Do Individual and Neighborhood Characteristics Influence Perceived Air Quality?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Statistical Units
2.2. Subjective Measures of Air Pollution and Individual Characteristics
- -
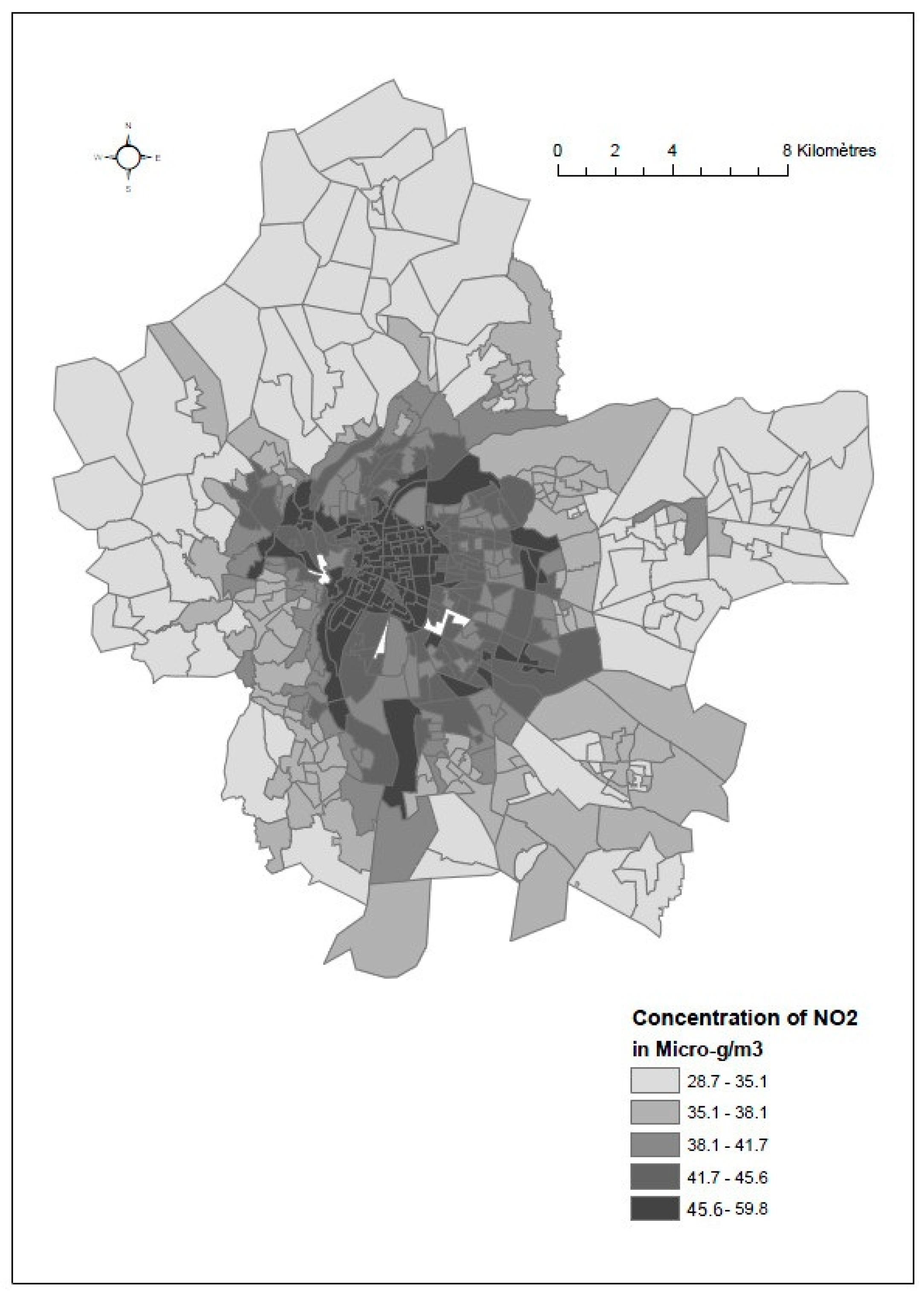
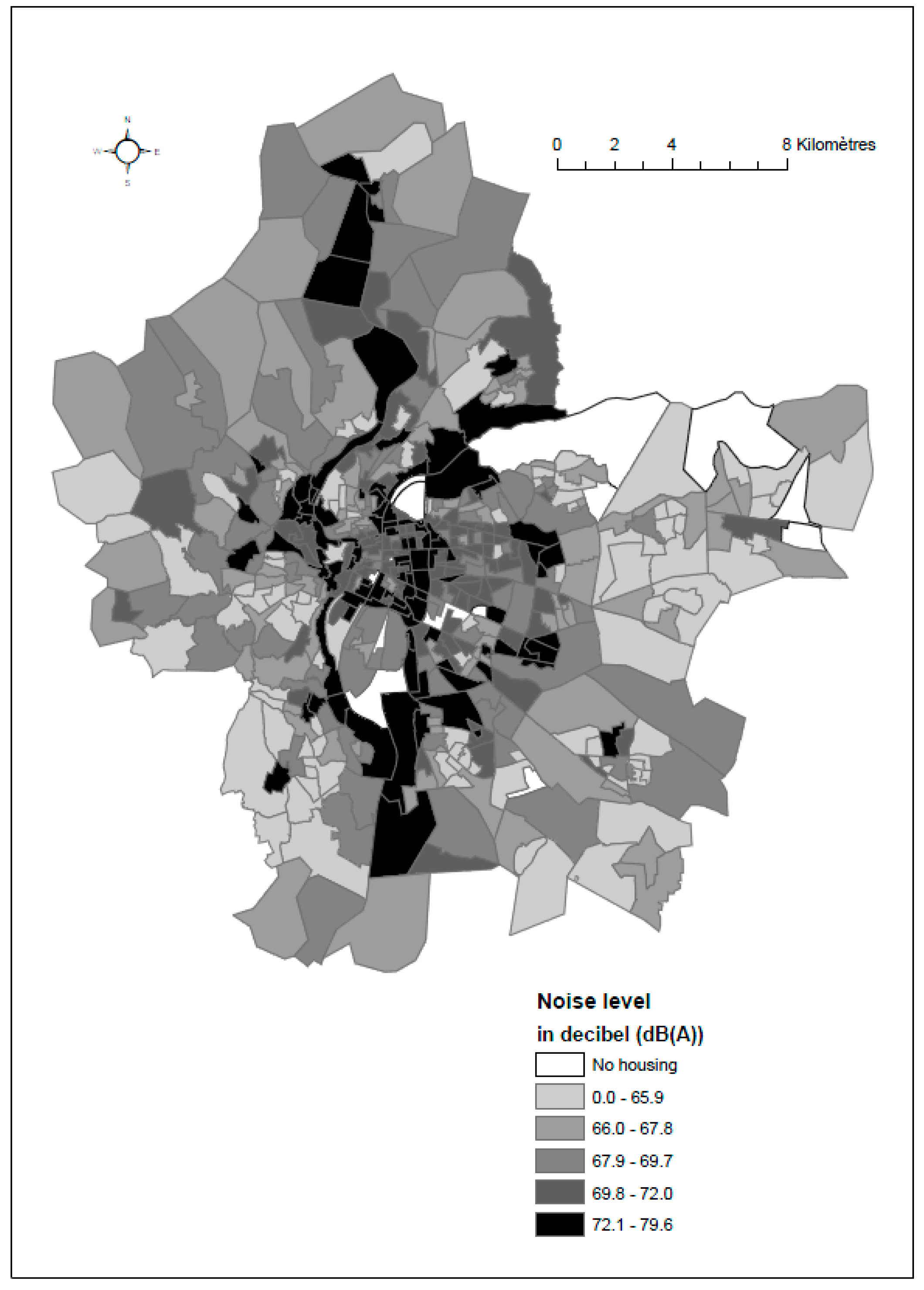
- Census blocks of LMA were first classified according to the median level of nitrogen dioxide (NO2 expressed in μg/m3) and noise level (equal to 40.2 μg/m3 and 32.9 decibels, respectively). Next, four distinct categories of census blocks were constructed: census blocks with: (i) lower levels of NO2 and noise than the median; (ii) a lower level of NO2 and a higher level of noise than the median; (iii) a higher level of NO2 and a lower level of noise than the median, and (iv) higher levels of NO2 and noise than the median. Noise and air pollution indicators were chosen as good indicators of environmental pollution in the LMA. Indeed, in the Lyon Metropolitan Area, traffic road has been recognized to be one of the main contributors of air pollution (http://www.ppa-lyon.org/). Noise exposure constitutes additional environmental consequences of the traffic road. In addition, following the recommendation of the second plan of environmental health of the Rhône-Alpes region, a web platform named Orphane (http://www.orhane.fr/) has been created to identify the part of the region accumulating high levels of air pollution and noise to better target action and decision making.
- -
- Next, 2500 phone numbers per category were randomly selected from the France Telecom Institute and other phone companies—creating a random data base of 10,000 phone numbers.
- -
- Finally, in each category, phone numbers were called until 250 people answered. Three calls, on different days and at different times, were made before moving to another phone number. In total, the study population included 1000 people.
- (1)
- Do you agree with the following statement: “the quality of the air you breathe within your residential census block is good”
- (2)
- Would you ever consider living in another place where air quality is better? (Yes/no)
- (3)
- Are you aware of any actions or interventions aimed at improving air quality in the Lyon Metropolitan area? (Yes/no)
- (4)
- Would you say that you are satisfied with the place where you live?
2.3. Objective Measures of Ambient Air Pollution and Neighborhood Socioeconomic Index
2.3.1. Air Pollution
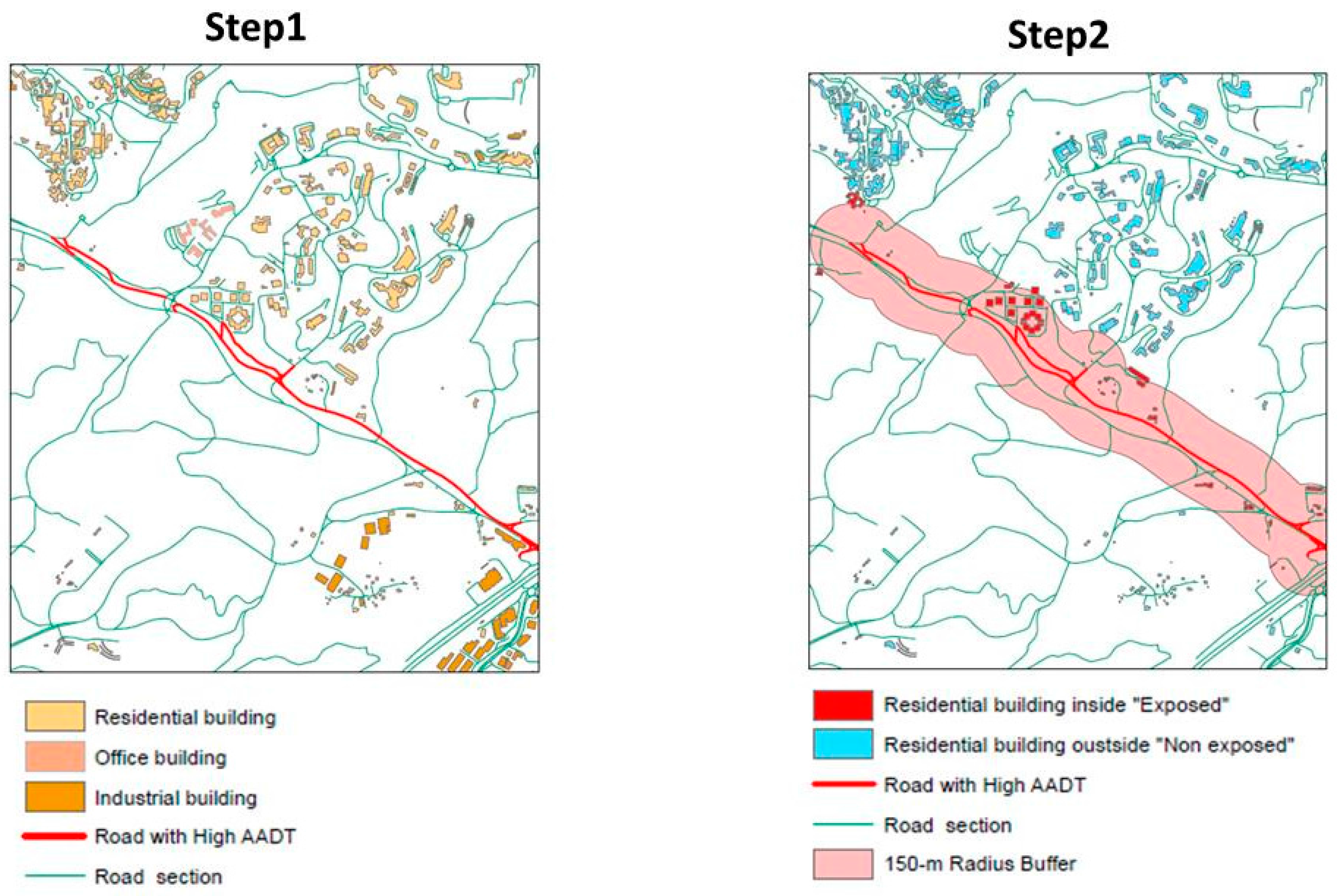
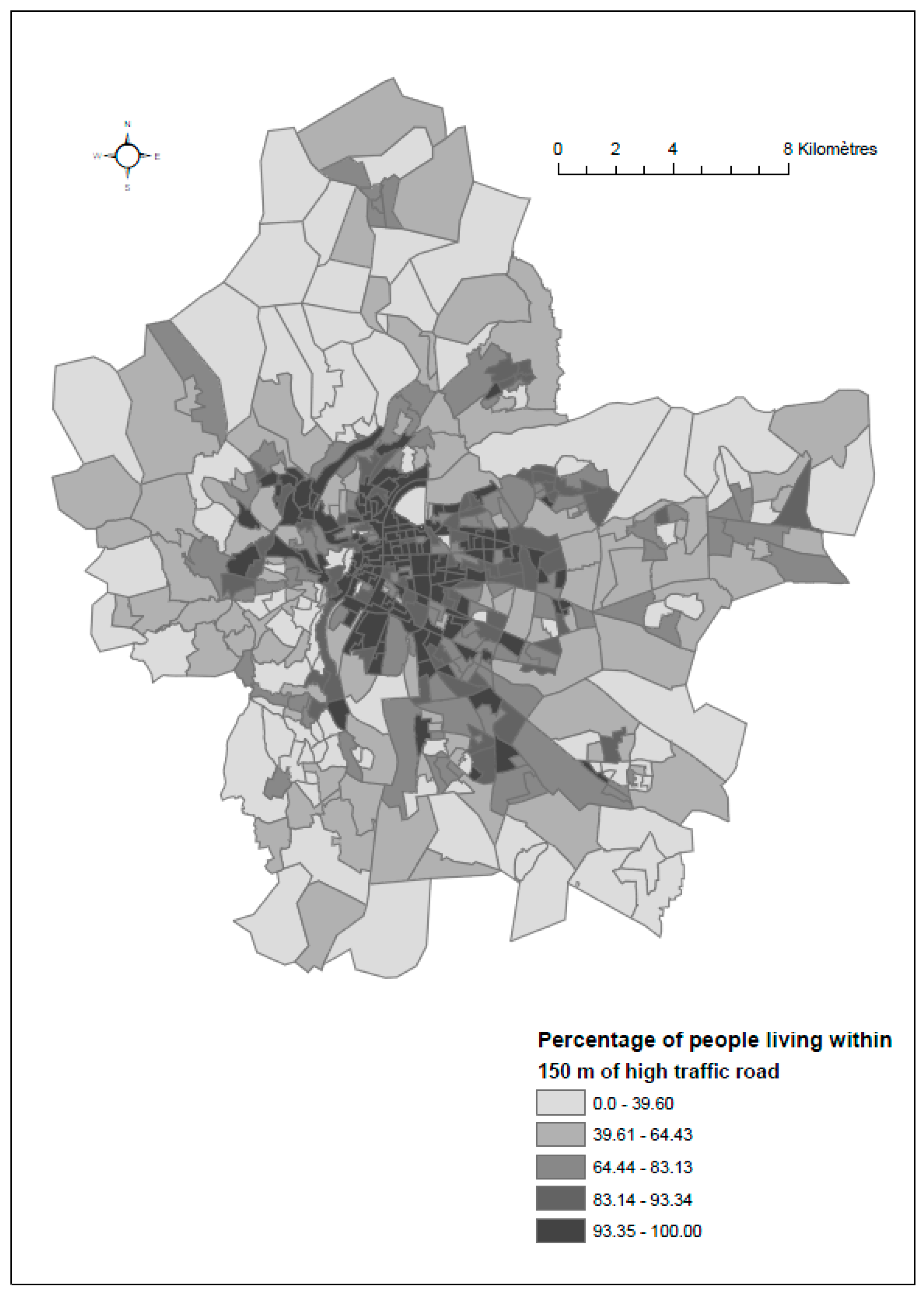
2.3.2. Heavy Residential Traffic Exposure
- (i)
- First, we modeled the distribution of inhabitants in buildings. The total number of inhabitants living in a given census block was distributed in each residential building located within the census block. To do this, two data sources were used: building volume according to the topographic database (from the National Geographic Institute) and the number of inhabitants per census block according to the national census, collected by the French National Statistics Institute (INSEE). The number of inhabitants per residential building was calculated assuming the equi-distribution to its volume.
- (ii)
- Second, the percentage of inhabitants living within 150 m of a major road was calculated for each census block. More precisely, circles with radii of 150 m were created around each road segment, as shown in Figure 2. The widest radius, of 150 m, was chosen based on studies revealing that NO2 concentrations drop off very rapidly within the first 50 m, and are divided by ten after 100 m [37,38]. We intersected these circles (buffers) with the topological database to pinpoint residential buildings located inside each circle which would be considered exposed to high-traffic roads. The total number of exposed inhabitants per census block was obtained by adding together the number of inhabitants of all the residential buildings within the buffers. Finally, the residential traffic exposure indicator was estimated at census block level by dividing the total number of exposed inhabitants by the population of the census block.
2.3.3. Noise Exposure
2.3.4. Green Spaces
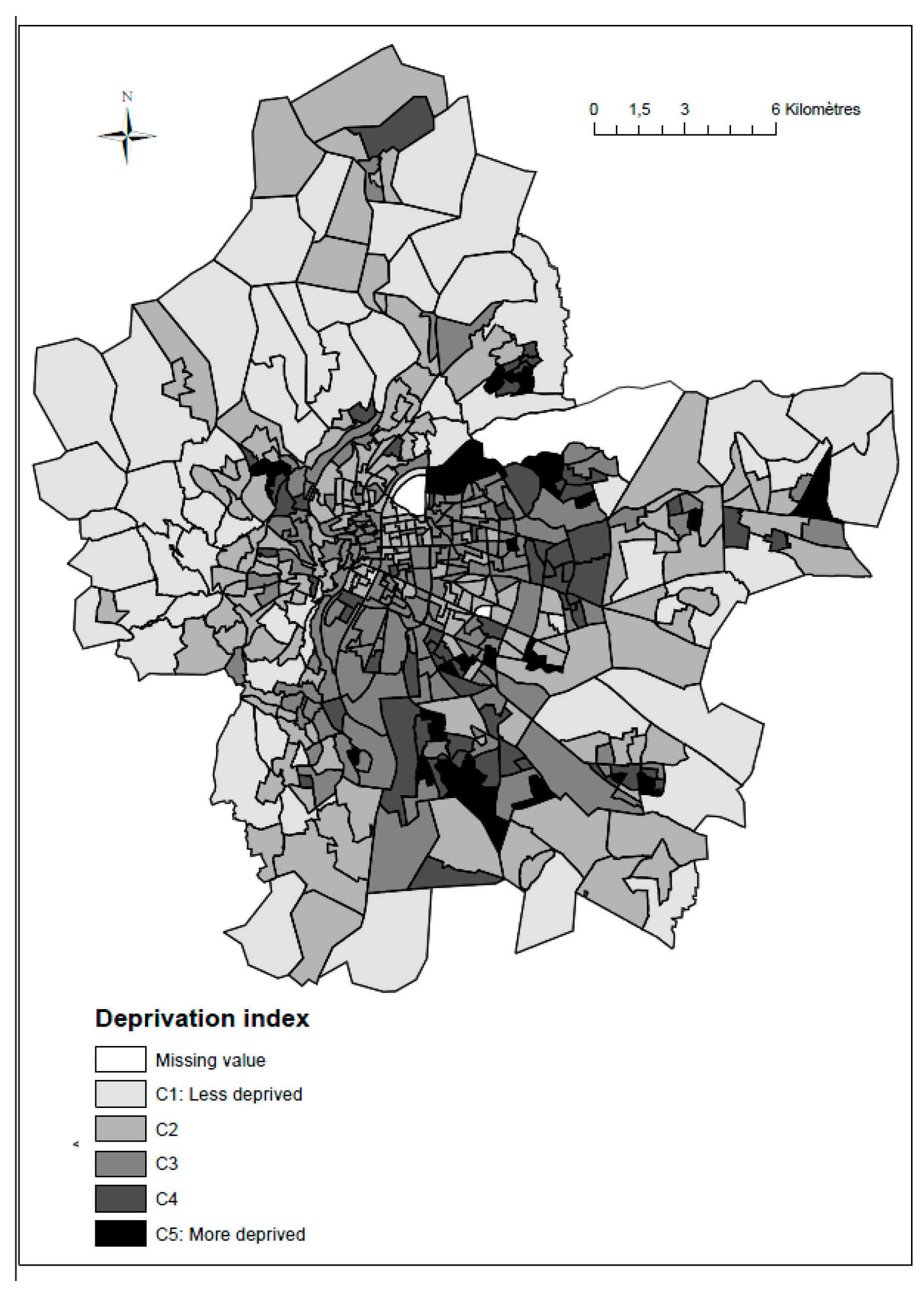
2.3.5. Socioeconomic Deprivation Index
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
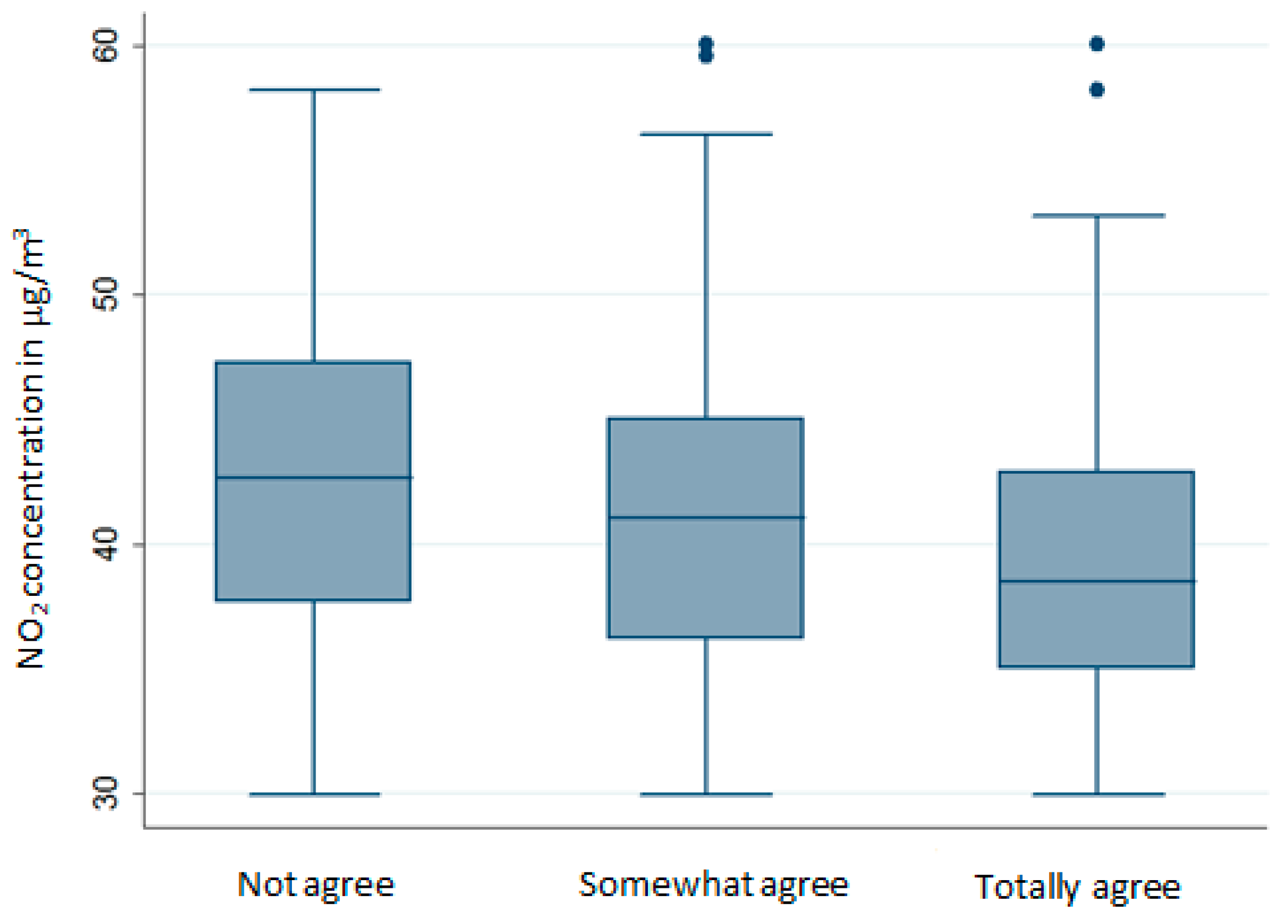
3.2. Relationship between Subjective and Objective Measures of Air Pollution
3.3. Relationship between Subjective and Objective Measures of Air Quality Based on the Demographic Characteristics of Respondents
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- World Health Organization (WHO). World Health Statistics; WHO: Geneva, Swizerland, 2013. [Google Scholar]
- Lepeule, J.; Laden, F.; Dockery, D.; Schwartz, J. Chronic exposure to fine particles and mortality: An extended follow-up of the Harvard Six Cities study from 1974 to 2009. Environ. Health Perspect. 2012, 120, 965–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hart, J.E.; Garshick, E.; Dockery, D.W.; Smith, T.J.; Ryan, L.; Laden, F. Long-term ambient multipollutant exposures and mortality. Am. J. Respir. Crit. Care Med. 2011, 183, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J.D. Long-term air pollution exposure and cardio-respiratory mortality: A review. Environ. Health 2013, 12, 43. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhang, L.-W.; Huang, J.-J.; Song, F.-J.; Zhang, L.-P.; Qian, Z.-M.; Chen, K.-X.; Liu, Y.-M.; Chen, J.; Zhao, B.-X. Long-term exposure to urban air pollution and lung cancer mortality: A 12-year cohort study in Northern China. Sci. Total Environ. 2016, 571, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Goldberg, M.S.; Villeneuve, P.J. A systematic review of the relation between long-term exposure to ambient air pollution and chronic diseases. Rev. Environ. Health 2008, 23, 243–297. [Google Scholar] [PubMed]
- Zhao, R.; Chen, S.; Wang, W.; Huang, J.; Wang, K.; Liu, L.; Wei, S. The impact of short-term exposure to air pollutants on the onset of out-of-hospital cardiac arrest: A systematic review and meta-analysis. Int. J. Cardiol. 2017, 226, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Zhang, B.; Ke, W.; Feng, B.; Lin, H.; Xiao, J.; Zeng, W.; Li, X.; Tao, J.; Yang, Z.; et al. Associations of short-term and long-term exposure to ambient air pollutants with hypertension: A systematic review and meta-analysis. Hypertension 2016, 68, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Hystad, P.; Villeneuve, P.J.; Goldberg, M.S.; Crouse, D.L.; Johnson, K. Canadian Cancer Registries Epidemiology Research Group. Exposure to traffic-related air pollution and the risk of developing breast cancer among women in eight Canadian provinces: A case-control study. Environ. Int. 2015, 74, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Yang, C.; Li, J.; Chen, R.; Chen, B.; Gu, D.; Kan, H. Association between long-term exposure to outdoor air pollution and mortality in China: A cohort study. J. Hazard. Mater. 2011, 186, 1594–1600. [Google Scholar] [CrossRef] [PubMed]
- Dockery, D.W.; Pope, C.A.; Xu, X.; Spengler, J.D.; Ware, J.H.; Fay, M.E.; Ferris, B.G., Jr.; Speizer, F.E. An association between air pollution and mortality in six U.S. cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A.; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 2002, 287, 1132–1141. [Google Scholar] [CrossRef] [PubMed]
- Padilla, C.M.; Kihal-Talantikite, W.; Vieira, V.M.; Rossello, P.; Le Nir, G.; Zmirou-Navier, D.; Deguem, D. Air quality and social deprivation in four French metropolitan areas—A localized spatio-temporal environmental inequality analysis. Environ. Res. 2014, 134, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Davis, D.A.; Bortolato, M.; Godar, S.C.; Sander, T.K.; Iwata, N.; Pakbin, P.; Shih, J.C.; Berhane, K.; McConnell, R.; Sioutas, C.; et al. Prenatal exposure to urban air nanoparticles in mice causes altered neuronal differentiation and depression-like responses. PLoS ONE 2013. [Google Scholar] [CrossRef] [PubMed]
- Fonken, L.K.; Xu, X.; Weil, Z.M.; Chen, G.; Sun, Q.; Rajagopalan, S.; Nelson, N.J. Air pollution impairs cognition, provokes depressive-like behaviors and alters hippocampal cytokine expression and morphology. Mol. Psychiatry 2011, 16, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.-H.; Kim, H.; Kim, J.H.; Bae, S.; Park, H.Y.; Hong, Y.-C. Air pollution and symptoms of depression in elderly adults. Environ. Health Perspect. 2012, 120, 1023–1028. [Google Scholar] [CrossRef] [PubMed]
- Szyszkowicz, M.; Rowe, B.H.; Colman, I. Air pollution and daily emergency department visits for depression. Int. J. Occup. Med. Environ. Health 2009, 22, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Perera, F.P.; Tang, D.; Wang, S.; Vishnevetsky, J.; Zhang, B.; Diaz, D.; Camann, D.; Rauh, V. Prenatal polycyclic aromatic hydrocarbon (PAH) exposure and child behavior at age 6–7 years. Environ. Health Perspect. 2012, 120, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Yi, O.; Kim, H. The role of differences in individual and community attributes in perceived air quality. Sci. Total Environ. 2012, 425, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Rotton, J.; Frey, J. Psychological costs of air pollution: Atmospheric conditions, seasonal trends, and psychiatric emergencies. Popul. Environ. 1984, 7, 3–16. [Google Scholar] [CrossRef]
- Bullinger, M. Psychological effects of air pollution on healthy residents a time-series approach. J. Environ. Psychol. 1989, 9, 10–18. [Google Scholar] [CrossRef]
- Martin, R.A.; Kazarian, S.S.; Breiter, H.J. Perceived stress, life events, dysfunctional attitudes, and depression in adolescent psychiatric inpatients. J. Psychopathol. Behav. Assess. 1995, 17, 81–95. [Google Scholar] [CrossRef]
- Johnson, B.B. Gender and race in beliefs about outdoor air pollution. Risk Anal. 2002, 22, 725–738. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, J.M.; Pijawka, K.D. Public concern for air quality: Explaining change in Toronto, Canada, 1967–1978. Int. J. Environ. Stud. 1982, 20, 17–26. [Google Scholar] [CrossRef]
- Bickerstaff, K.; Walker, G. Public understandings of air pollution: The ‘localisation’ of environmental risk. Glob. Environ. Chang. 2001, 11, 133–145. [Google Scholar] [CrossRef]
- Elliott, S.J.; Cole, D.C.; Krueger, P.; Voorberg, N.; Wakefield, S. The power of perception: Health risk attributed to air pollution in an urban industrial neighbourhood. Risk Anal. 1999, 19, 621–634. [Google Scholar] [CrossRef] [PubMed]
- Oglesby, L.; Kunzli, N.; Monn, C.; Schindler, C.; Ckermann-Liebrich, U.; Leuenberger, P. Validity of annoyance scores for estimation of long term air pollution exposure in epidemiologic studies: The Swiss Study on Air Pollution and Lung Diseases in Adults (SAPALDIA). Am. J. Epidemiol. 2000, 152, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Forsberg, B.; Stjernberg, N.; Wall, S. People can detect poor air quality well below guideline concentrations: A prevalence study of annoyance reactions and air pollution from traffic. Occup. Environ. Med. 1997, 54, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Williams, I.D.; Bird, A. Public perceptions of air quality and quality of life in urban and suburban areas of London. J. Environ. Monit. 2003, 5, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Jacquemin, B.; Sunyer, J.; Forsberg, B.; Götschi, T.; Bayer-Oglesby, L.; Ackermann-Liebrich, U.; de Marco, R.; Heinrich, J.; Jarvis, D.; Künzli, K.T.N. Annoyance due to air pollution in Europe. Int. J. Epidemiol. 2007, 36, 809–820. [Google Scholar] [CrossRef] [PubMed]
- Rotko, T.; Oglesby, L.; Kunzli, N.; Carrer, P.; Nieuwenhuijsen, M.J.; Jantunen, M. Determinants of perceived air pollution annoyance and association between annoyance scores and air pollution (PM2.5, NO2) concentrations in the European EXPOLIS study. Atmos. Environ. 2002, 36, 4593–4602. [Google Scholar] [CrossRef]
- Hillier, D. Communicating Health Risks to the Public: A Global Perspective; Gower: Aldershot, UK, 2006. [Google Scholar]
- Egondi, T.; Kyobutungi, C.; Ng, N.; Muindi, K.; Oti, S.; van de Vijver, S.; Ettarh, R.; Rocklöv, J. Community perceptions of air pollution and related health risks in Nairobi slums. Int. J. Environ. Res. Public Health 2013, 10, 4851–4868. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.; Popham, F. Greenspace, urbanity and health: Relationships in England. J. Epidemiol. Community Health 2007, 61, 681–683. [Google Scholar] [CrossRef] [PubMed]
- Lalloué, B.; Monnez, J.-M.; Padilla, C.; Kihal, W.; Zmirou-Navier, D.; Deguen, S. Data analysis techniques: A tool for cumulative exposure assessment. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Généreux, M.; Auger, N.; Goneau, M.; Daniel, M. Neighbourhood socioeconomic status, maternal education and adverse birth outcomes among mothers living near highways. J. Epidemiol. Community Health 2008, 62, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Beckerman, B.; Jerrett, M.; Brook, J.R.; Verma, D.K.; Arain, M.A.; Finkelstein, M.M. Correlation of nitrogen dioxide with other traffic pollutants near a major expressway. Atmos. Environ. 2008, 42, 275–290. [Google Scholar] [CrossRef]
- Gilbert, N.L.; Woodhouse, S.; Stieb, D.M.; Brook, J.R. Ambient nitrogen dioxide and distance from a major highway. Sci. Total Environ. 2003, 312, 43–46. [Google Scholar] [CrossRef]
- European Commission. Directive 2002/49/EC of the European Parliament and of the Council of 25 June 2002 Relating to the Assessment and Management of Environmental Noise. Available online: http://eur-lex.europa.eu/legal-content/en/TXT/?uri=CELEX%3A32002L0049 (accessed on 4 December 2017).
- World Health Organization (WHO). Guidelines for Community Noise, Geneva [Internet], 1999. Available online: http://www.who.int/docstore/peh/noise/guidelines2.html (accessed on 1 September 2017).
- European Environment Agency. Good Practice Guide on Noise Exposure and Potential Health Effects; EEA Technical Report No 11/2010; European Environment Agency: Copenhagen, Denmark, 2010. [Google Scholar]
- Kihal-Talantikite, W.; Padilla, C.M.; Lalloue, B.; Rougier, C.; Defrance, J.; Zmirou-Navier, D.; Deguen, S. An exploratory spatial analysis to assess the relationship between deprivation, noise and infant mortality: An ecological study. Environ. Health 2013, 12, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kihal-Talantikite, W.; Padilla, C.M.; Lalloué, B.; Gelormini, M.; Zmirou-Navier, D.; Deguen, S. Green space, social inequalities and neonatal mortality in France. BMC Pregnancy Childbirth 2013, 13, 191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lalloué, B.; Monnez, J.-M.; Padilla, C.; Kihal, W.; Le Meur, N.; Zmirou-Navier, D.; Deguen, S. A statistical procedure to create a neighborhood socioeconomic index for health inequalities analysis. Int. J. Equity Health 2013, 12, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, M.; O’Neill, M.; Cifuentes, L.; Braga, A.; Green, C.; Nweke, A.; Rogat, J.; Sibold, K. Challenges and recommendations for the study of socioeconomic factors and air pollution health effects. J. Environ. Sci. Policy 2005, 8, 525–533. [Google Scholar] [CrossRef]
- Klaeboe, R.; Amundsen, A.H.; Fyhri, A. Annoyance from vehicular air pollution: A comparison of European exposure-response relationships. Atmos. Environ. 2008, 42, 7689–7694. [Google Scholar] [CrossRef]
- Semenza, J.C.; Wilson, D.J.; Parra, J.; Bontempo, B.D.; Hart, M.; Sailor, D.J.; George, L.A. Public perception and behavior change in relationship to hot weather and air pollution. Environ. Res. 2008, 107, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Liu, F.; Lu, Y.; Mao, Z.; Lu, H.; Wu, Y.; Chu, Y.; Yu, L.; Liu, Y.; Ren, M.; et al. Factors affecting parent’s perception on air quality-from the individual to the community level. Int. J. Environ. Res. Public Health 2016, 13, 493. [Google Scholar] [CrossRef] [PubMed]
- Badland, H.M.; Duncan, M.J. Perceptions of air pollution during the work-related commute by adults in Queensland, Australia. Atmos. Environ. 2009, 43, 5791–5795. [Google Scholar] [CrossRef]
- Kohlhuber, M.; Mielck, A.; Weiland, S.K.; Bolte, G. Social inequality in perceived environmental exposures in relation to housing conditions in Germany. Environ. Res. 2006, 101, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Lercher, P.; Schmitzberger, R.; Kofler, W. Perceived traffic air pollution, associated behavior and health in an alpine area. Sci. Total Environ. 1995, 169, 71–74. [Google Scholar] [CrossRef]
- Bengtsson, S.; Berglund, H.; Gulyas, B.; Cohen, E.; Savic, I. Brain activation during odor perception in males and females. Neuroreport 2001, 12, 2027–2033. [Google Scholar] [CrossRef] [PubMed]
- Brody, S.D.; Peck, B.M.; Highfield, W.E. Examining localized patterns of air quality perception in Texas: A spatial and statistical analysis. Risk Anal. 2004, 24, 1561–1574. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Frequency | % |
|---|---|---|
| Gender | ||
| Men | 440 | 44.0 |
| Women | 560 | 56.0 |
| Age (years) | ||
| 18–29 | 147 | 14.7 |
| 30–44 | 220 | 22.0 |
| 45–59 | 251 | 25.1 |
| 60–74 | 229 | 22.9 |
| >74 | 153 | 15.3 |
| Family status | ||
| Live with a partner without children | 309 | 30.9 |
| Live with a partner with children | 287 | 28.7 |
| Live alone without children | 257 | 25.7 |
| Live with parent | 84 | 8.4 |
| Single parent families | 56 | 5.6 |
| Live with a roommate | 7 | 0.7 |
| Level of education | ||
| Low level | 384 | 38.4 |
| Intermediate level | 321 | 32.1 |
| High level | 295 | 29.5 |
| Occupational status | ||
| Retired | 339 | 33.9 |
| Student | 61 | 6.1 |
| Employed | 460 | 46.0 |
| Unemployed-inactive | 140 | 14.0 |
| Housing (1 missing value) | ||
| House | 258 | 25.8 |
| Apartment | 739 | 74.0 |
| Other type of housing | 2 | 0.2 |
| Heating mode (4 missing values) | ||
| Wood | 37 | 3.7 |
| Fuel oil | 76 | 7.6 |
| Electric | 251 | 25.2 |
| Gas | 592 | 59.4 |
| Other | 40 | 4.0 |
| Number of years that they have lived in the metropolitan area (4 missing values) | ||
| <1 year | 8 | 0.8 |
| 1–2 years | 14 | 1.4 |
| 2–4 years | 77 | 7.7 |
| 5–9 years | 121 | 12.1 |
| ≥10 years | 776 | 77.9 |
| Respiratory health problem (3 missing values) | ||
| no | 731 | 73.3 |
| yes | 263 | 26.4 |
| Do not know | 3 | 0.3 |
| Cardiovascular health problem | ||
| no | 912 | 91.2 |
| yes | 88 | 8.8 |
| Occupation | ||
| Tradespeople-Shopkeepers | 26 | 5.7 |
| Managers | 108 | 23.5 |
| Employees | 137 | 29.8 |
| Manual workers | 64 | 13.9 |
| Non-manual workers | 125 | 27.2 |
| Work location (1 missing value) | ||
| At home | 36 | 7.8 |
| In the municipality of residence | 187 | 48.6 |
| In a municipality of the Rhône-Alpes department | 192 | 90.4 |
| In a municipality not in the Rhône-Alpes department | 12 | 2.6 |
| Other place of work | 32 | 7.0 |
| Means of travel to work (37 missing values) | ||
| Public transportation (Bus, tramway, metro) | 91 | 21.5 |
| Car | 230 | 54.4 |
| Bicycle | 31 | 7.3 |
| Motorbike | 7 | 1.7 |
| By foot | 53 | 12.5 |
| Other | 11 | 2.6 |
| Questions | Answers | Frequency | % |
|---|---|---|---|
| Would you say that the quality of the air you breathe within your residential census block is good (3 missing values) | Yes totally agree | 228 | 22.9 |
| Somewhat agree | 471 | 47.2 | |
| Do not agree | 244 | 24.5 | |
| No opinion—do not know | 54 | 5.4 | |
| Would you ever consider living in another place where air quality is better (7 missing values) | Yes | 289 | 29.1 |
| No | 673 | 67.8 | |
| No opinion—do not know | 31 | 3.1 | |
| Are you aware of actions or interventions aimed at improving air quality in the Lyon MA (3 missing values) | Yes | 267 | 26.8 |
| No | 729 | 73.2 | |
| Would you say that you are satisfied with the place where you live | Yes totally agree | 472 | 47.2 |
| Somewhat agree | 460 | 46.0 | |
| Do not agree | 61 | 6.1 | |
| No opinion—do not know | 7 | 0.7 |
| (a) | ||||||
| Profile 1 (n = 31) | Profile 2 (n = 43) | Profile 3 (n = 48) | Profile 4 (n = 24) | |||
| Perceived Air quality | Totally agree | 67.74 | 4.65 | 20.83 | 12.50 | |
| Somewhat agree | 16.13 | 41.86 | 56.25 | 66.67 | ||
| Not agree | 6.45 | 51.16 | 22.92 | 16.67 | ||
| Do not know | 9.68 | 2.33 | 0.00 | 4.17 | ||
| Satisfaction with the residential place | Totally agree | 77.42 | 23.26 | 43.75 | 41.67 | |
| Somewhat agree | 16.13 | 60.47 | 56.25 | 58.33 | ||
| Not agree | 0.00 | 16.28 | 0.00 | 0.00 | ||
| Do not know | 6.45 | 0.00 | 0.00 | 0.00 | ||
| Living in another place | yes | 16.13 | 81.40 | 22.92 | 25.00 | |
| no | 83.87 | 18.60 | 64.58 | 66.67 | ||
| Do not know | 0.00 | 0.00 | 12.50 | 8.33 | ||
| Knowledge about air quality | yes | 35.48 | 23.26 | 27.08 | 29.17 | |
| no | 64.52 | 76.74 | 72.92 | 70.83 | ||
| (b) | ||||||
| Profile 1 (n = 121) | Profile 2 (n = 124) | Profile 3 (n = 121) | Profile 4 (n = 102) | |||
| Perceived Air quality | Totally agree | 28.10 | 0.00 | 33.06 | 15.69 | |
| Somewhat agree | 52.07 | 44.35 | 47.93 | 44.12 | ||
| Not agree | 16.53 | 54.03 | 10.74 | 34.31 | ||
| Do not know | 3.31 | 1.61 | 8.26 | 5.88 | ||
| Satisfaction with the residential place | Totally agree | 50.41 | 12.90 | 57.02 | 39.22 | |
| Somewhat agree | 48.76 | 70.16 | 38.84 | 51.96 | ||
| Not agree | 0.83 | 16.94 | 4.13 | 8.82 | ||
| Do not know | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Living in another place | yes | 28.93 | 65.32 | 20.66 | 42.16 | |
| no | 68.60 | 29.84 | 76.03 | 52.94 | ||
| Do not know | 2.48 | 4.84 | 3.31 | 4.90 | ||
| Knowledge about air quality | yes | 49.59 | 33.06 | 26.45 | 23.53 | |
| no | 50.41 | 66.94 | 73.55 | 76.47 | ||
| (c) | ||||||
| Profile 1 (n = 34) | Profile 2 (n = 99) | Profile 3 (n = 84) | Profile 4 (n = 103) | Profile 5 (n = 35) | ||
| Perceived Air quality | Totally agree | 29.41 | 59.60 | 23.81 | 1.94 | 0.00 |
| Somewhat agree | 41.18 | 27.27 | 59.52 | 73.79 | 20.00 | |
| Not agree | 29.41 | 6.06 | 11.90 | 11.65 | 80.00 | |
| Do not know | 0.00 | 7.07 | 4.76 | 12.62 | 0.00 | |
| Satisfaction with the residential place | Totally agree | 38.24 | 268.57 | 44.05 | 52.43 | 17.14 |
| Somewhat agree | 55.88 | 11.43 | 54.76 | 47.57 | 40.00 | |
| Not agree | 5.88 | 0.00 | 1.19 | 0.00 | 37.14 | |
| Do not know | 0.00 | 2.86 | 0.00 | 0.00 | 5.71 | |
| Living in another place | yes | 17.65 | 1.01 | 14.29 | 4.85 | 57.14 |
| no | 79.41 | 98.99 | 85.71 | 92.23 | 40.00 | |
| Do not know | 2.94 | 0.00 | 0.00 | 2.91 | 2.86 | |
| Knowledge about air quality | yes | 23.53 | 5.15 | 44.05 | 11.65 | 8.57 |
| no | 76.47 | 94.85 | 55.95 | 88.35 | 91.43 | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deguen, S.; Padilla, M.; Padilla, C.; Kihal-Talantikite, W. Do Individual and Neighborhood Characteristics Influence Perceived Air Quality? Int. J. Environ. Res. Public Health 2017, 14, 1559. https://doi.org/10.3390/ijerph14121559
Deguen S, Padilla M, Padilla C, Kihal-Talantikite W. Do Individual and Neighborhood Characteristics Influence Perceived Air Quality? International Journal of Environmental Research and Public Health. 2017; 14(12):1559. https://doi.org/10.3390/ijerph14121559
Chicago/Turabian StyleDeguen, Séverine, Manon Padilla, Cindy Padilla, and Wahida Kihal-Talantikite. 2017. "Do Individual and Neighborhood Characteristics Influence Perceived Air Quality?" International Journal of Environmental Research and Public Health 14, no. 12: 1559. https://doi.org/10.3390/ijerph14121559
APA StyleDeguen, S., Padilla, M., Padilla, C., & Kihal-Talantikite, W. (2017). Do Individual and Neighborhood Characteristics Influence Perceived Air Quality? International Journal of Environmental Research and Public Health, 14(12), 1559. https://doi.org/10.3390/ijerph14121559