
Urban Place and Health Equity: Critical Issues and Practices


{kind=link}
{kind=link}
Abstract
:1. Introduction
“Health inequities are the result of the circumstances in which people grow, live, work and age, and the health systems they can access, which in turn are shaped by broader political, social and economic forces. They are not distributed randomly, but rather show a consistent pattern across the population, often by socioeconomic status or geographical location. No city—large or small, rich or poor, east or west, north or south—has been shown to be immune to the problem of health inequity.”[4]
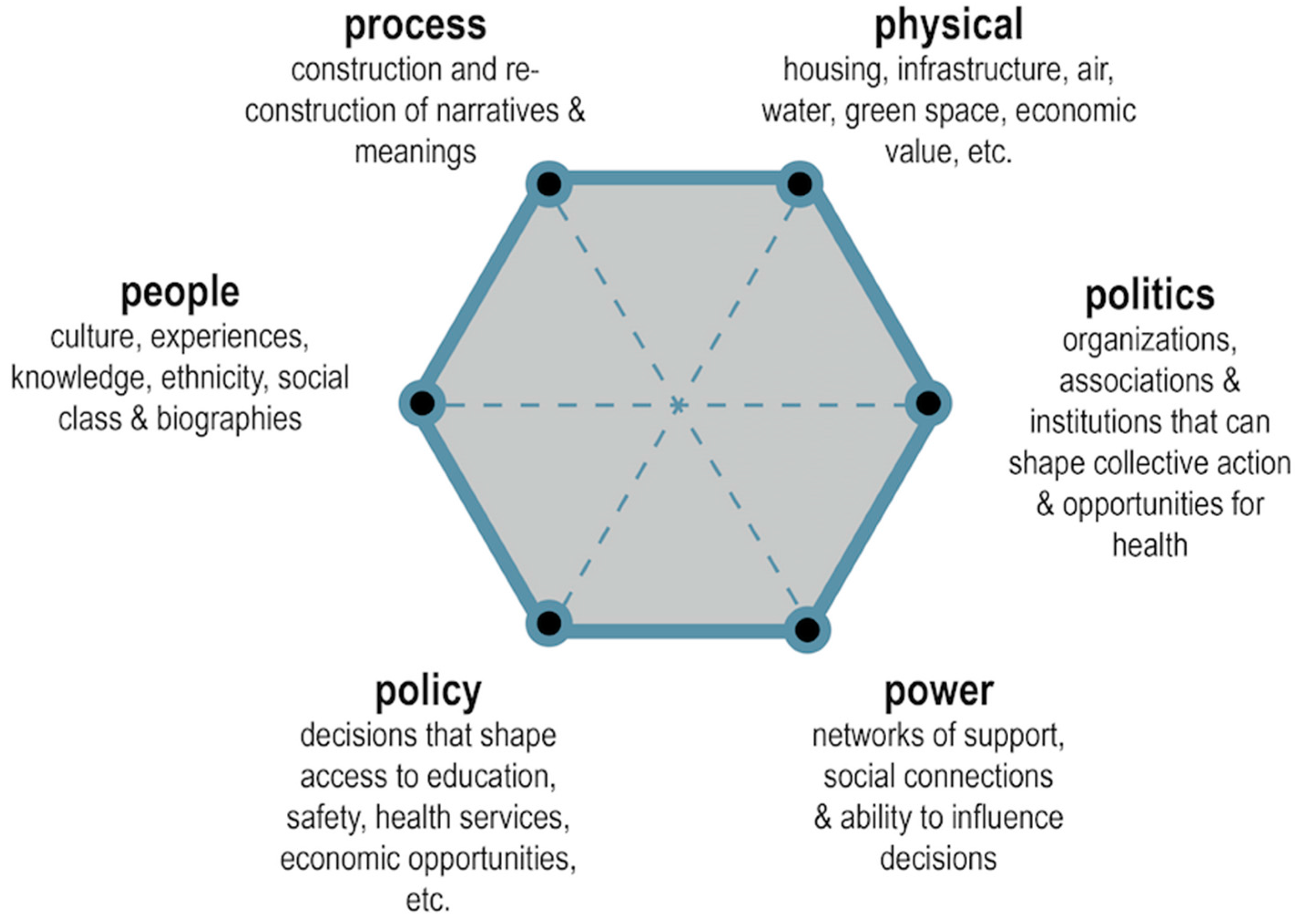
2. Urban Places: Beyond the Built Environment
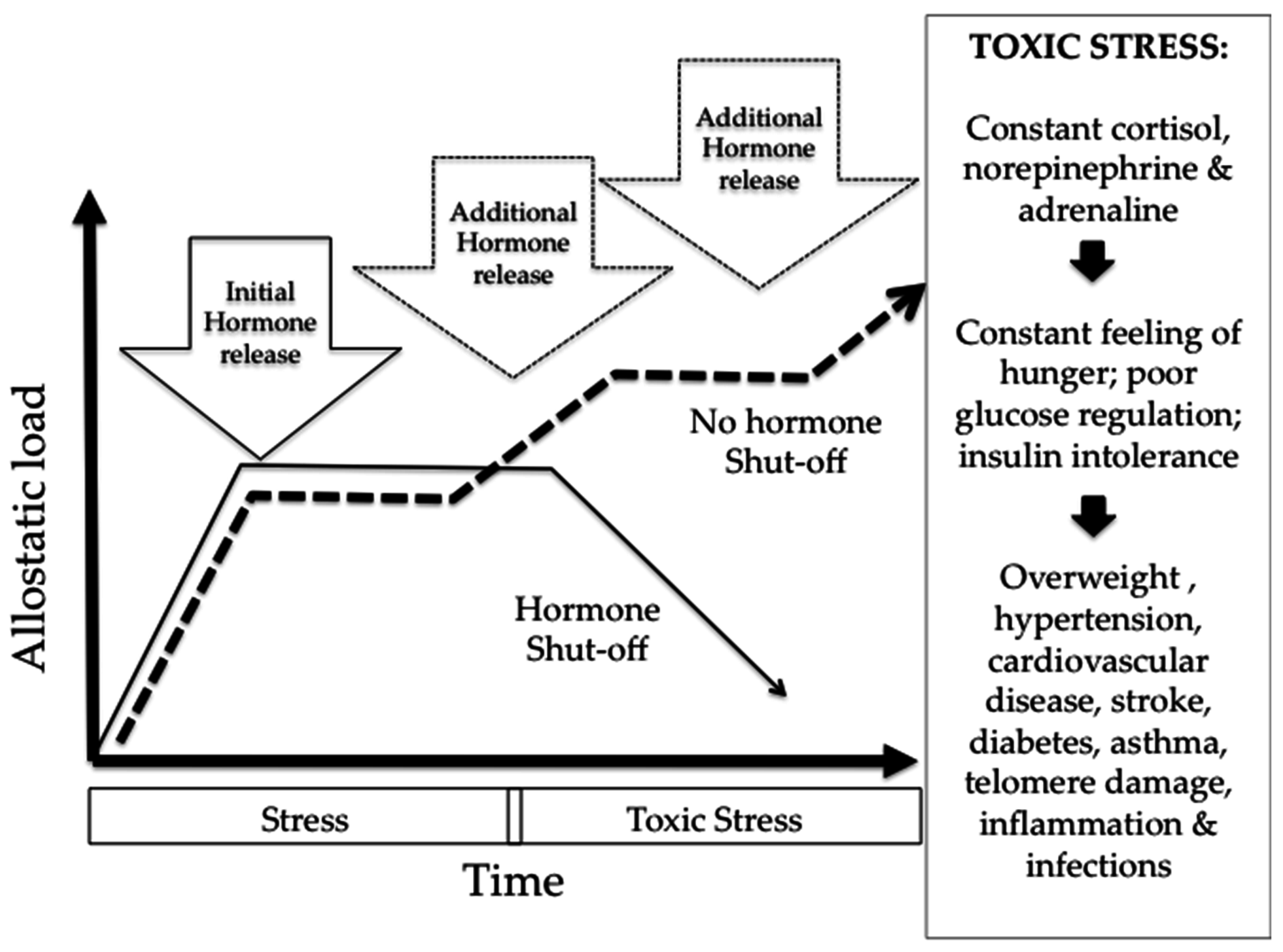
3. Urban Place, Health Equity and Biologic Embodiment
4. From Analysis to Practice for Urban Place and Health Equity
4.1. Community-Led Mapping
4.2. Health Equity in All Urban Polices
4.3. Urban Ecosystem Services and Human Health
4.4. Integrated Participatory Slum Upgrading
5. Conclusions
Conflicts of Interest
References
- UN Habitat/World Health Organization. Global Report on Urban Health. Kobe, Japan. Available online: http://www.who.int/kobe_centre/measuring/urban-global-report/en/ (accessed on 29 June 2016).
- Braveman, P.; Gruskin, S. Defining Equity in Health. J. Epidemiol. Commun. Health 2003, 57, 254–258. [Google Scholar] [CrossRef]
- Corburn, J. Healthy City Planning: From Neighbourhood to National Health Equity; Routledge: London, UK, 2013. [Google Scholar]
- UN Habitat/World Health Organisation (WHO). Hidden Cities: Unmasking and Overcoming Health Inequities in Urban Settings. Kobe Centre, Japan. Available online: http://www.who.int/kobe_centre/publications/hidden_cities2010/en/ (accessed on 7 September 2016).
- Corburn, J. Toward the Healthy City: People, Places and the Politics of Urban Planning; MIT Press: Cambridge, MA, USA, 2009. [Google Scholar]
- WHO. Environmental Health. Geneva. Available online: http://www.who.int/topics/environmental_health/en/ (accessed 31 October 2016).
- Macintyre, S.; Ellaway, A.; Cummins, S. Place effects on health: How can we conceptualise, operationalise and measure them? Soc. Sci. Med. 2002, 55, 125–139. [Google Scholar] [CrossRef]
- Cronon, W. The Trouble with Wilderness or Getting Back to the Wrong Nature. In Uncommon Ground: Rethinking the Human Place in Nature; Cronon, W., Ed.; W.W. Norton & Co.: New York, NY, USA, 1995; pp. 69–90. [Google Scholar]
- Anguelovski, I. New Directions in Urban Environmental Justice: Rebuilding Community, Addressing Trauma, and Remaking Place. J. Plan. Educ. Res. 2013, 33, 160–175. [Google Scholar] [CrossRef]
- Cummins, S.; Curtis, S.; Diez-Roux, A.V.; Macintyre, S. Understanding and Representing “Place” in Health Research: A Relational Approach. Soc. Sci. Med. 2007, 65, 1825–1838. [Google Scholar] [CrossRef]
- Díez-Roux, A.V.; Mair, C. Neighborhoods and health. Ann. N. Y. Acad. Sci. 2010, 1186, 125–145. [Google Scholar] [CrossRef] [PubMed]
- Escobar, A. Culture Sits in Places: Reflections on Globalism and Subaltern Strategies of Localization. Political Geogr. 2001, 20, 139–174. [Google Scholar] [CrossRef]
- Smith, S.; Easterlow, D. The strange geography of health inequalities. Trans. Inst. Br. Geogr. 2005, 30, 173–190. [Google Scholar] [CrossRef]
- Ewing, R. Can the physical environment determine physical activity levels? Exerc. Sport Sci. Rev. 2005, 33, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Ann. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [PubMed]
- Laraia, B.A.; Siega-Riz, A.M.; Kaufman, J.S.; Jones, S.J. Proximity of supermarkets is positively associated with diet quality index for pregnancy. Prev. Med. 2004, 39, 869–875. [Google Scholar] [CrossRef]
- Black, C.; Moon, G.; Baird, J. Dietary inequalities: What is the evidence for the effect of the neighbourhood food environment? Health Place 2013, 27, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Healey, P. Urban Complexity and Spatial Strategies: Towards a Relational Planning for Our Times; Routledge: London, UK, 2007. [Google Scholar]
- Beil, K.; Hanes, D. The influence of urban natural and built environments on physiological and psychological measures of stress—A pilot study. Int. J. Environ. Res. Public Health 2013, 10, 1250–1267. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N. Embodiment: A Conceptual Glossary for Epidemiology. J. Epidemiol. Commun. Health 2005, 59, 350–355. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S.; Gianaros, P.J. Central role of the brain in stress and adaptation: Links to socioeconomic status, health, and disease. Ann. N. Y. Acad. Sci. 2010, 1186, 190–222. [Google Scholar] [CrossRef] [PubMed]
- Price, L.H.; Kao, H.T.; Burgers, D.E.; Carpenter, L.L.; Tyrka, A.R. Telomeres and early-life stress: An overview. Biol. Psychiatry 2013, 73, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Gee, G.; Walsemann, K.; Brondolo, E. A Life Course Perspective on How Racism May Be Related to Health Inequities. Am. J. Public Health 2012, 102, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Payne-Sturges, D.C.; Korfmacher, K.S.; Cory-Slechta, D.A.; Jimenez, M.; Symanski, E.; Carr Shmool, J.L.; Dotson-Newman, O.; Clougherty, J.E.; French, R.; Levy, J.I.; et al. Engaging communities in research on cumulative risk and social stress-environment interactions: Lessons learned from EPA’s STAR Program. Environ. Justice 2015, 8, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Corbett, J.; Rambaldi, G.; Kyem, P.; Weiner, D.; Olson, R.; Muchemi, J.; McCall, M.; Chambers, R. Mapping for Change: Practice, Technologies and Communication. Participatory Learning and Action No. 54. Available online: http://pubs.iied.org/pdfs/14507IIED.pdf (accessed on 9 December 2016).
- Corburn, J.; Karanja, I. Informal settlements and a relational view of health in Nairobi, Kenya: Sanitation, gender and dignity. Health Promot. Int. 2014, 31, 258–269. [Google Scholar] [CrossRef] [PubMed]
- Rocha, I. Mapeamento Digital Liderado por Adolescentes e Jovens: Guia do Facilitador. Rio de Janeiro: Cedaps, 2014. Available online: http://www.unicef.org/brazil/pt/guia_mapeamento_pcu1316.pdf (accessed on 11 September 2016).
- Ollila, E. Health in all policies: From rhetoric to action. Scand. J. Public Health 2011, 39 (Suppl. S6), S11–S18. [Google Scholar] [CrossRef] [PubMed]
- Pastor, M.; Morello-Frosch, R. Integrating Public Health and Community Development to Tackle Neighborhood Distress and Promote Well-being. Health Affairs 2014, 33, 1890–1896. [Google Scholar] [CrossRef] [PubMed]
- Wernham, A.; Teutsch, S.M. Health in All Policies for Big Cities. Public Health Manag. Pract. 2015, 21 (Suppl. S1), S56–S65. [Google Scholar] [CrossRef] [PubMed]
- Corburn, J.; Curl, S.; Arredondo, G.; Malgon, J. Health in All Urban Policy: City Services Through the Prism of Health. J. Urban Health 2014, 91, 623–636. [Google Scholar] [CrossRef] [PubMed]
- Serrano, E.; Larrañaga, I.; Morteruel, M.; de Ros, M.D.; Basterrechea, M.; Martinez, D.; Aldasoro, E.; Bacigalupe, A. Urban regeneration as population health intervention: A health impact assessment in the Bay of Pasaia (Spain). Int. J. Equity Health 2016, 15, 145. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Sustainable Development Goals. Available online: http://www.un.org/sustainabledevelopment/cities/ (accessed on 30 August 2016).
- Elmqvist, T.; Setälä, H.; Handel, S.N.; Van Der Ploeg, S.; Aronson, J.; Blignaut, J.N.; Gómez-Baggethun, E.; Nowak, D.J.; Kronenberg, J.; De Groot, R. Benefits of restoring ecosystem services in urban areas. Curr. Opin. Environ. Sustain. 2015, 14, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Gascon, M.; Triguero-Mas, M.; Martínez, D.; Dadvand, P.; Forns, J.; Plasència, A.; Nieuwenhuijsen, M.J. Mental health benefits of long-term exposure to residential green and blue spaces: A systematic review. Int. J. Environ. Res. Public Health 2015, 12, 4354–4379. [Google Scholar] [CrossRef] [PubMed]
- Sandifer, P.A.; Sutton-Grier, A.E.; Ward, B.P. Exploring connections among nature, biodiversity, ecosystem services, and human health and well-being: Opportunities to enhance health and biodiversity conservation. Ecosyst. Serv. 2015, 12, 1–15. [Google Scholar] [CrossRef]
- Soleri, D.; Long, J.; Ramirez-Andreotta, M.; Eitemiller, R.; Pandya, R. Finding Pathways to More Equitable and Meaningful Public-Scientist Partnerships. Citiz. Sci. Theory Pract. 2016, 1, 1–11. [Google Scholar]
- Corburn, J.; Riley, L. Slum Health: From the Cell to the Street; University of California Press: Berkeley, CA, USA, 2016. [Google Scholar]
- Muggah, R. Deconstructing the fragile city: Exploring insecurity, violence and resilience. Environ. Urban. 2014, 26, 345–358. [Google Scholar] [CrossRef]
- Ezeh, A.; Oyebode, O.; Satterthwaite, D.; Chen, Y.F.; Ndugwa, R.; Sartori, J.; Mberu, B.; Melendez-Torres, G.J.; Haregu, T.; Watson, S.I.; et al. The history, geography, and sociology of slums and the health problems of people who live in slums. Lancet 2016. [Google Scholar] [CrossRef]
- Rojas, E. Building Cities: Neighborhood Upgrading and Urban Quality of Life; Inter-American Development Bank: Washington, DC, USA, 2010. [Google Scholar]
- Butala, N.M.; vanRooyen, M.J.; Patel, R.B. Improved Health Outcomes in Urban Slums through Infrastructure Upgrading. Soc. Sci. Med. 2010, 71, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Violence Prevention through Urban Upgrading. City of Cape Town, South Africa. Available online: http://www.vpuu.org.za (accessed on 7 July 2016).
- Boonyabancha, S. Land for Housing the Poor by the Poor: Experiences from the Baan Mankong Nationwide Slum Upgrading Programme in Thailand. Environ. Urban. 2009, 21, 309–329. [Google Scholar] [CrossRef]


© 2017 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corburn, J. Urban Place and Health Equity: Critical Issues and Practices. Int. J. Environ. Res. Public Health 2017, 14, 117. https://doi.org/10.3390/ijerph14020117
Corburn J. Urban Place and Health Equity: Critical Issues and Practices. International Journal of Environmental Research and Public Health. 2017; 14(2):117. https://doi.org/10.3390/ijerph14020117
Chicago/Turabian StyleCorburn, Jason. 2017. "Urban Place and Health Equity: Critical Issues and Practices" International Journal of Environmental Research and Public Health 14, no. 2: 117. https://doi.org/10.3390/ijerph14020117
APA StyleCorburn, J. (2017). Urban Place and Health Equity: Critical Issues and Practices. International Journal of Environmental Research and Public Health, 14(2), 117. https://doi.org/10.3390/ijerph14020117