Exploratory Temporal and Spatial Analysis of Myocardial Infarction Hospitalizations in Calgary, Canada

Abstract
:1. Introduction
2. Materials and Methods
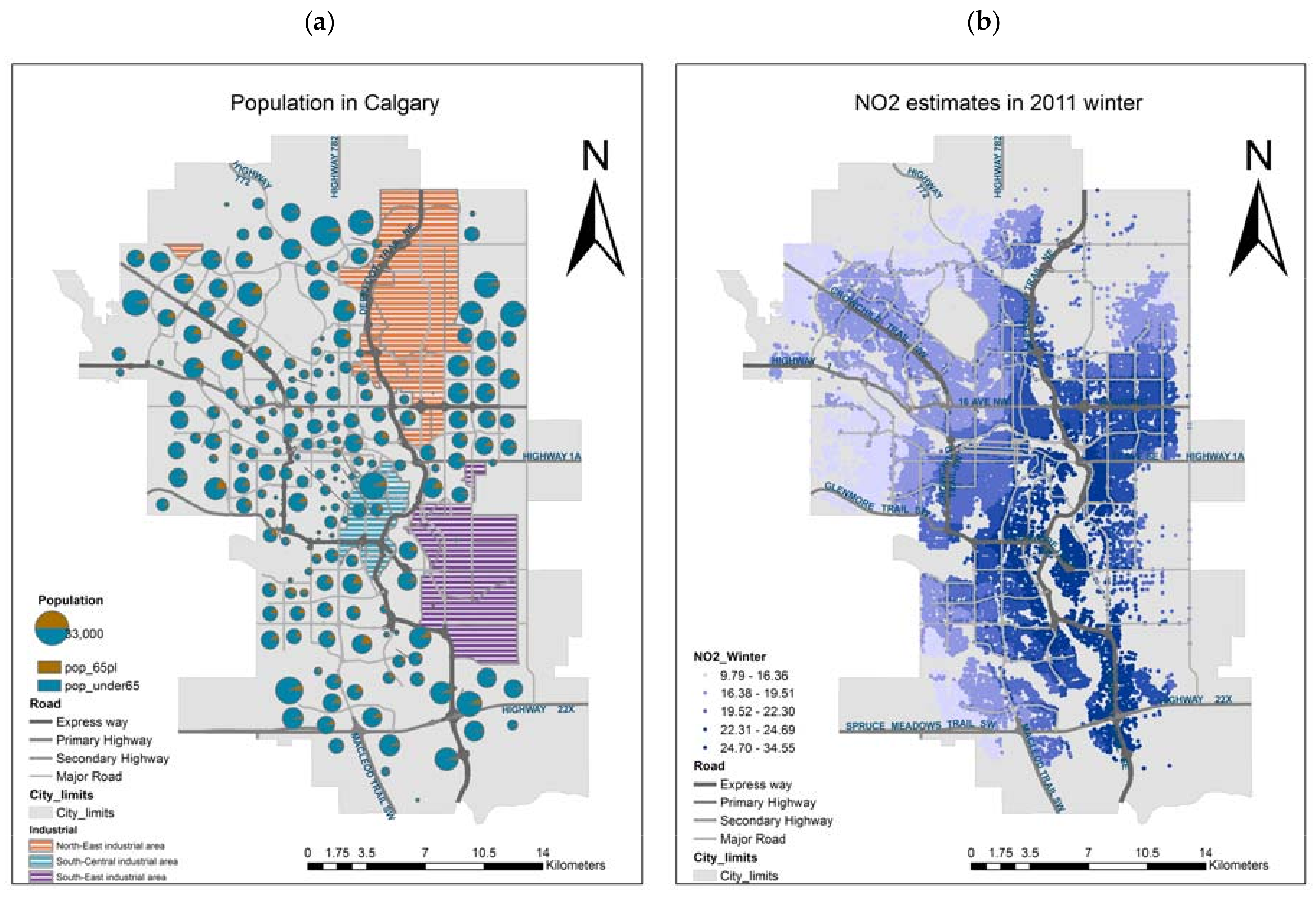
2.1. Study Area
2.2. Data
2.3. Methods
2.3.1. Temporal Analysis
2.3.2. Spatial Analysis
3. Results
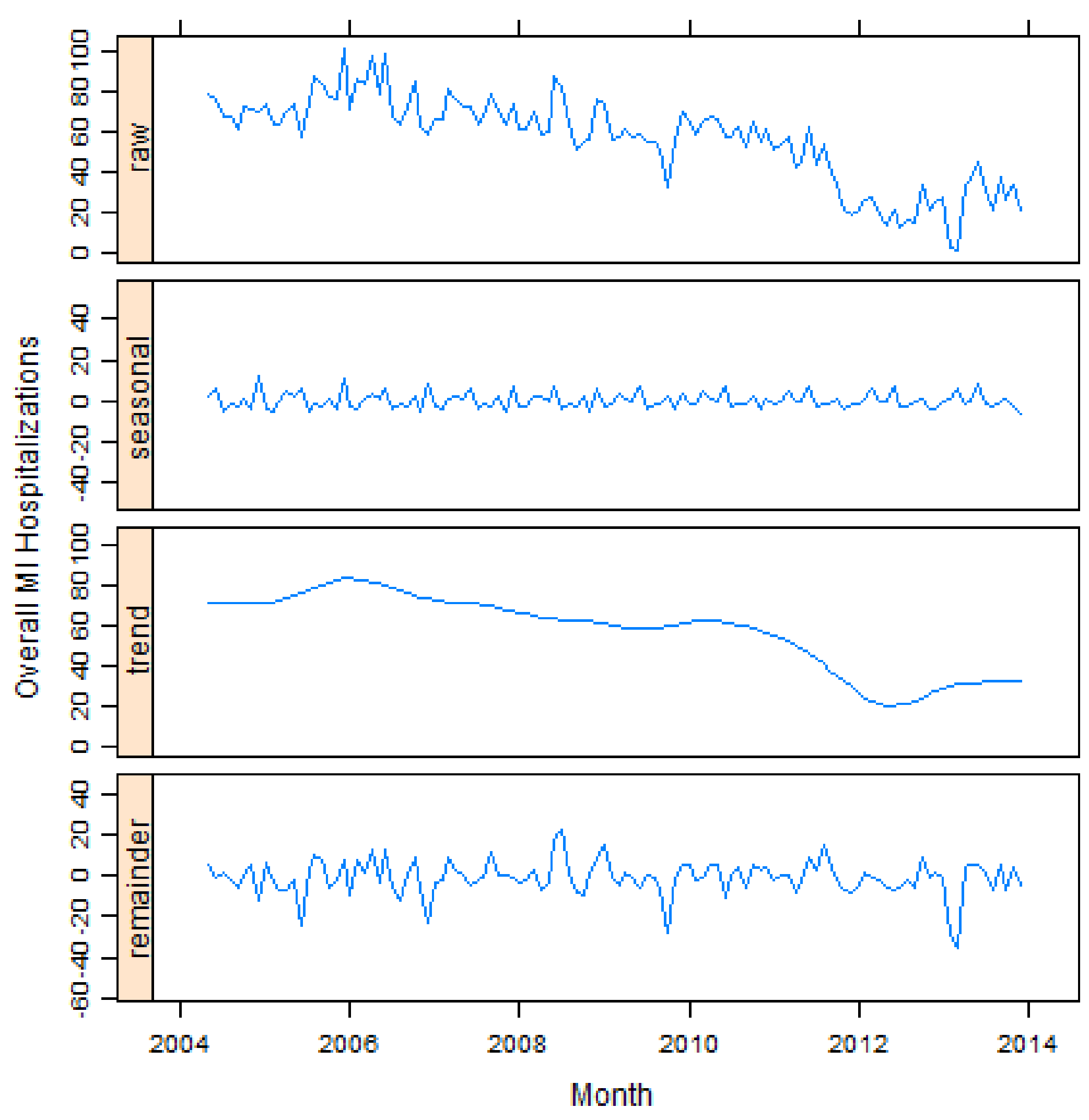
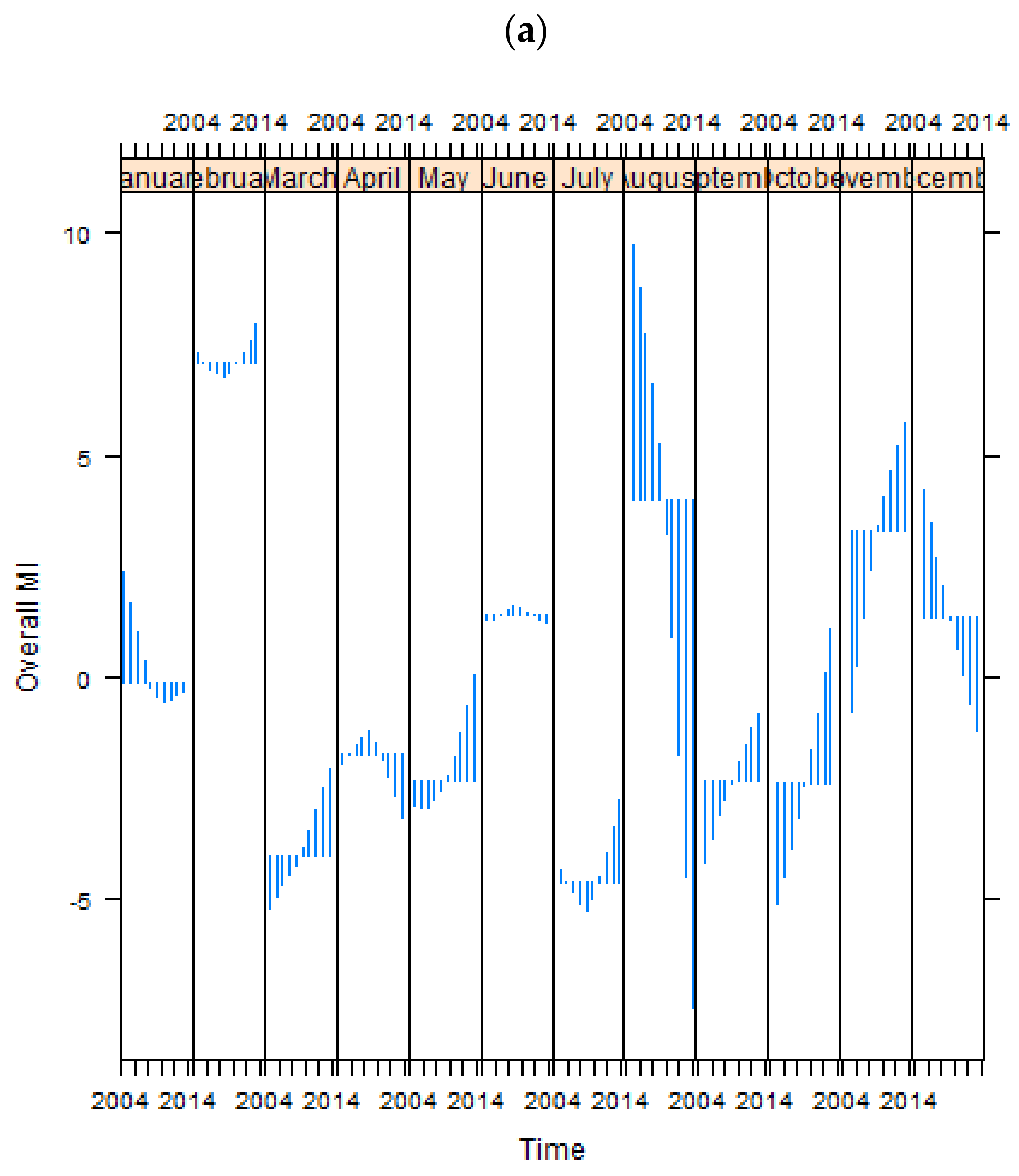
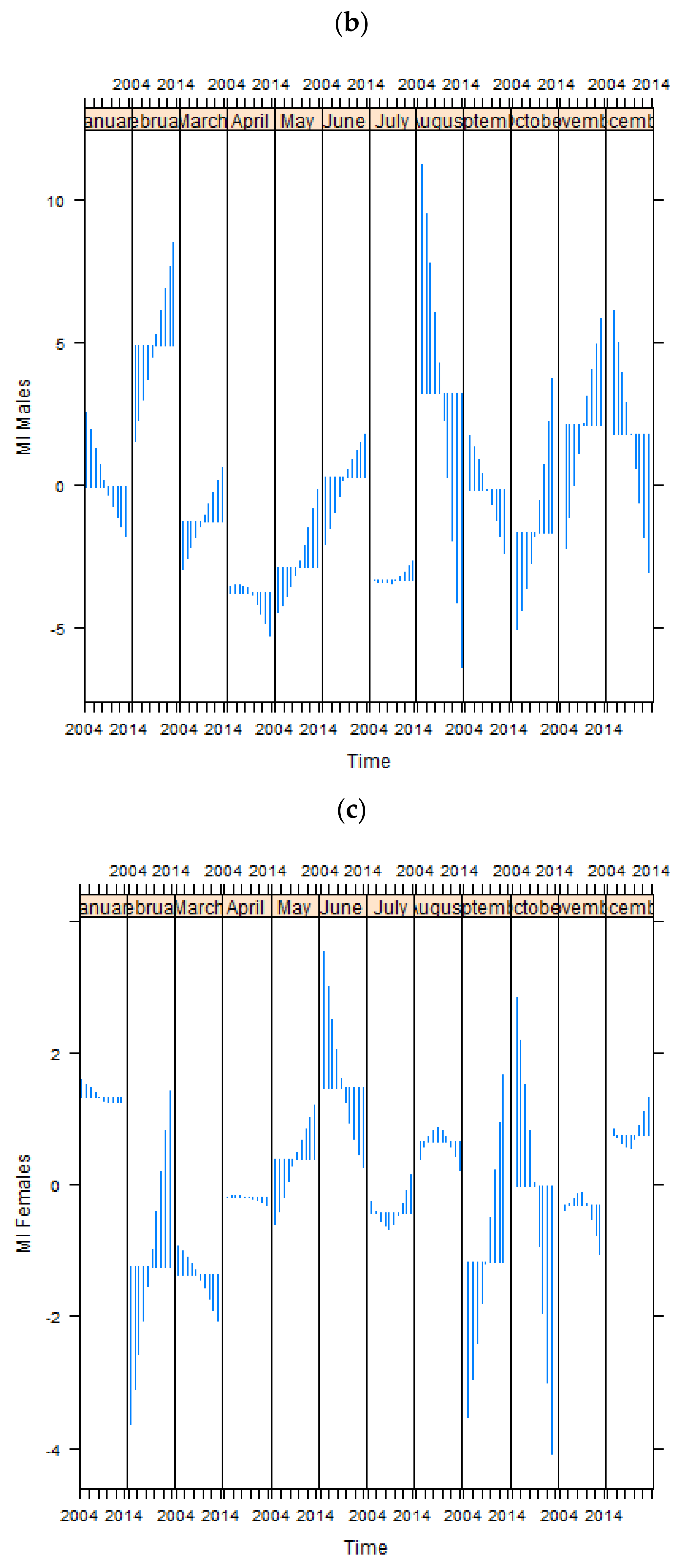
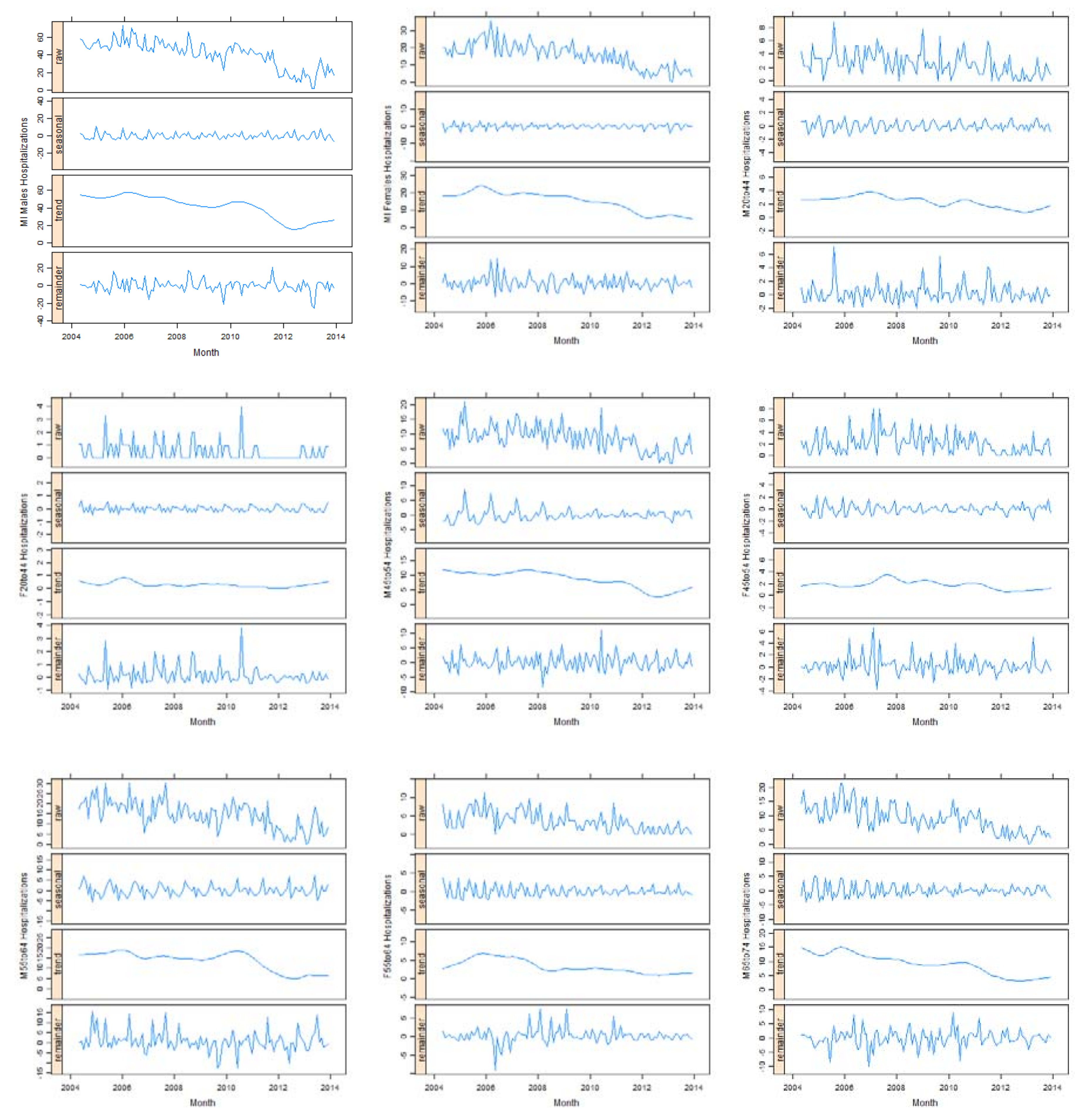
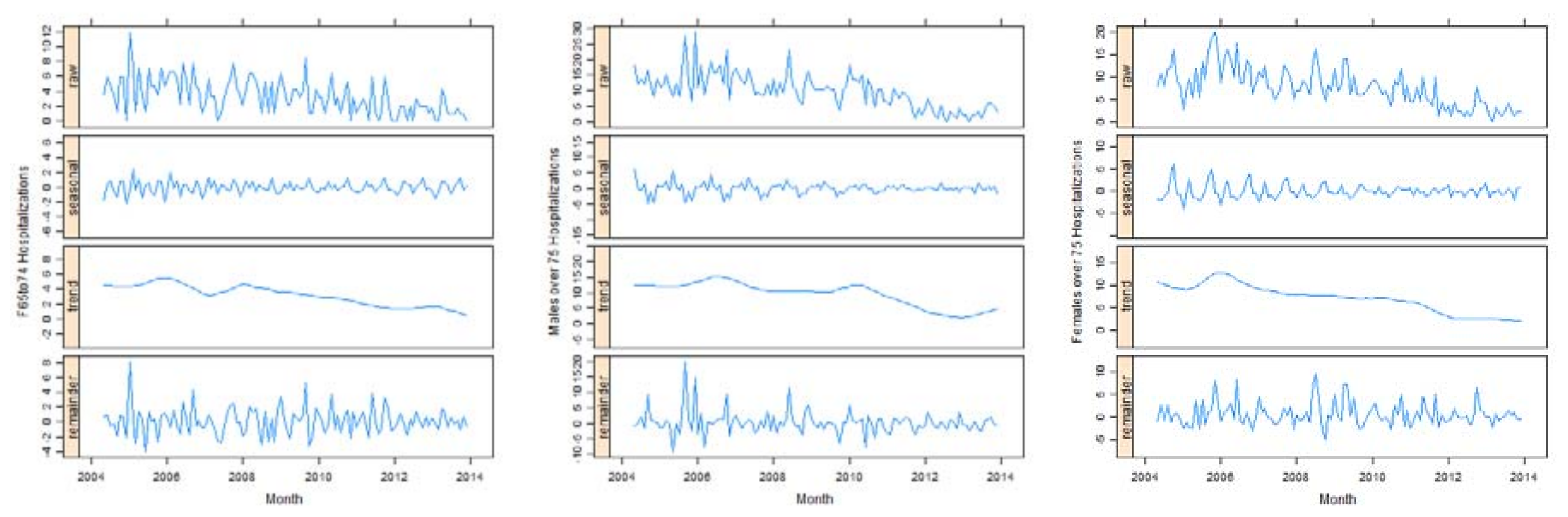
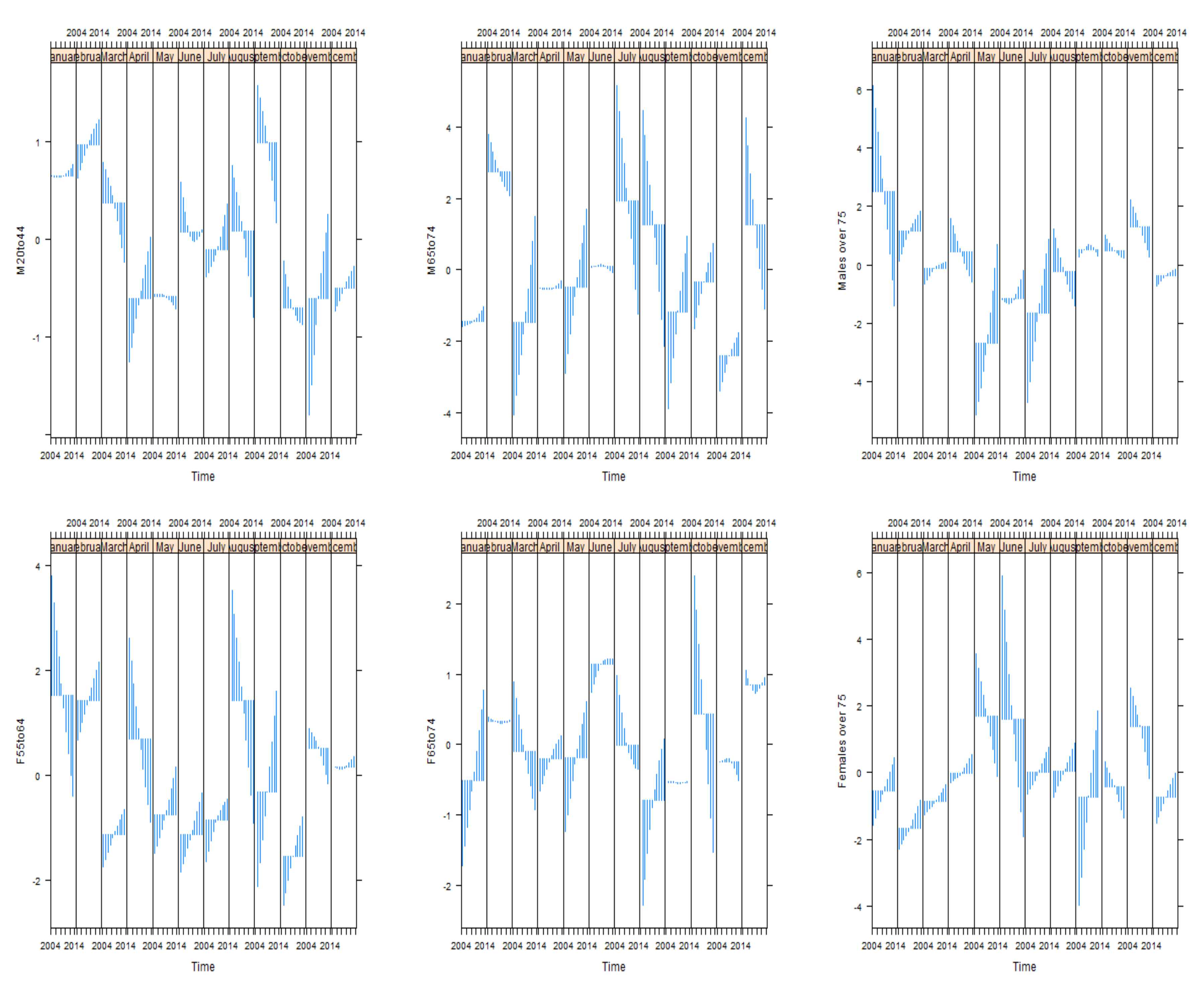
3.1. Seasonal Trend Decomposition
3.2. Linear Trend of MI Hospitalizations
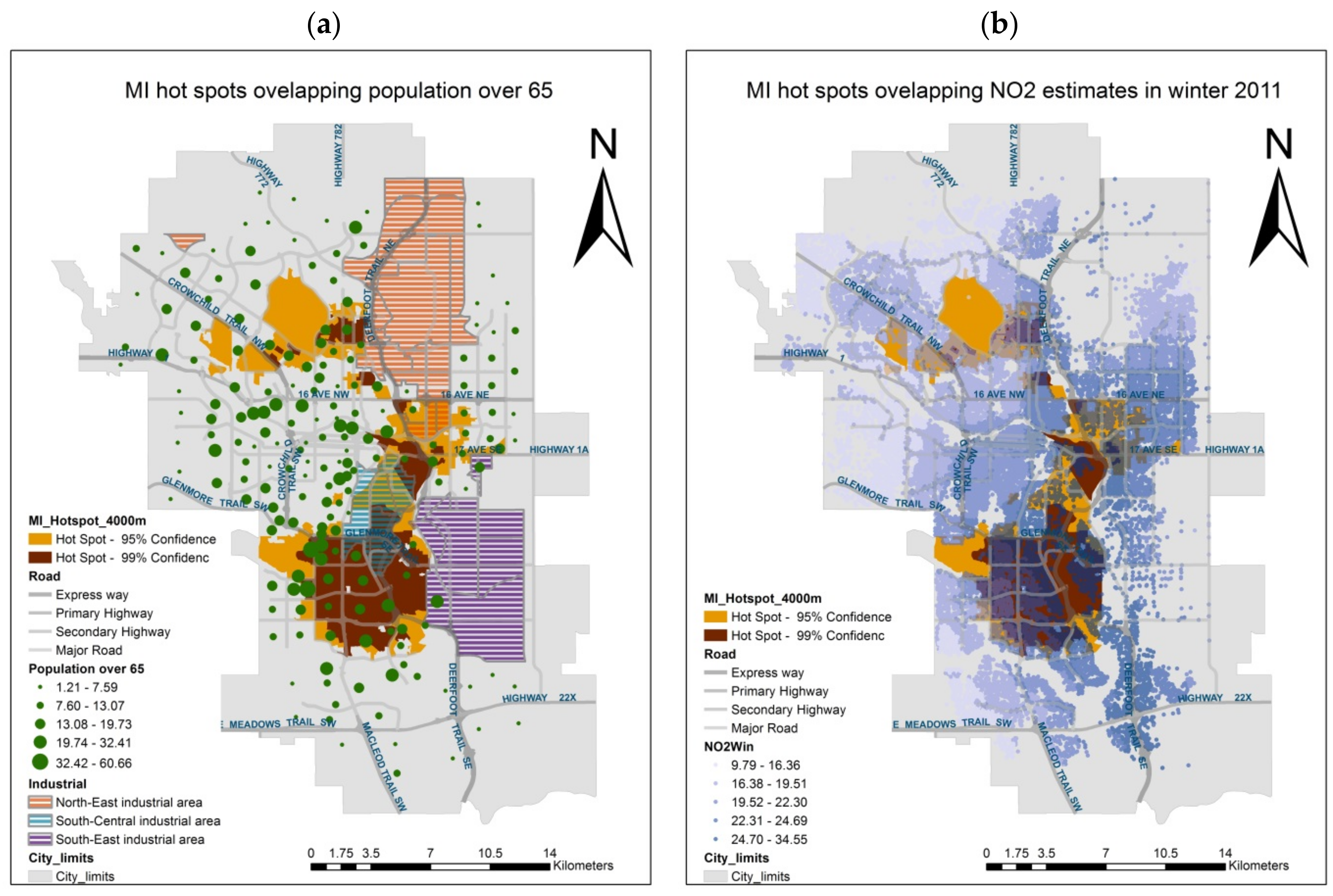
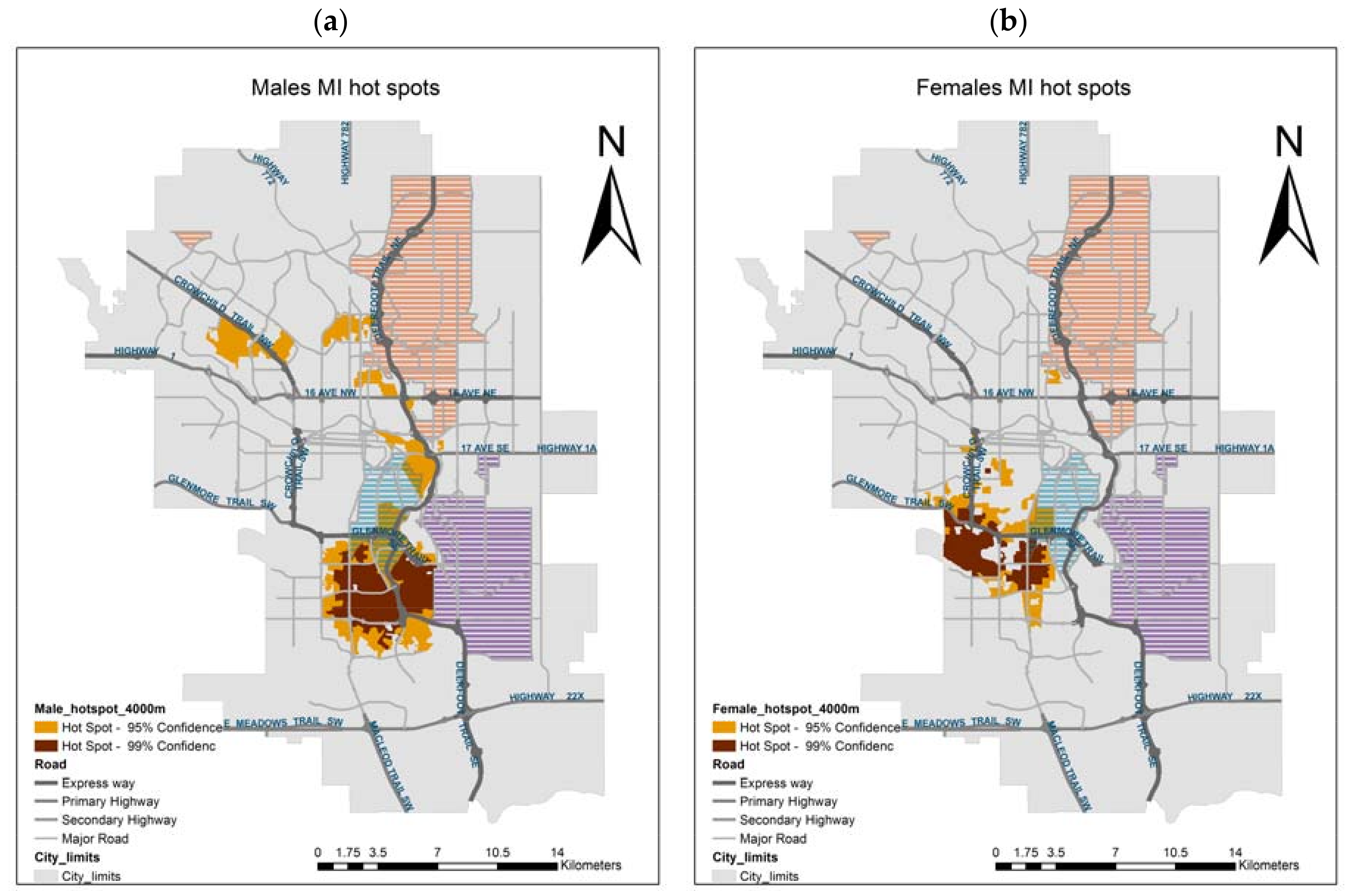
3.3. Spatial Analysis
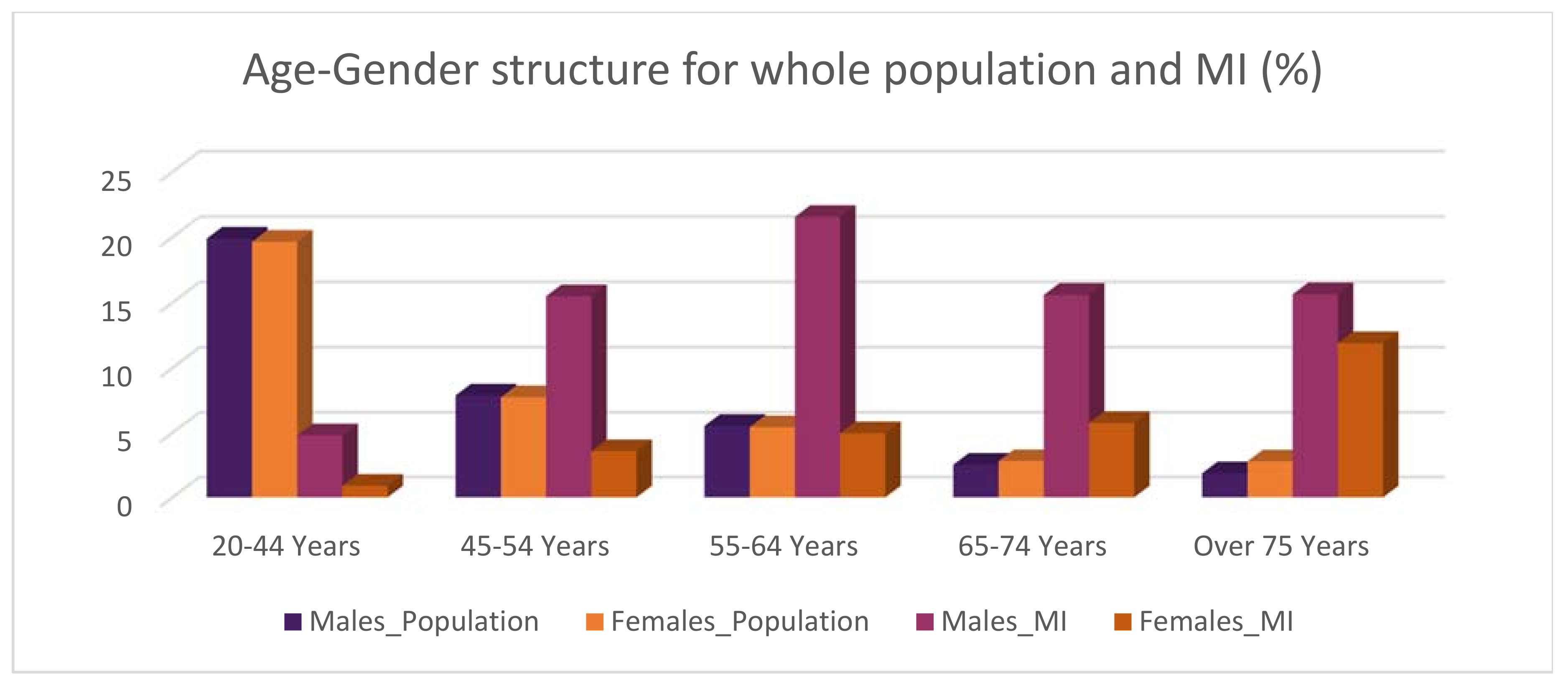
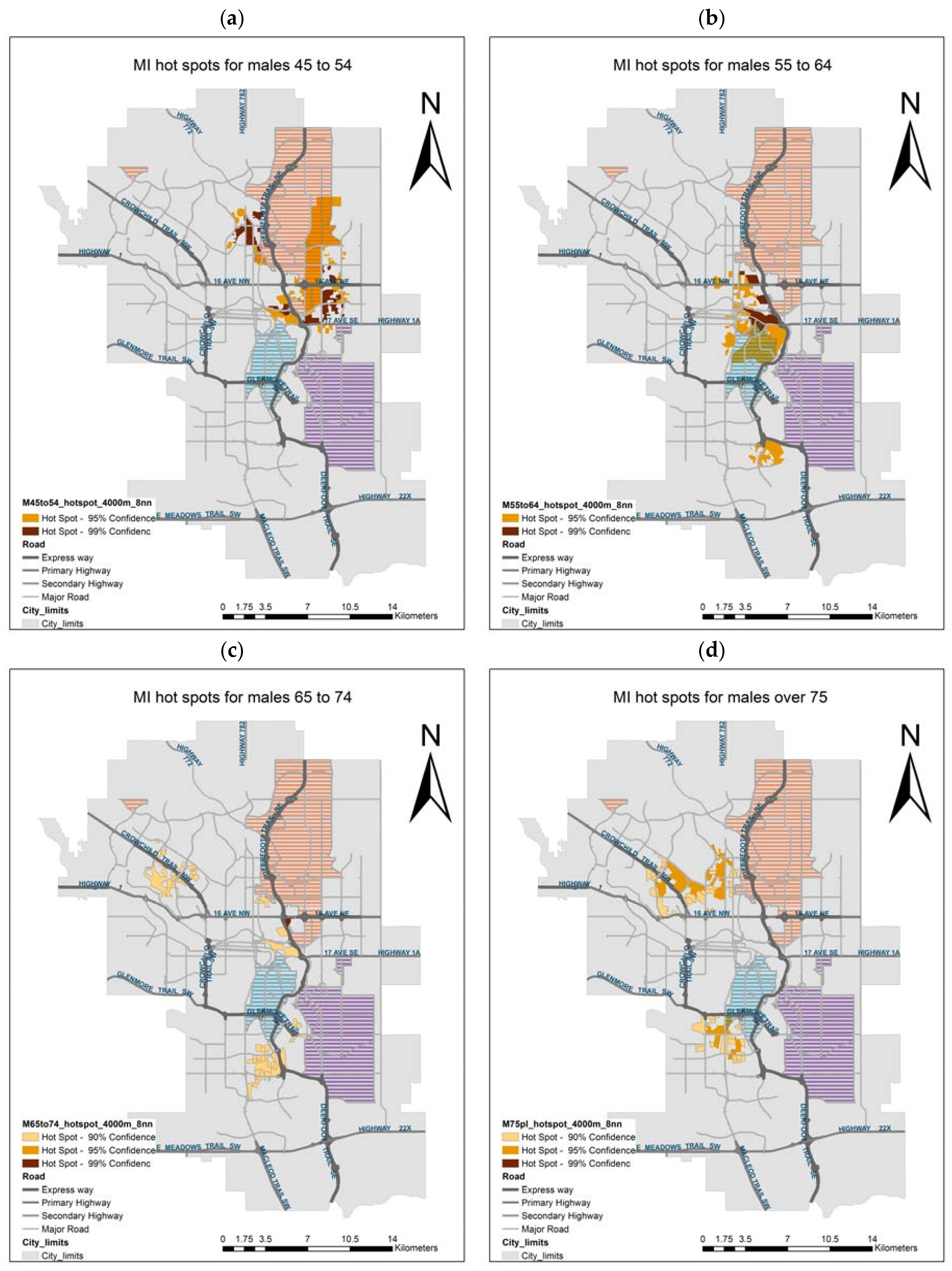
Spatial Analysis for Age and Gender Specific Groups
4. Discussion
4.1. Seasonality
4.2. Long Term Linear Decreasing Trend
4.3. Spatial Pattern and Spatio-Temporal Processes
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A





References
- Mendis, S.; Thygesen, K.; Kuulasmaa, K.; Giampaoli, S.; Mähönen, M.; Ngu Blackett, K.; Lisheng, L. World Health Organization definition of myocardial infarction: 2008–2009 revision. Int. J. Epidemiol. 2011, 40, 139–146. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Prevention of Cardiovascular Disease: Guidelines for Assessment and Management of Total Cardiovascular Risk; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Statistics Canada. Leading Causes of Death, by Sex (Both Sexes). Available online: http://www.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/hlth36a-eng.htm (accessed on 16 November 2017).
- World Health Organization. Preventing Chronic Diseases: A Vital Investment; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Bayentin, L.; El Adlouni, S.; Ouarda, T.B.; Gosselin, P.; Doyon, B.; Chebana, F. Spatial variability of climate effects on ischemic heart disease hospitalization rates for the period 1989–2006 in Quebec, Canada. Int. J. Health Geogr. 2010, 9, 5. [Google Scholar] [CrossRef] [PubMed]
- Majlund, K.T.; Kjær, E.A.; Gunnar, G.; Jasper, S. Geographical clustering of incident acute coronary infaction in Denmark: A spatial analysis approach. Spat. Spatio-Temporal Epidemiol. 2016, 19, 46–59. [Google Scholar]
- Caswell, J.M. Exploring spatial trends in Canadian incidence of hospitalization due to myocardial infarction with additional determinants of health. Public Health 2016, 140, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Gabet, A.; Chatignoux, E.; Ducimetière, P.; Danchin, N.; Olié, V. Differential trends in myocardial infarction mortality over 1975–2010 in France according to gender: An age-period-cohort analysis. Int. J. Cardiol. 2016, 223, 660–664. [Google Scholar] [CrossRef] [PubMed]
- Sidney, S.; Quesenberry, C.P., Jr.; Jaffe, M.G.; Sorel, M.; Nguyen-huynh, M.N.; Kushi, L.H.; Go, A.S.; Rana, J.S. Recent Trends in Cardiovascular Mortality in the United States and Public Health Goals. JAMA Cardiol. 2016, 1, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Health Fact Sheets: The 10 Leading Causes of Death, 2012; Statistics Canada: Ottawa, ON, Canada, 2015. [Google Scholar]
- Tu, J.V.; Nardi, L.; Fang, J.; Liu, J.; Khalid, L.; Johansen, H. National trends in rates of death and hospital admissions related to acute myocardial infarction, heart failure and stroke, 1994–2004. CMAJ 2009, 180, E118–E125. [Google Scholar] [CrossRef] [PubMed]
- Tu, J.V.; Khan, A.M.; Ng, K.; Chu, A. Recent temporal changes in atherosclerotic cardiovascular diseases in Ontario: Clinical and health systems impact. Can. J. Cardiol. 2017, 33, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Fares, A. Winter Cardiovascular Diseases Phenomenon. N. Am. J. Med. Sci. 2013, 5, 266–279. [Google Scholar] [CrossRef] [PubMed]
- Park, H.E.; Koo, B.-K.; Lee, W.; Cho, Y.; Park, J.S.; Choi, J.-Y. Periodic variation and its effect on management and prognosis of korean patients with acute myocardial infarction. Circ. J. 2010, 74, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Chrysohoou, C.; Pitsavos, C.; Nastos, P.; Anadiotis, A.; Tentolouris, C.; Stefanadis, C.; Toutouzas, P.; Paliatsos, A. Climatological variations in daily hospital admissions for acute coronary syndromes. Int. J. Cardiol. 2004, 94, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Loughnan, M.E.; Nicholls, N.; Tapper, N.J. Demographic, seasonal, and spatial differences in acute myocardial infarction admissions to hospital in Melbourne Australia. Int. J. Health Geogr. 2008, 7, 42. [Google Scholar] [CrossRef] [PubMed]
- Wijeysundera, H.; Machado, M.; Farahati, F.; Wang, X.; Witteman, W.; van der Velde, G.; Tu, J.V.; Lee, D.S.; Goodman, S.G.; Petrella, R.; et al. Association of temporal trends in risk factors and treatment uptake with coronary heart disease mortality, 1994–2005. JAMA 2010, 303, 1841–1847. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Calgary [Economic Region], Alberta and Alberta [Province] (Table). Census Profile. 2016 Census. Available online: http://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/index.cfm?Lang=E (accessed 7 December 2017).
- Nkemdirim, L.C. The role of wind velocity and mixing depth in the distribution of urban air pollution hazard in Calgary, AB, Canada. GeoJournal 1984, 8, 197–200. [Google Scholar] [CrossRef]
- Environment Canada. Canadian Climate Normals 1981–2010 Station Data: Calgary Int’l. Airport; Environment Canada: Calgary, AB, Canada, 2017. [Google Scholar]
- Calgary Region Airshed Zone. All Source Pollutant Emissions Inventory for the Calgary Region Airshed Zone (CRAZ)—Spatial Allocation Project (2012–2013) (Final Draft); Calgary Region Airshed Zone: Calgary, AB, Canada, 2013. [Google Scholar]
- Bertazzon, S.; Johnson, M.; Eccles, K.; Kaplan, G.G. Accounting for spatial effects in land use regression for urban air pollution modeling. Spat. Spatio-Temporal Epidemiol. 2015, 14–15, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Bertazzon, S. Geographic Information Science: 9th International Conference, GIScience 2016, Montreal, QC, Canada, 27–30 September 2016, Proceedings; Miller, A.J., O’Sullivan, D., Wiegand, N., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 210–224. [Google Scholar]
- The City of Calgary. 2014 Civic Census Results 1; The City of Calgary: Calgary, AB, Canada, 2014. [Google Scholar]
- Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease (APPROACH). Available online: http://www.approach.org/index.html (accessed on 13 October 2017).
- Statistics Canada. Statistics Canada Catalogue no. 98-316-XWE. Ottawa. Released 24 October 2012; Statistics Canada: Ottawa, ON, Canada, 2011. [Google Scholar]
- Sanchez-vazquez, M.J.; Nielen, M.; Gunn, G.J.; Lewis, F.I. Using seasonal-trend decomposition based on loess (STL) to explore temporal patterns of pneumonic lesions in finishing pigs slaughtered in England, 2005–2011. Prev. Vet. Med. 2012, 104, 65–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleveland, R.; Cleveland, W.; McRae, J.E.; Terpenning, I. STL: A seasonal-trend decomposition prodedure based on loess. J. Off. Stat. 1990, 6, 3–33. [Google Scholar]
- Enders, W. Applied Econometric Time Series, 4th ed.; Wiley: Toronto, ON, Canada, 2014; p. 485. [Google Scholar]
- Cleveland, W.S.; Devlin, S.J. Locally weighted regression: An approach to regression analysis by local fitting. J. Am. Stat. Assoc. 1988, 83, 596–610. [Google Scholar] [CrossRef]
- Pickup, M. Quantitative Applications in the Social Sciences: Introduction to Time Series Analysis; SAGE Publications Inc.: Thousand Oaks, CA, USA, 2015. [Google Scholar]
- Moran, P.A.P. Notes on continuous stochastic phenomena. Biometrika 1950, 37, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Calder, C.A.; Cressie, N. Beyond Moran’s I: Testing for spatial dependence based on the spatial autoregressive model. Geogr. Anal. 2007, 39, 357–375. [Google Scholar] [CrossRef]
- Ord, K. Estimation methods for models of spatial interaction. J. Am. Stat. Assoc. 1975, 70, 120–126. [Google Scholar] [CrossRef]
- Environmental Systems Research Institute (ESRI). Incremental Spatial Autocorrelation. Available online: http://desktop.arcgis.com/en/arcmap/10.3/tools/spatial-statistics-toolbox/incremental-spatial-autocorrelation.html (accessed on 1 January 2017).
- Getis, A.; Ord, J.K. The analysis of spatial association. Geogr. Anal. 1992, 24, 189–206. [Google Scholar] [CrossRef]
- Anselin, L. Local indicators of spatial association-LISA. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Riffenburgh, R.H. Statistics in Medicine; Elsevier/Academic Press: Cambridge, MA, USA, 2012. [Google Scholar]
- Hopstock, L.A.; Wilsgaard, T.; Njølstad, I.; Mannsverk, J.; Mathiesen, E.B.; Løchen, M.; Bønaa, K.H. Seasonal variation in incidence of acute myocardial infarction in a sub-Arctic population: The Tromsø Study 1974–2004. Eur. J. Cardiovasc. Prev. Rehabil. 2011, 18, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Fischer, T.; Lundbye-Christensen, S.; Johnsen, S.P.; Schønheyder, H.C.; Sørensen, H.T. Secular trends and seasonality in first-time hospitalization for acute myocardial infarction—A Danish population-based study. Int. J. Cardiol. 2004, 97, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Ravljen, M.; Bilban, M.; Kajfez-Bogataj, L.; Hovelja, T.; Vavpotic, D. Influence of daily individual meteorological parameters on the incidence of acute coronary syndrome. Int. J. Environ. Res. Public Health 2014, 11, 11616–11626. [Google Scholar] [CrossRef] [PubMed]
- Ku, C.S.; Yang, C.Y.; Lee, W.J.; Chiang, H.T.; Liu, C.P.; Lin, S.L. Absence of a seasonal variation in myocardial infarction onset in a region without temperature extremes. Cardiology 1998, 89, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Morabito, M.; Amedeo, P.; Cecchi, L.; Crisci, A.; Orlandini, S.; Maracchi, G.; Franco, G. Relationships between weather and myocardial infarction: A biometeorological approach. Int. J. Cardiol. 2005, 105, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, G.C.; Keatinge, W.R. Early increases in ischaemic heart disease mortality dissociated from and later changes associated with respiratory mortality after cold weather in south east England. J. Epidemiol. Community Health 1997, 51, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Jehn, M.; Appel, L.J.; Sacks, F.M.; Miller, E.R.; DASH Collaborative Research Group. The effect of ambient temperature and barometric pressure on ambulatory blood pressure variability. Am. J. Hypertens. 2002, 15, 941–945. [Google Scholar] [CrossRef]
- Sen, T.; Astarcioglu, M.A.; Asarcikli, L.D.; Kilit, C.; Kafes, H.; Parspur, A.; Yaymaci, M.; Pinar, M.; Tüfekcioglu, O.; Amasyali, B. The effects of air pollution and weather conditions on the incidence of acute myocardial infarction. Am. J. Emerg. Med. 2016, 34, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Varotsos, C.; Kondratyev, K.Y.; Efstathiou, M. On the seasonal variation of the surface ozone in Athens, Greece. Atmos. Environ. 2001, 35, 315–320. [Google Scholar] [CrossRef]
- Pudasainee, D.; Sapkota, B.; Shrestha, M.L.; Kaga, A.; Kondo, A.; Inoue, Y. Ground level ozone concentrations and its association with NOx and meteorological parameters in Kathmandu valley, Nepal. Atmos. Environ. 2006, 40, 8081–8087. [Google Scholar] [CrossRef]
- Wang, X.; Kindzierski, W.; Kaul, P.; Sun, Q. Air pollution and acute myocardial infarction hospital admission in Alberta, Canada: A three-step procedure case-crossover study. PLoS ONE 2015, 10, e0132769. [Google Scholar] [CrossRef] [PubMed]
- Lanki, T.; Pekkanen, J.; Aalto, P.; Elosua, R.; Berglind, N.; D’Ippoliti, D.; Kulmala, M.; Nyberg, F.; Peters, A.; Picciotto, S.; et al. Associations of traffic related air pollutants with hospitalisation for first acute myocardial infarction: The HEAPSS study. Occup. Environ. Med. 2006, 63, 844–851. [Google Scholar] [CrossRef] [PubMed]
- Bender, R.; Lange, S. Adjusting for multiple testing—When and how? J. Clin. Epidemiol. 2001, 54, 343–349. [Google Scholar] [CrossRef]
- Armstrong, R.A. When to use the Bonferroni correction. Ophthalmic Physiol. Opt. 2014, 34, 502–508. [Google Scholar] [CrossRef] [PubMed]
- United Way Calgary and Area. Mapping Poverty in Calgary; United Way Calgary and Area: Calgary, AB, Canada, 2011. [Google Scholar]
- Calgary Region Airshed Zone. Calgary Region Airshed Zone 2013 Annual Report; Calgary Region Airshed Zone: Calgary, AB, Canada, 2013. [Google Scholar]
- Trentinaglia, I.; Hörmann, A.; Wichmann, H.E.; Löwel, H. Exposure to traffic and the onset of myocardial infarction. N. Engl. J. Med. 2004, 351, 1721–1730. [Google Scholar]
- Murad, M.H. Main air pollutants and myocardial infarction. J. Am. Med. Assoc. Rev. 2012, 307, 713–721. [Google Scholar]
- D’Ippoliti, D.; Forastiere, F.; Ancona, C.; Agabiti, N.; Fusco, D.; Michelozzi, P.; Perucci, C.A. Air pollution and myocardial infarction in Rome: A case-crossover analysis. Epidemiology 2003, 14, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Bertazzon, S.; Shahid, R. Schools, air pollution, and active transportation: An exploratory spatial analysis of calgary, Canada. Int. J. Environ. Res. Public Health 2017, 14, 834. [Google Scholar] [CrossRef] [PubMed]
- Shahid, R.; Bertazzon, S. Local Spatial Analysis and Dynamic Simulation of Childhood Obesity and Neighbourhood Walkability in a Major Canadian City. AIMS Public Health 2015, 2, 616–637. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trend Model | Intercept | Trend Coefficient | t Value | (p-Value) | R2 |
|---|---|---|---|---|---|
| Overall MI | 86.29 | −0.50 | −22.44 | <2 × 10−16 | 0.82 |
| Males | 61.46 | −0.35 | −21.28 | <2 × 10−16 | 0.80 |
| 45–54 Years | 13.09 | −0.08 | −20.97 | <2 × 10−16 | 0.79 |
| 55–64 Years | 20.03 | −0.11 | −14.14 | <2 × 10−16 | 0.64 |
| 65–74 Years | 15.00 | −0.10 | −32.22 | <2 × 10−16 | 0.90 |
| Over 75 Years | 15.53 | −0.10 | −18.06 | <2 × 10−16 | 0.74 |
| Females | 24.11 | −0.15 | −23.32 | <2 × 10−16 | 0.83 |
| 65–74 Years | 5.43 | −0.04 | −26.93 | <2 × 10−16 | 0.86 |
| Over 75 Years | 12.17 | −0.09 | −28.42 | <2 × 10−16 | 0.88 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, X.; Bertazzon, S. Exploratory Temporal and Spatial Analysis of Myocardial Infarction Hospitalizations in Calgary, Canada. Int. J. Environ. Res. Public Health 2017, 14, 1555. https://doi.org/10.3390/ijerph14121555
Liu X, Bertazzon S. Exploratory Temporal and Spatial Analysis of Myocardial Infarction Hospitalizations in Calgary, Canada. International Journal of Environmental Research and Public Health. 2017; 14(12):1555. https://doi.org/10.3390/ijerph14121555
Chicago/Turabian StyleLiu, Xiaoxiao, and Stefania Bertazzon. 2017. "Exploratory Temporal and Spatial Analysis of Myocardial Infarction Hospitalizations in Calgary, Canada" International Journal of Environmental Research and Public Health 14, no. 12: 1555. https://doi.org/10.3390/ijerph14121555
APA StyleLiu, X., & Bertazzon, S. (2017). Exploratory Temporal and Spatial Analysis of Myocardial Infarction Hospitalizations in Calgary, Canada. International Journal of Environmental Research and Public Health, 14(12), 1555. https://doi.org/10.3390/ijerph14121555