
Parental Supply of Alcohol in Childhood and Risky Drinking in Adolescence: Systematic Review and Meta-Analysis


Abstract
:1. Introduction
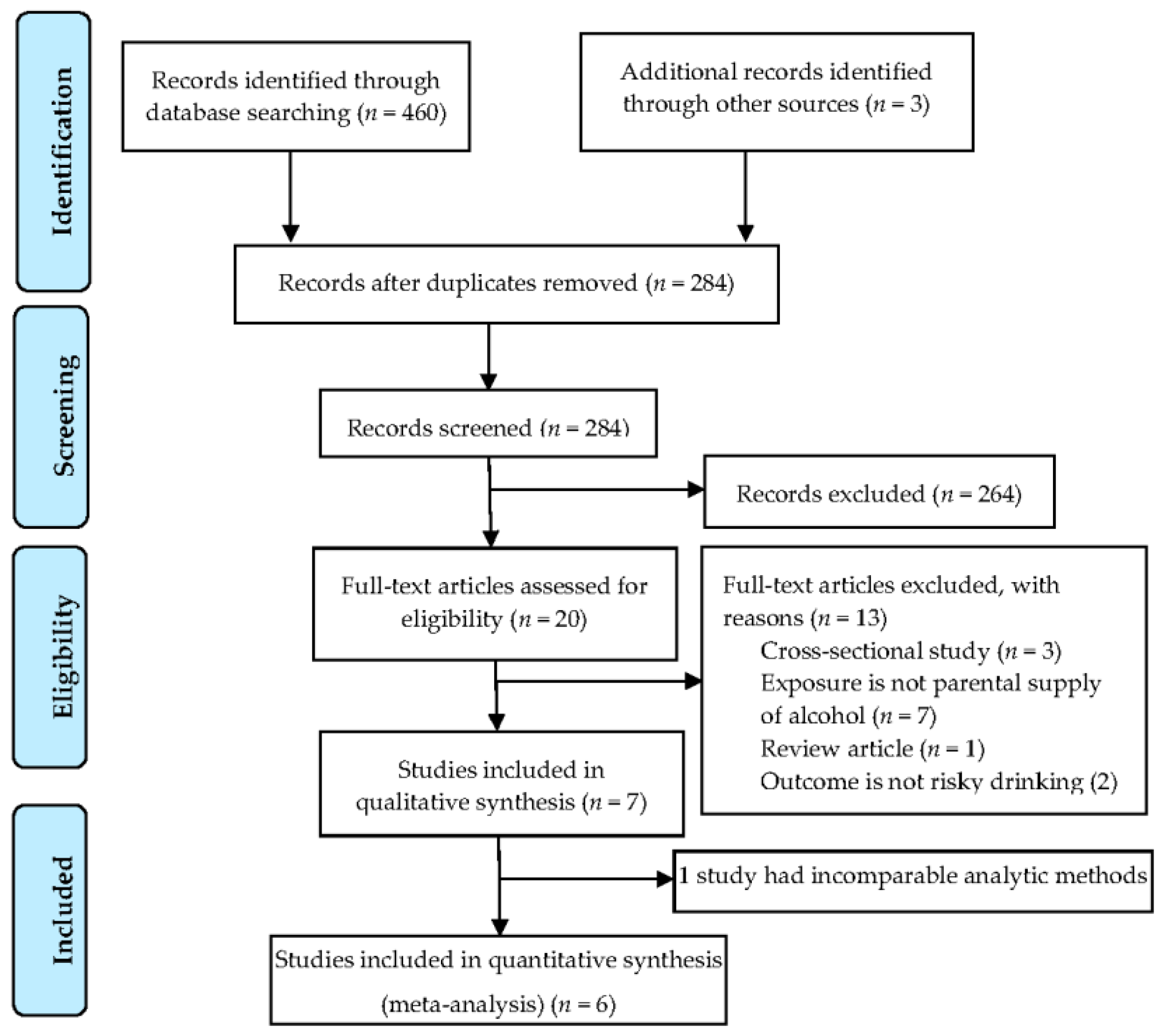
2. Materials and Methods
2.1. Selection and Eligibility Criteria
2.2. Search Strategy
2.3. Data Extraction and Validity Assessment
2.4. Statistical Analysis (Meta-Analysis)
3. Results
3.1. Study Characteristics
3.2. Summary of Study Findings
3.2.1. Drinking at Home or with Family
3.2.2. Drinking under Adult Supervision
3.2.3. Parental Supply and Offers of Alcohol
3.3. Assessment of Study Validity
3.3.1. Selection
3.3.2. Measurement of Exposure and Outcome
3.3.3. Confounding
3.3.4. Attrition
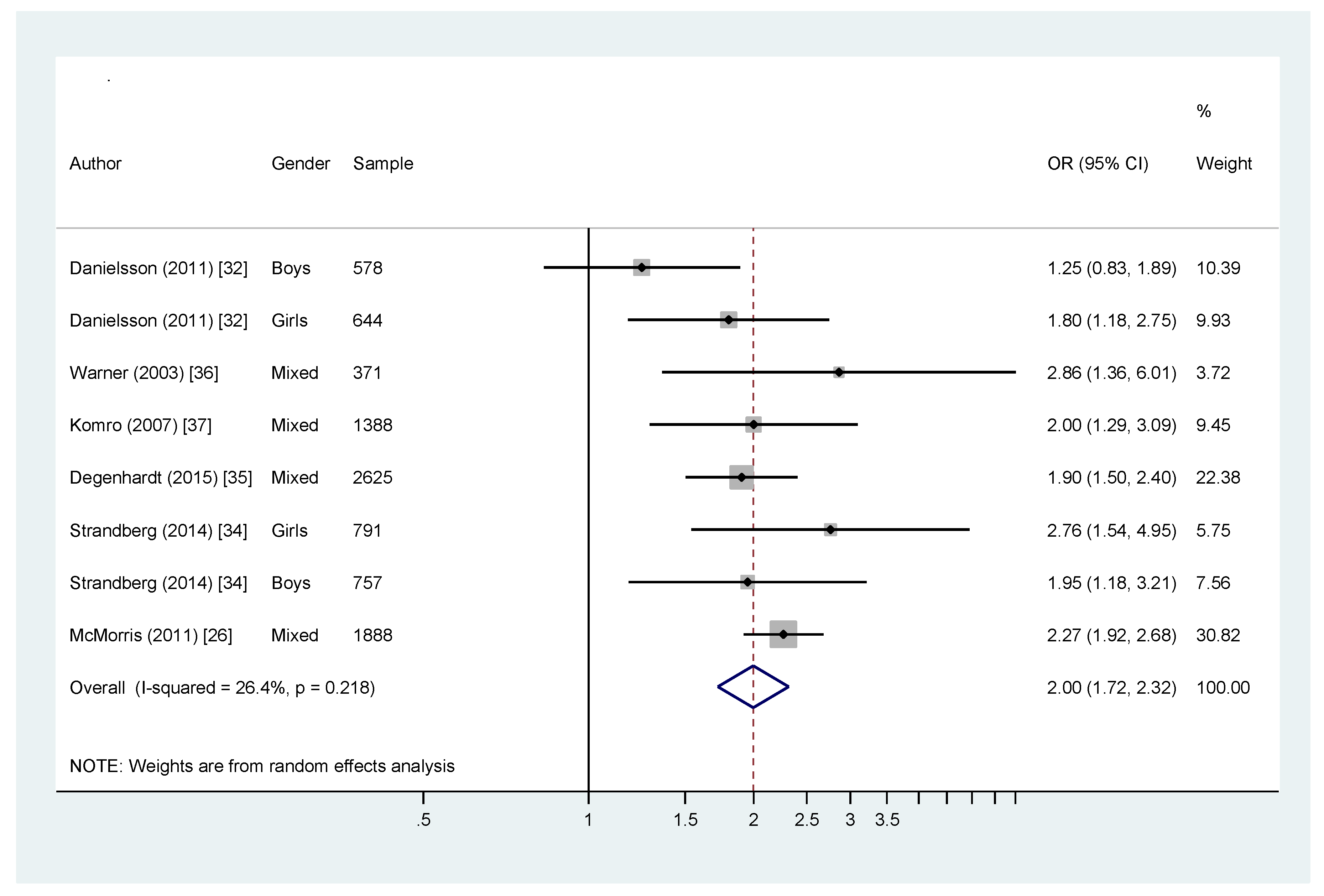
3.4. Meta-Analysis
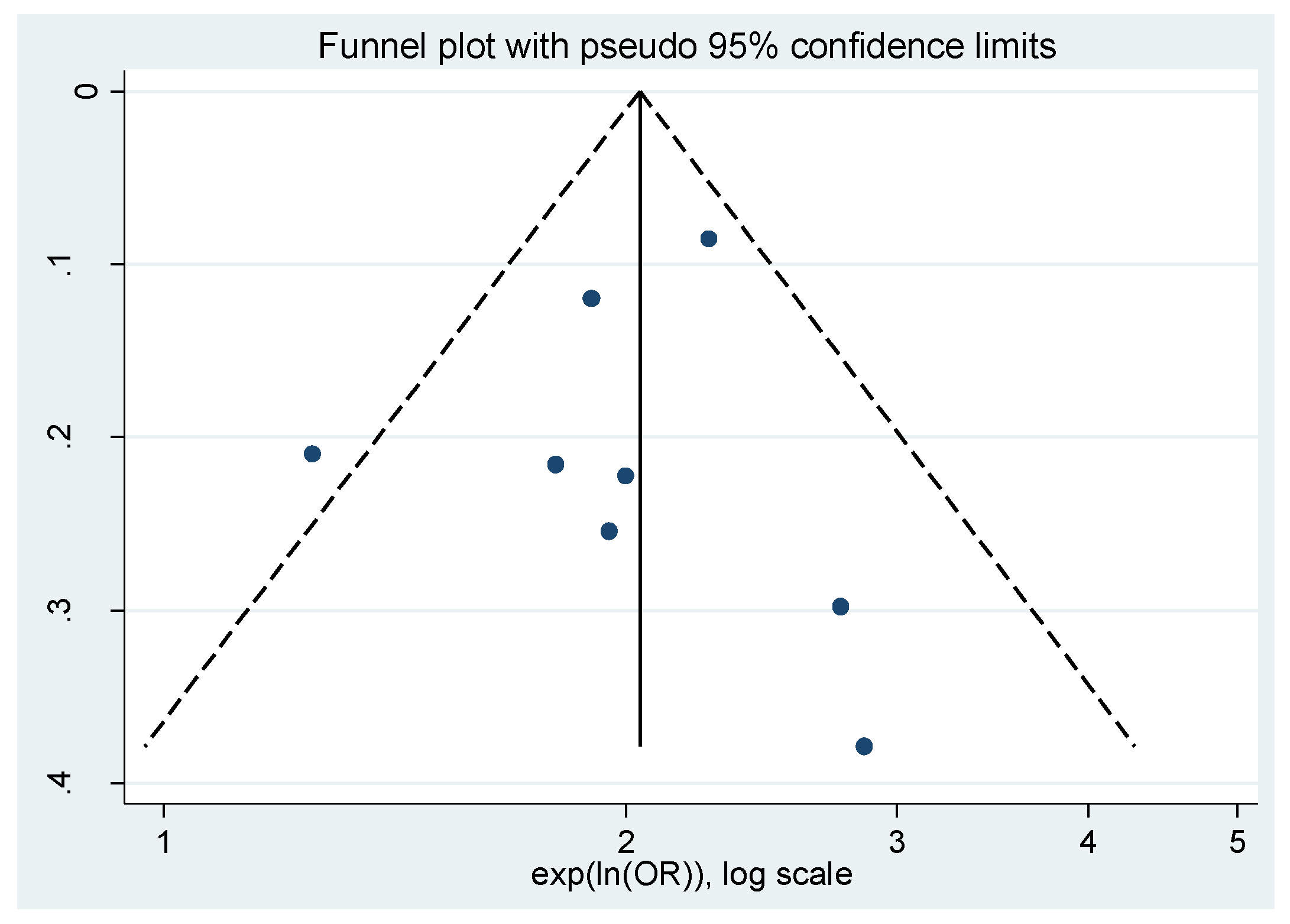
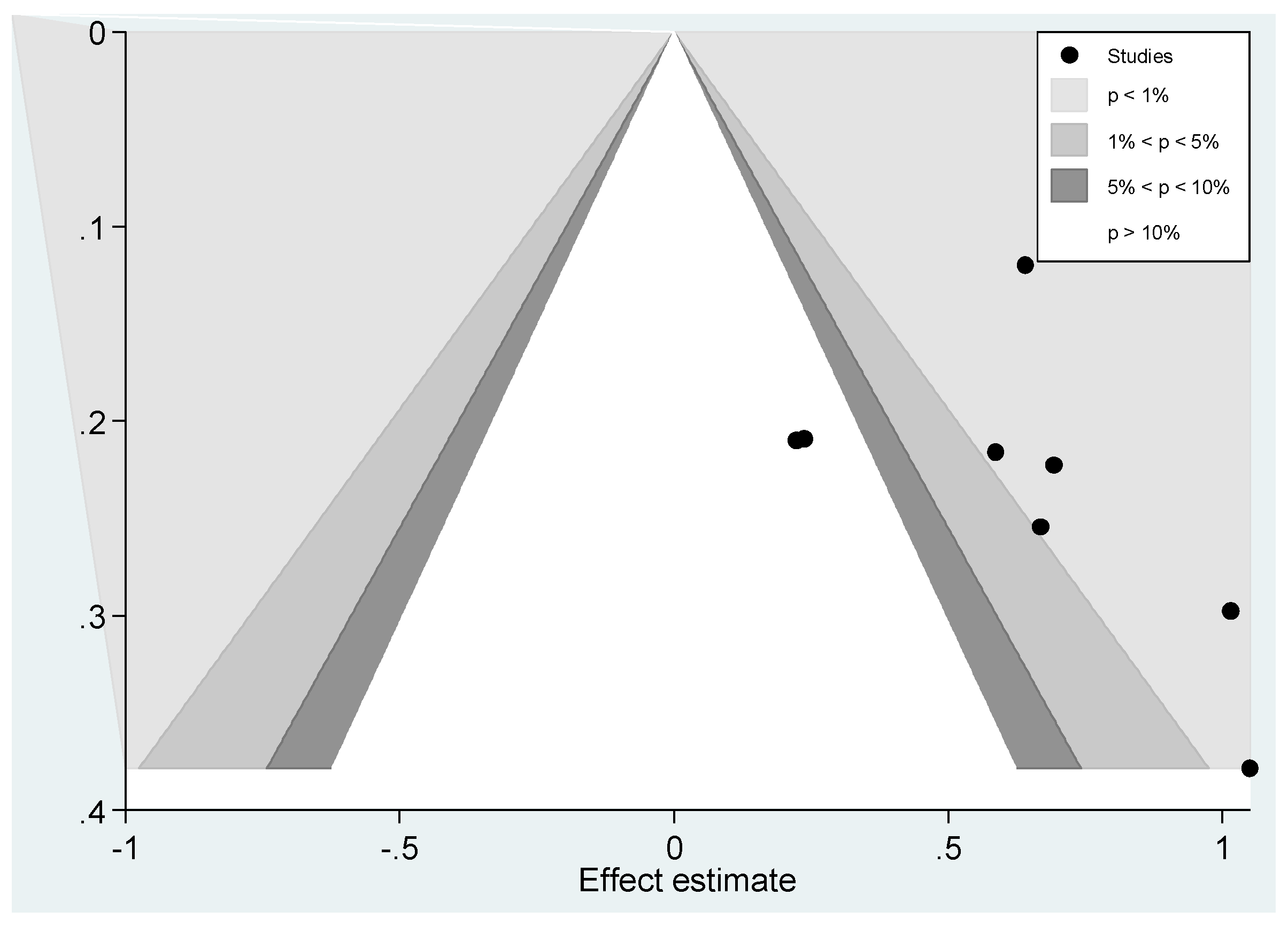
Publication Bias
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A. Parent Rules | B. Adolescent | C. Risky Drinking | D. Study Design |
|---|---|---|---|
| 1. ((parent* or mother* or father* or maternal* or guardian* or custodian*) adj5 (provision* or approv* or suppl* or influence* or permissive* or host* or offer or furnish or source* or allow* or permission* or permit or agree*)).mp. (33999) | 2. child*.mp. (2213989) 3. offspring.mp. (60119) 4. adolescen*.mp. (1373825) 5. famil*.mp. (1109647) 6. juvenil*.mp. (110083) 7. girl*.mp. (149109) 8. boy*.mp. (157168) 9. youth.mp. (48965) 10. pubescen*.mp. (2207) 11. teen*.mp. (30193) 12. young women.mp. (22130) 13. young men.mp. (13253) 14. “young male*”.mp. (12873) 15. “young female*”.mp. (8448) 16. student*.mp.(332349) 17. young people.mp. (24628) 18. minor*.mp. (287800) 19. kid*.mp. (1036340) 20. underage*.mp. (1013) 21. puber*.mp. (47802) 22. early adult.mp. (1242) 23. young adult*.mp. (167841) 24. exp high school/ (11830) 25. exp progeny/ (34734) 26. 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 (5322013) | 27. exp alcoholic beverage/(21773) 28. exp alcohol intoxication/(11605) 29.liquor.mp. (8808) 30. Heavy drink*.mp. (7354) 31. exp alcoholism/(106005) 32. exp binge drinking/(1831) 33. heavy episodic drink*.mp. (630) 34. problem drink*.mp. (3129) 35. excessive drink*.mp. (1177) 36. risky drink*.mp. (646) 37. hazardous drink*.mp. (1005) 38. 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 (149053) 39.26 and 38 (35524) | 40. longitudinal stud*.mp.(106835) 41. cohort stud*.mp. (143528) 42. prospective study.mp. or prospective study/(355640) 43. retrospective study.mp. (448846) 44. 40 or 41 or 42 or 43 (975260) 45. randomized controlled trial/(392091) 46. 44 or 45 (1376262) 47. random*.tw (1053065) 48. Clinical Trials/(68194) 49. 46or 47 or 48 (2233152) |
| 50. A (1) and B (39) and C (49) = 107 | |||
| Studies for Sensitivity Analysis | No. of Studies (No. of Estimates) | OR | 95% CI (Lower, Upper Limit) | p for Heterogeneity ((%)) |
|---|---|---|---|---|
| All except Danielsson (2011) (boys) | 6 (7) | 2.12 | 1.89, 2.39 | 0.730 (0) |
| All except Danielsson (2011) (girls) | 6 (7) | 2.01 | 1.70, 2.38 | 0.166 (34.3) |
| All except Warner (2003) | 5 (7) | 1.96 | 1.68, 2.29 | 0.191 (31.0) |
| All except Komro (2007) | 5 (7) | 1.99 | 1.67, 2.36 | 0.147 (36.8) |
| All except Degenhardt (2015) | 5 (7) | 2.01 | 1.66, 2.43 | 0.171 (33.6) |
| All except Strandberg (2014) (girls) | 6 (7) | 1.96 | 1.68, 2.28 | 0.071 (46.3) |
| All except Strandberg (2014) (boys) | 6 (7) | 1.99 | 1.68, 2.36 | 0.149 (36.7) |
| All except McMorris (2011) | 5 (7) | 1.88 | 1.59, 2.22 | 0.338 (12) |
| Excluding studies rated as poor quality | 4 (5) | 1.90 | 1.57, 2.29 | 0.109 (47.1) |
| Excluding studies that assessed both parent and child self-report | 4 (5) | 1.90 | 1.57, 2.29 | 0.109 (47.1) |
References
- Gore, F.M.; Bloem, P.J.; Patton, G.C.; Ferguson, J.; Joseph, V.; Coffey, C.; Sawyer, S.M.; Mathers, C.D. Global burden of disease in young people aged 10–24 years: A systematic analysis. Lancet 2011, 377, 2093–2102. [Google Scholar] [CrossRef]
- Patton, G.C.; Coffey, C.; Cappa, C.; Currie, D.; Riley, L.; Gore, F.; Degenhardt, L.; Richardson, D.; Astone, N.; Sangowawa, A.O. Health of the world’s adolescents: A synthesis of internationally comparable data. Lancet 2012, 379, 1665–1675. [Google Scholar] [CrossRef]
- Kraus, L.; Guttormsson, U.; Leifman, H.; Arpa, S.; Molinaro, S.; Monshouwer, K.; Trapencieris, M.; Vicente, J.; Arnarsson, A.M.; Balakireva, O.; et al. ESPAD Report 2015 Results from the European School Survey Project on Alcohol and Other Drugs; EMCDDA/ESPAD: Lisbon, Portugal, 2016. [Google Scholar]
- Substance Abuse and Mental Health Services Administration. Drug Abuse Warning Network, 2011: National Estimates of Drug-Related Emergency Department Visits; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2013.
- Kelly, A.B.; Chan, G.C.; Weier, M.; Quinn, C.; Gullo, M.J.; Connor, J.P.; Hall, W.D. Parental supply of alcohol to australian minors: An analysis of six nationally representative surveys spanning 15 years. BMC Public Health 2016, 16, 325. [Google Scholar] [CrossRef] [PubMed]
- Kaynak, Ö.; Winters, K.C.; Cacciola, J.; Kirby, K.C.; Arria, A.M. Providing alcohol for underage youth: What messages should we be sending parents? J. Stud. Alcohol Drugs 2014, 75, 590–605. [Google Scholar] [CrossRef] [PubMed]
- Fuller, E.; Hawkins, V. Smoking, Drinking and Drug Use among Young People in England in 2011; Health and Social Care Information Centre London: London, UK, 2012. [Google Scholar]
- White, V.; Bariola, E. Australian Secondary School Students’ Use of Tobacco, Alcohol, and Over-Thecounter and Illicit Substances in 2011; The Cancer Council Victoria, Centre for Behavioural Research in Cancer: Victoria, Australia, 2012. [Google Scholar]
- Roberts, R.; Beckwith, M.; Watts, D. Mothers’ intentions to introduce their adolescent to alcohol use: Does mothers’ alcohol use effect intentions? Aust. N. Z. J. Public Health 2010, 34, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.; Ennett, S.T.; Dickinson, D.M.; Bowling, J.M. Letting children sip: Understanding why parents allow alcohol use by elementary school-aged children. Arch. Pediatr. Adolesc. Med. 2012, 166, 1053–1057. [Google Scholar] [CrossRef] [PubMed]
- Wadolowski, M.; Hutchinson, D.; Bruno, R.; Aiken, A.; Najman, J.M.; Kypri, K.; Slade, T.; McBride, N.; Mattick, R.P. Parents who supply sips of alcohol in early adolescence: A prospective study of risk factors. Pediatrics 2016, 137, e20152611. [Google Scholar] [CrossRef] [PubMed]
- Ward, B.M.; Snow, P.C. Factors affecting parental supply of alcohol to underage adolescents. Drug Alcohol Rev. 2011, 30, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Kypri, K.; Dean, J.I.; Stojanovski, E. Parent attitudes on the supply of alcohol to minors. Drug Alcohol Rev. 2007, 26, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, C.; Kypri, K.; Johnson, N.; Lynagh, M.; Love, S. Parental supply of alcohol and adolescent risky drinking. Drug Alcohol Rev. 2012, 31, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Dent, C.; Grube, J.W.; Biglan, A. Community level alcohol availability and enforcement of possession laws as predictors of youth drinking. Prev. Med. 2013, 40, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Reboussin, B.A.; Song, E.-Y.; Wolfson, M. Social influences on the clustering of underage risky drinking and its consequences in communities. J. Stud. Alcohol Drugs 2012, 73, 890–898. [Google Scholar] [CrossRef] [PubMed]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the social determinants of health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]
- Maimaris, W.; McCambridge, J. Age of first drinking and adult alcohol problems: Systematic review of prospective cohort studies. J. Epidemiol. Community Health 2014, 68, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Fergusson, D.M.; Boden, J.M.; Horwood, L.J. Alcohol misuse and psychosocial outcomes in young adulthood: Results from a longitudinal birth cohort studied to age 30. Drug Alcohol Depend. 2013, 133, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRIMSA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Sackett, D.L. Evidence-Based Medicine: How to Practice and Teach EBM; WB Saunders Company: Philadelphia, PA, USA, 1997. [Google Scholar]
- Prospero International Prospective Register of Systematic Reviews. Available online: https://www.crd.york.ac.uk/PROSPERO/ (accessed on 21 January 2016).
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley Online Library: Hoboken, NJ, USA, 2008; Volume 5. [Google Scholar]
- Wells, G.; Shea, B.; O’connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (Nos) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2000. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- STATA Data Analysis and Statistical Software. Available online: http://www.stata.com/order/ (accessed on 31 July 2016).
- McMorris, B.J.; Catalano, R.F.; Kim, M.J.; Toumbourou, J.W.; Hemphill, S.A. Influence of family factors and supervised alcohol use on adolescent alcohol use and harms: Similarities between youth in different alcohol policy contexts. J. Stud. Alcohol Drugs 2011, 72, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Thomson Reuters Endnote X7. Available online: http://endnote.com/product-details/X7 (accessed on 27 July 2016).
- Van der Vorst, H.; Engels, R.C.; Burk, W.J. Do parents and best friends influence the normative increase in adolescents’ alcohol use at home and outside the home? J. Stud. Alcohol 2010, 71, 105–114. [Google Scholar] [CrossRef]
- Danielsson, A.-K.; Romelsjo, A.; Tengstrom, A. Heavy episodic drinking in early adolescence: Gender-specific risk and protective factors. Subst. Use Misuse 2011, 46, 633–643. [Google Scholar] [CrossRef] [PubMed]
- White, H.R.; Labouvie, E.W. Towards the assessment of adolescent problem drinking. J. Stud. Alcohol 1989, 50, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Strandberg, A.K.; Bodin, M.C.; Romelsjo, A. Gender differences in the prediction of parental servings of alcohol to adolescents and youth drunkenness. Subst. Use Misuse 2014, 49, 1857–1866. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, L.; Romaniuk, H.; Coffey, C.; Hall, W.D.; Swift, W.; Carlin, J.B.; O’Loughlin, C.; Patton, G.C. Does the social context of early alcohol use affect risky drinking in adolescents? Prospective cohort study. BMC Public Health 2015, 15, 1137. [Google Scholar] [CrossRef] [PubMed]
- Warner, L.A.; White, H.R. Longitudinal effects of age at onset and first drinking situations on problem drinking. Subst. Use Misuse 2003, 38, 983–2016. [Google Scholar] [CrossRef]
- Komro, K.A.; Maldonado-Molina, M.M.; Tobler, A.L.; Bonds, J.R.; Muller, K.E. Effects of home access and availability of alcohol on young adolescents’ alcohol use. Addiction 2007, 102, 1597–1608. [Google Scholar] [CrossRef] [PubMed]
- Babor, T.; Caetano, R.; Casswell, S.; Edwards, G.; Giesbrecht, N.; Graham, K. Alcohol: No Ordinary Commodity: Research and Public Policy, 2nd ed.; Oxford University Press: Oxford, UK, 2010; p. xv. 360p. [Google Scholar]
- Room, R.; Bullock, S. Can alcohol expectancies and attributions explain Western Europe’s north-south gradient in alcohol’s role in violence? Contemp. Drug Probl. 2002, 29, 619–648. [Google Scholar]
- Rothman, K.J.; Greenland, S. Modern Epidemiology, 2nd ed.; Lippincott-Raven Publishers: Philadelphia, PA, USA, 1998; pp. 1–737. [Google Scholar]
- Kypri, K.; Dean, J.; Kirby, S.; Harris, J.; Kake, T. ‘Think before you buy under-18s drink’: Evaluation of a community alcohol intervention. Drug Alcohol Rev. 2005, 24, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Campanelli, P.C.; Dielman, T.; Shope, J.T. Validity of adolescents’ self-reports of alcohol use and misuse using a bogus pipeline procedure. Adolescence 1987, 22, 7–22. [Google Scholar] [PubMed]
- Livingston, J.A.; Testa, M.; Hoffman, J.H.; Windle, M. Can parents prevent heavy episodic drinking by allowing teens to drink at home? Addict. Behav. 2010, 35, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Fergusson, D.M.; Horwood, L.J.; Lynskey, M.T. The prevalence and risk factors associated with abusive or hazardous alcohol consumption in 16-year-olds. Addiction 1995, 90, 935–946. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, C.; Kypri, K.; Lubman, D. Changing parental behaviour to reduce risky drinking among adolescents: Current evidence and future directions. Alcohol Alcohol. 2012, 47, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Robins, J.M.; Hernan, M.A.; Brumback, B. Marginal structural models and causal inference in epidemiology. Epidemiology 2000, 11, 550–560. [Google Scholar] [CrossRef]
- Gilligan, C.; Kypri, K. Parent attitudes, family dynamics and adolescent drinking: Qualitative study of the Australian parenting guidelines for adolescent alcohol use. BMC Public Health 2012, 12, 491. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, C.; Toumbourou, J.W.; Kypri, K.; McElduff, P. Factors associated with parental rules for adolescent alcohol use. Subst. Use Misuse 2014, 49, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Wadolowski, M.; Bruno, R.; Aiken, A.; Stone, C.; Najman, J.; Kypri, K.; Slade, T.; Hutchinson, D.; McBride, N.; Mattick, R. Sipping, drinking, and early adolescent alcohol consumption: A cautionary note. Alcohol. Clin. Exp. Res. 2015, 39, 350–354. [Google Scholar] [CrossRef] [PubMed]
- Mattick, R.P.; Wadolowski, M.; Aiken, A.; Clare, P.; Hutchinson, D.; Najman, J.; Slade, T.; Bruno, R.; McBride, N.; Degenhardt, L. Parental supply of alcohol and alcohol consumption in adolescence: Prospective cohort study. Psychol. Med. 2017, 47, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Aiken, A.; Wadolowski, M.; Bruno, R.; Najman, J.; Kypri, K.; Slade, T.; Hutchinson, D.; McBride, N.; Mattick, R.P. Cohort profile: The australian parental supply of alcohol longitudinal study (APSALS). Int. J. Epidemiol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Room, R. Alcohol and the Developing World: A Public Health Perspective; Finnish Foundation for Alcohol Studies in Collaboration with World Health Organization: Helsinki, Finland, 2002; p. 276. [Google Scholar]




| Population | Adolescents who could have been exposed to parental supply of alcohol prior to the age of 18. |
| Intervention | Parental supply of alcohol |
| Comparison | Children who were exposed versus unexposed to parental supply of alcohol |
| Outcome | Adolescent risky drinking is defined as consumption of ≥5 drinks on a single occasion, at least monthly. A range of terms was used in the literature in reference to consumption at the risk level we defined, or at higher risk: alcohol misuse, drunkenness, alcohol dependence, heavy drinking, binge drinking, intoxication, heavy episodic drinking. We considered these as falling within the category “risky drinking”. |
| Author | Study Design | Location | Follow-Up Period (Years) | Sample (n) | Age at Baseline (Years) | Exposure | Outcome | Statistical Method | Results |
|---|---|---|---|---|---|---|---|---|---|
| Danielsson et al. (2011) [33] | Prospective study | Sweden | 2 | 1222 adolescents | 13 | Parents’ offer of alcohol | Risky drinking 1 | Simple and multivariable logistic regression | Parental offer of alcohol increased the risk for HED in the ninth grade for girls (OR = 1.8, 95% CI = 1.2, 2.8) only. |
| Degenhardt et al. (2015) [36] | Prospective study | Australia | 2 | 2625 adolescents | 14.9 | Drinking at home with family | Risky drinking (past week) 2 | Repeated measures discrete time proportional hazards models | Adolescents reported that those who drank with family more than 3 times were more likely to drink riskily in later adolescence (RR = 1.9, 95% CI = 1.5, 2.4). |
| Komro et al. (2007) [38] | Prospective study | USA | 2 | 1388 adolescents 1388 parents | 12 | Received alcohol from parents. | Drunkenness Risky drinking (past 2 weeks) 2 | Generalized linear mixed-model regression | A significant increase in the trajectory of drunkenness (OR = 2.3, 95% CI = 1.5, 3.4) and HED (OR = 2.0, 95% CI = 1.3–3.2) was observed when students, at age 12, reported that at the last time they drank they received alcohol from their parent. |
| McMorris et al. (2011) [27] | Prospective study | USA (Washington State) and Australia (Victoria); | 1 | 1888 adolescents 1888 parents | 13 | Adult supervised alcohol use | Alcohol-related harm | Two-group multiple-group path models | In both states, adult-supervised alcohol use among 8th grade students was associated to later alcohol use and alcohol related harms in 9th grade (correlation coefficient = 0.22). |
| Strandberg et al. (2014) [35] | Prospective study | Sweden | 2.5 | 1752 adolescents 1314 parents | 13 | Alcohol servings to youth at home. | Drunkenness (past month) | Multilevel logistic regression | Adolescents who were being supplied alcohol at home in the 7th grade were more likely have ever been drunk in the 9th grade compared to non-supplied adolescents. Girls: OR = 2.8, 95% CI = 1.5, 5.0 Boys: OR = 2.0, 95% CI = 1.2, 3.2 Supply of alcohol at home did not significantly predict frequent drunkenness in adolescents. Girls: OR = 1.26, 95% CI = 0.74, 2.15 Boys: OR = 1.24, 95% CI = 0.80, 1.92 |
| Van der Vorst et al. (2010) [32] | Prospective study | Netherlands | 3 | 428 3 | 15.22 (older sibling) 13.36 (younger sibling) | Drinking alcohol at home. | Problem drinking | Structural path analysis | For both older and younger siblings, drinking alcohol at home and outside home in mid-adolescence predicted problem drinking in late adolescence. (1) = 0.34, p > 0.05; (1) = 0.20, p > 0.05. |
| Warner & White (2003) [37] | Prospective study | USA | 3, 6, 13, and 18 | 371 adolescents | 12 | Drinking alcohol at a family gathering. | Alcohol use-related problems | Hierarchical logistic regression models | Participants who had their first drink at a family gathering before the age of 11 are significantly more likely to develop problems associated with alcohol use compared to participants who were more than 11 years old (ORs = 2.9, 95% CI = 1.4, 6.0). |
| Study | Selection | Comparability | Outcome | Quality Score | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of Exposed Cohort | Selection of the Non-Exposed Cohort from Same Source as Exposed Cohort | Ascertainment of Exposure | Outcome of Interest Was Not Present at Start of Study | Comparability of Cohorts | Assessment of Outcome | Follow-Up Long Enough for Outcome to Occur (Median Duration of Follow-Up ≥6 Months) | Adequacy of Follow-Up | ||
| Danielsson et al. (2011) [33] | Participants were truly representative of adolescents of Stockholm, Sweden. Participants covered low, middle and high socio-demographic profiles and participated from 6 districts (18 schools and 79 classes) of Stockholm out of 18 districts. ★ | Yes ★ | Students answered questionnaires in school | Yes ★ | Early alcohol debut (proportion of friends who drink, smoking, truancy, bullying, more than 300SEK to spend per month), protective factors (more than 6 h spent with parents on weekends, relationship to parents and peers), parental monitoring, school environment were adjusted for multivariable logistic regression. ★ | Adolescent self-report | Yes ★ | 87% of adolescents participated at the first data collection and after two years 85% participated at the second data collection. ★ | Good |
| Degenhardt et al. (2015) [36] | Adolescents were truly representative of the community. Schools were randomly selected from a stratified frame of government, independent private and Catholic schools. From each type of school the probability of selection was proportional to the number of students of that age. ★ | Yes ★ | Students completed questionnaires by computer at school | Yes ★ | Wave of observation, sex, school location, parental separation/divorce, frequency of parental drinking, smoking, adolescents’ smoking, cannabis use, antisocial behaviour and signs of anxiety and depression were adjusted for repeated measures discrete time proportional hazards models. ★★ | Adolescent self-report | Yes ★ | 87% participated at the 6-month follow-up, 84% at the 12-month follow-up, 81% at the 18-month follow-up and 79% at 24-month follow-up. ★ | Good |
| Komro et al. (2007) [38] | Participants were not representative of adolescents of Chicago, USA. Only Chicago public schools were selected and students were predominantly African American (44%) or Hispanic (39%) and low income (79%). | Yes ★ | Parents completed survey at home and students completed at school | Yes ★ | Race/ethnicity, age, gender and family composition, parent/child communication, family alcohol discussions, peer alcohol use, peers’ supply of alcohol, parental monitoring and alcohol communication were adjusted for generalized linear mixed-model regression. ★★ | Adolescent self-report | Yes ★ | Between 91% and 96% participated at each of the 12-month and 24-month follow-up. ★ | Fair |
| McMorris et al. (2011) [27] | Representative samples were recruited from seventh grade students of Victoria and Washington states of Australia and USA respectively. ★ | Yes ★ | Students completed questionnaires at classroom | Yes ★ | Gender, age, and socioeconomic status were adjusted for path models. ★ | Adolescent self-report | Yes ★ | 97% participated at 12-month follow-up and 24-month follow-up. ★ | Good |
| Strandberg et al. (2014) [35] | 40 municipal schools participated from 13 counties out of 21 Swedish counties. ★ | Yes ★ | Parents received questionnaires by post and youth completed questionnaires in school | Yes ★ | Multilevel logistic regression. What confounders were adjusted for was not clearly stated. | Adolescent and parent self-report | Yes ★ | 92% adolescents and 75% parents participated at the 12-month follow-up and 88% adolescents and 68% parents participated at the 30-month follow-up. | Poor |
| van der Vorst et al. (2010) [32] | Participants were representative of two biological parent households of 20 municipalities of Netherlands. There were inclusion criteria of participants that indicate “parents had to be married or living together, and the siblings and their parents had to be biologically related”. ★ | Yes ★ | Family members (both parents and two adolescent children) completed questionnaires at home in the presence of a trained interviewer | Yes ★ | Structural path analysis. What confounders were adjusted for was not clearly stated. | Adolescent self-report | Yes ★ | 416 families participated at the 12-month follow-up and 404 families participated at the 24-month follow-up. ★ | Poor |
| Warner & White (2003) [37] | Participants were representative of white adolescents (89%) who lived in metropolitan, middle-class and working environment. | Yes ★ | Parents and adolescents completed self-reported questionnaires at home during recruitment and later completed in the project site | Yes ★ | Gender, socioeconomic status, religion were adjusted for hierarchical logistic regression models. ★ | Adolescent and parent self-report | Yes ★ | 91% participated at 3-year follow-up, 6-year follow-up and 13-year follow-up. Participation rate is not specified at the 18-year follow-up. | Poor |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharmin, S.; Kypri, K.; Khanam, M.; Wadolowski, M.; Bruno, R.; Mattick, R.P. Parental Supply of Alcohol in Childhood and Risky Drinking in Adolescence: Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2017, 14, 287. https://doi.org/10.3390/ijerph14030287
Sharmin S, Kypri K, Khanam M, Wadolowski M, Bruno R, Mattick RP. Parental Supply of Alcohol in Childhood and Risky Drinking in Adolescence: Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2017; 14(3):287. https://doi.org/10.3390/ijerph14030287
Chicago/Turabian StyleSharmin, Sonia, Kypros Kypri, Masuma Khanam, Monika Wadolowski, Raimondo Bruno, and Richard P. Mattick. 2017. "Parental Supply of Alcohol in Childhood and Risky Drinking in Adolescence: Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 14, no. 3: 287. https://doi.org/10.3390/ijerph14030287
APA StyleSharmin, S., Kypri, K., Khanam, M., Wadolowski, M., Bruno, R., & Mattick, R. P. (2017). Parental Supply of Alcohol in Childhood and Risky Drinking in Adolescence: Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 14(3), 287. https://doi.org/10.3390/ijerph14030287