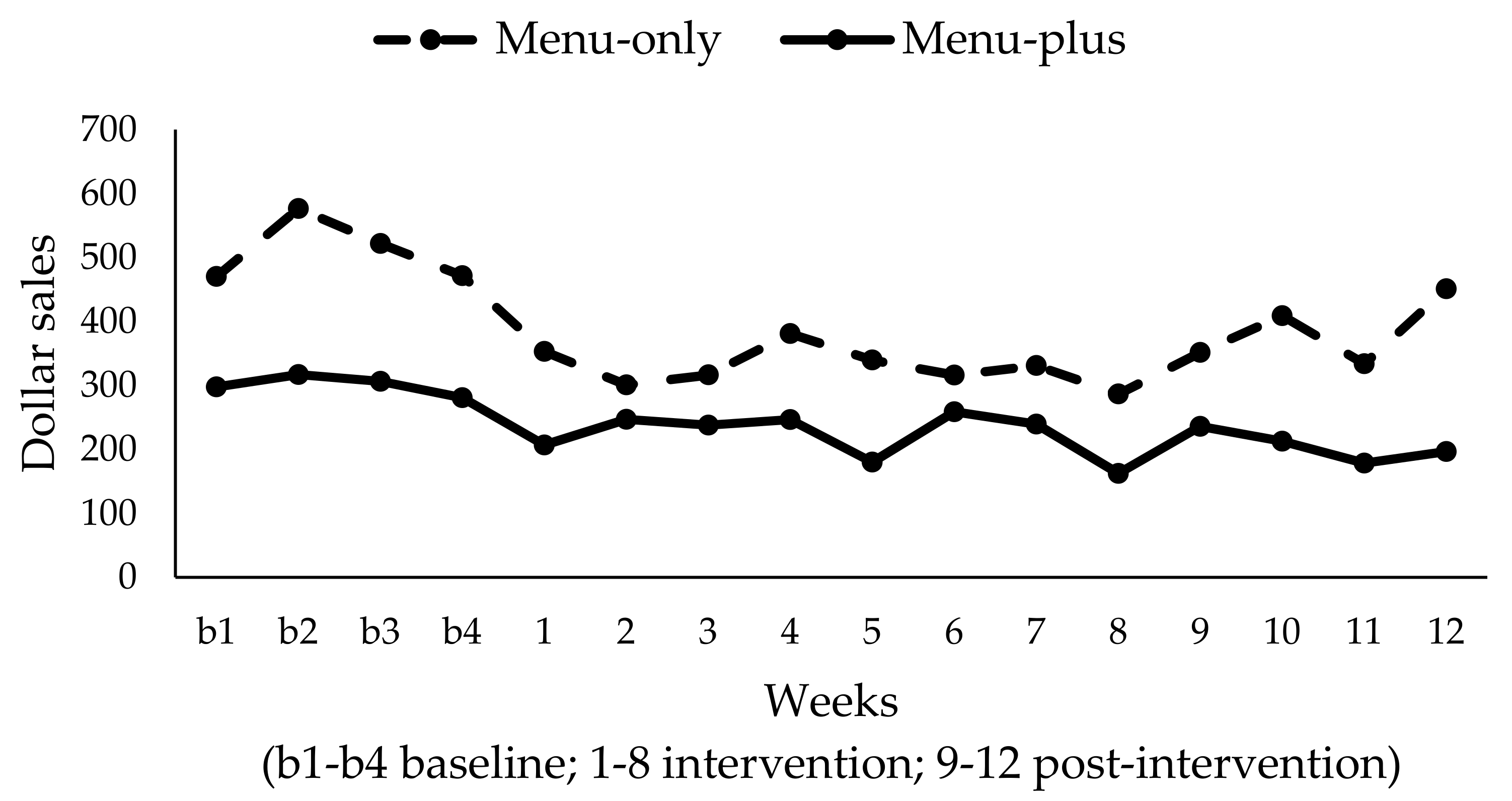
3.5. Secondary Outcome Evaluation: Short-Term Efficacy on Sales of Existing Child Menu Items
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Poti, J.M.; Popkin, B.M. Trends in energy intake among U.S. children by eating location and food source, 1977–2006. J. Am. Diet. Assoc. 2011, 111, 1156–1164. [Google Scholar] [CrossRef] [PubMed]
- Bowen, D.J.; Barrington, W.E.; Beresford, S.A. Identifying the effects of environmental and policy change interventions on healthy eating. Annu. Rev. Public Health 2015, 36, 289–306. [Google Scholar] [CrossRef] [PubMed]
- Rose, D.; Nicholas Bodor, J.; Hutchinson, P.L.; Swalm, C.M. The importance of a multi-dimensional approach for studying the links between food access and consumption. J. Nutr. 2010, 140, 1170–1174. [Google Scholar] [CrossRef] [PubMed]
- Lytle, L.A.; Sokol, R.L. Measures of the food environment: A systematic review of the field, 2007–2015. Health Place 2017, 44, 18–34. [Google Scholar] [CrossRef] [PubMed]
- Odoms-Young, A.M.; Zenk, S.N.; Karpyn, A.; Ayala, G.X.; Gittelsohn, J. Obesity and the food environment among minority groups. Curr. Obes. Rep. 2012, 1, 141–151. [Google Scholar] [CrossRef]
- Valdivia Espino, J.N.; Guerrero, N.; Rhoads, N.; Simon, N.-J.; Escaron, A.L.; Meinen, A.; Javier Nieto, F.; Martinez-Donate, A.P. Community-based restaurant interventions to promote healthy eating: A systematic review. Prev. Chronic Dis. 2015, 12. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.A.; Babey, S.H. Contextual influences on eating behaviours: Heuristic processing and dietary choices. Obes. Rev. 2012, 13, 766–779. [Google Scholar] [CrossRef] [PubMed]
- Sliwa, S.; Anzman-Frasca, S.; Lynskey, V.; Washburn, K.; Economos, C. Assessing the availability of healthier children’s meals at leading quick-service and full-service restaurants. J. Nutr. Educ. Behav. 2016, 48, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Ayala, G.X.; Ibarra, L.; Binggeli-Vallarta, A.; Moody, J.; McKenzie, T.L.; Angulo, J.; Hoyt, H.; Chuang, E.; Ganiats, T.G.; Gahagan, S.; et al. Our choice/nuestra opción: The imperial county, California childhood obesity research demonstration study (CA-CORD). Child. Obes. 2015, 11, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Ayala, G.X.; Castro, I.A.; Pickrel, J.L.; Wiliams, C.B.; Lin, S.-F.; Madanat, H.; Jun, H.-J.; Zive, M. A restaurant-based intervention to promote sales of healthy children’s menu items: The kids’ choice restaurant program cluster randomized trial. BMC Public Health 2016, 16, 250. [Google Scholar] [CrossRef] [PubMed]
- Urban, L.E.; Weber, J.L.; Heyman, M.B.; Schichtl, R.L.; Verstraete, S.; Lowery, N.S.; Das, S.K.; Schleicher, M.M.; Rogers, G.; Economos, C.D.; et al. Energy contents of frequently ordered restaurant meals and comparison with human energy requirements and U.S. department of agriculture database information: A multisite randomized study. J. Acad. Nutr. Diet. 2016, 116, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Powell, L.M.; Nguyen, B.T. Fast-food and full-service restaurant consumption among children and adolescents: Effect on energy, beverage, and nutrient intake. JAMA Pediatr. 2013, 167, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Hillier-Brown, F.C.; Summerbell, C.D.; Moore, H.J.; Routen, A.; Lake, A.A.; White, M.; Arauji-Soares, V.; Abraham, C.; Adamson, A.J.; Brown, T.J. The impact of interventions to promote healthier ready-to-eat meals (to eat in, to take away or to be delivered) sold by specific food outlets open to the general public: A systematic review. Obes. Rev. 2017, 18, 227–246. [Google Scholar] [CrossRef] [PubMed]
- Hillier-Brown, F.C.; Moore, H.J.; Lake, A.A.; Adamson, A.J.; White, M.; Adams, J.; Arauji-Soares, V.; Abraham, C.; Summerbell, C.D. The effectiveness of interventions targeting specific out-of-home food outlets: Protocol for a systematic review. Syst. Rev. 2014, 3, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CHD Expert. CHD Expert Evaluates and Compares the Independent and Chain Restaurant Segments, Breaking Each Down with an Overview Around Full Service and Limited Service Restaurants 2015. Available online: https://www.chd-expert.com/blog/press_release/chd-expert-evaluates-and-compares-the-independent-and-chain-restaurant-segments-breaking-each-down-with-an-overview-around-full-service-and-limited-service-restaurants/ (accessed on 30 September 2015).
- Ogden, C.L.; Caroll, M.D.; Fryar, C.D.; Flegal, K.M. Prevalence of Obesity among Adults and Youth: United States, 2011–2014; U.S. Department of Health and Human Services: Hyattsville, MD, USA, 2015.
- Cohen, D.; Bhatia, R.; Story, M.T.; Sugarman, S.D.; Wootan, M.; Economos, C.D.; Van Horn, L.; Whitsel, L.P.; Roberts, S.; Powell, L.M.; et al. Performance Standards for Restaurants: A New Approach to Addressing the Obesity Epidemic; RAND Corporation: Santa Monica, CA, USA, 2013. [Google Scholar]
- Glanz, K.; Resnicow, K.; Seymour, J.S.; Hoy, K.; Stewart, H.; Lyons, M.; Goldberg, J. How major restaurant chains plan their menus: The role of profit, demand, and health. Am. J. Prev. Med. 2007, 32, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Crixell, S.H.; Friedman, B.; Fisher, D.T.; Biediger-Friedman, L. Improving children’s menus in community restaurants: Best food for families, infants, and toddlers (Best Food FITS) intervention, South Central Texas, 2010–2014. Prev. Chronic Dis. 2014, 11, 223. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau. Profile of General Population and Housing Characteristics: 2015 Demographic Profile Data; American Factfinder: San Diego, CA, USA, 2015.
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979; p. 352. [Google Scholar]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Cohen, D.A.; Scribner, R.A.; Farley, T.A. A structural model of health behavior: A pragmatic approach to explain and influence health behaviors at the population level. Prev. Med. 2000, 30, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.A.; Story, M. Mitigating the health risks of dining out: The need for standardized portion sizes in restaurants. Am. J. Public Health 2014, 104, 586–590. [Google Scholar] [CrossRef] [PubMed]
- Anzman-Frasca, S.; Muller, M.P.; Sliwa, S.; Dolan, P.R.; Harelick, L.; Roberts, S.B.; Washburn, K.; Economos, C.D. Changes in children’s meal orders following healthy menu modifications at a regional U.S. restaurant chain. Obes. Soc. 2015, 23, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, B.; Caliskan, O. A review of literature on restaurant menus: Specifying the managerial issues. Int. J. Gastron. Food Sci. 2014, 2, 3–13. [Google Scholar] [CrossRef]
- Castro, I.A.; Williams, C.B.; Madanat, H.; Jun, H.J.; Zive, M.; Gahagan, S.; Ayala, G.X. Food ordering for children in restaurants: Multiple sources of influence on decision making. Public Health Nutr. 2016, 19, 2404–2409. [Google Scholar] [CrossRef] [PubMed]
- About National Restaurant Association. Available online: http://www.restaurant.org/Industry-Impact/Food-Healthy-Living/Kids-LiveWell/About#faq#4 (accessed on 15 September 2015).
- Food Processor Diet Analysis Software 2014. Available online: https://www.esha.com/products/food-processor-nutrition-analysis-software/ (accessed on 30 March 2016).
- Wansink, B.; van Ittersum, K. Portion size me: Plate-size induced consumption norms and win-win solutions for reducing food intake and waste. J. Exp. Psychol. Appl. 2013, 19, 320–332. [Google Scholar] [CrossRef] [PubMed]
- Anzman-Frasca, S.; Muller, M.P.; Lynskey, V.M.; Harelick, L.; Economos, C.D. Orders of Healthier Children’s Items Remain High More Than Two Years after Menu Changes at A Regional Restaurant Chain. Health Aff. (Millwood) 2015, 34, 1885–1892. [Google Scholar] [CrossRef] [PubMed]
- Wansink, B.; Love, K. Slim by design: Menu strategies for promoting high-margin, healthy foods. Int. J. Hosp. Manag. 2014, 42, 137–143. [Google Scholar] [CrossRef]
- Castro, I.A.; Calderon, J.; Ayala, G.X. Who is influencing whom? Latino parent–child request interactions and product purchases in food retail environments. Soc. Mark. Q. 2017, 23, 155–168. [Google Scholar] [CrossRef]
- Calderon, J.; Ayala, G.X.; Elder, J.P.; Belch, G.E.; Castro, I.A.; Weibel, N.; Pickrel, J. What Happens When Parents and Children Go Grocery Shopping? An Observational Study of Latino Dyads in Southern California, USA. Health Educ. Behav. 2016. [Google Scholar] [CrossRef] [PubMed]
- McGuffin, L.E.; Price, R.K.; McCaffrey, T.A.; Hall, G.; Lobo, A.; Wallace, J.M.; Livingstone, M.B. Parent and child perspectives on family out-of-home eating: A qualitative analysis. Public Health Nutr. 2015, 18, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Ayala, G.X.; Baquero, B.; Laraia, B.A.; Ji, M.; Linnan, L. Efficacy of a store-based environmental change intervention compared with a delayed treatment control condition on store customers’ intake of fruits and vegetables. Public Health Nutr. 2013, 16, 1953–1960. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.K.; Piaggio, G.; Elbourne, D.R.; Altman, D.G.; CONSORT Group. CONSORT 2010 statement: Extension to cluster randomised trials. BMJ 2012, 345, e5661. [Google Scholar] [CrossRef] [PubMed]
- Mueller, M.P.; Anzman-Frasca, S.; Blakeley, C.E.; Folta, S.C.; Wilde, P.; Economos, C.D. Ordering patterns following the implementation of a healthier children’s restaurant menu: A latent class analysis. Obesity 2017, 25, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Sosa, E.T.; Biediger-Friedman, L.; Banda, M. Associations between a voluntary restaurant menu designation initiative and patron purchasing behavior. Health Promot. Pract. 2014, 15, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Ragunathan, R.; Naylor, R.W.; Hoyer, W.D. The unhealthy = tasty intuition and its effects on taste inferences, enjoyment, and choice of food products. J. Mark. 2006, 70, 170–184. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Restaurant Characteristics | Overall | Menu-Only | Menu-Plus |
|---|---|---|---|
| Mean (SD) or Median (Range) or % (n) | |||
| Number of restaurants | N = 8 | n = 4 | n = 4 |
| Mean years in operation | 17.8 (15.0) | 17.8 (20.5) | 17.7 (10.3) |
| Mean number of full-time employees | 12.9 (6.6) | 11.8 (5.7) | 14.0 (8.2) |
| Mean number of part-time employees | 11.1 (11.5) | 12.3 (14.1) | 10.0 (10.4) |
| Mean number of tables | 33.0 (7.2) | 36.8 (4.5) | 29.3 (7.9) |
| Restaurants’ marketing in English only | 87.5% (7) | 75.0% (3) | 100% (4) |
| Restaurants with existing child menu | 75.0% (6) | 75.0% (3) | 75.0% (3) |
| Median of manager reported average weekly sales | $21,500 ($8000–60,000) | $16,000 ($8000–60,000) | $23,750 ($13,461–32,000) |
| Child Menu Characteristics | Menu-Only | Menu-Plus |
|---|---|---|
| Composition of existing menu (n = 6; 3 per condition) | ||
| Offer healthy sides | 33% (1) | 33% (1) |
| Existing beverage included | 66% (2) | 66% (2) |
| Price (average) | ||
| Existing child menu item 1 | $6.67 | $5.50 |
| New healthy child menu item 2 | $6.55 3 | $5.47 |
| Program Implementation | Planned Dose | Menu-Only (n = 4) Median (Range) | Menu-Plus (n = 4) Median (Range) |
|---|---|---|---|
| Number of healthy main entrees offered | 5 | 5 (5–6) | 5.5 (5–6) |
| Median % of supplied menus present across site visits per restaurant | 100% | 89.0% (70–92%) | 95.0% (91–100%) |
| Median % of tables displaying table tents across site visits per restaurant | 100% | NA | 65% (0–95%) |
| Median number of promotional signs always displayed across site visits per restaurant | 1 | NA | 1 (1–2) |
| Average minutes of kitchen manager/chef meetings | NA | 59.5 (37–80) | 62.0 (60–64) a |
| Dose Delivered | |||
| Average minutes of kitchen staff training | 15 | NA | 33.0 (5–49) b |
| Average % of topics covered in kitchen training c | 100% | NA | 87.5% (88–100%) |
| Average minutes of general wait staff d training | 15 | NA | 12.0 (0–19) |
| Average % of topics covered in general training c | 100% | NA | 91.7% (83–92%) |
| Average minutes of advanced wait staff training | 15 | NA | 11.0 (0–19) |
| Average % of topics covered in advanced training c | 100% | NA | 91.7% (83–92%) |
| Dose Received | |||
| % of kitchen staff received kitchen training | 100% | NA | 47.2% (29–50%) |
| % of wait staff received general training | 100% | NA | 38.5% (0–78%) |
| % of wait staff received advanced training | 50% e | NA | 56.0% (0–86%) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayala, G.X.; Castro, I.A.; Pickrel, J.L.; Lin, S.-F.; Williams, C.B.; Madanat, H.; Jun, H.-J.; Zive, M. A Cluster Randomized Trial to Promote Healthy Menu Items for Children: The Kids’ Choice Restaurant Program. Int. J. Environ. Res. Public Health 2017, 14, 1494. https://doi.org/10.3390/ijerph14121494
Ayala GX, Castro IA, Pickrel JL, Lin S-F, Williams CB, Madanat H, Jun H-J, Zive M. A Cluster Randomized Trial to Promote Healthy Menu Items for Children: The Kids’ Choice Restaurant Program. International Journal of Environmental Research and Public Health. 2017; 14(12):1494. https://doi.org/10.3390/ijerph14121494
Chicago/Turabian StyleAyala, Guadalupe X., Iana A. Castro, Julie L. Pickrel, Shih-Fan Lin, Christine B. Williams, Hala Madanat, Hee-Jin Jun, and Michelle Zive. 2017. "A Cluster Randomized Trial to Promote Healthy Menu Items for Children: The Kids’ Choice Restaurant Program" International Journal of Environmental Research and Public Health 14, no. 12: 1494. https://doi.org/10.3390/ijerph14121494
APA StyleAyala, G. X., Castro, I. A., Pickrel, J. L., Lin, S. -F., Williams, C. B., Madanat, H., Jun, H. -J., & Zive, M. (2017). A Cluster Randomized Trial to Promote Healthy Menu Items for Children: The Kids’ Choice Restaurant Program. International Journal of Environmental Research and Public Health, 14(12), 1494. https://doi.org/10.3390/ijerph14121494