
Monitoring of Selected Health Indicators in Children Living in a Copper Mine Development Area in Northwestern Zambia

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
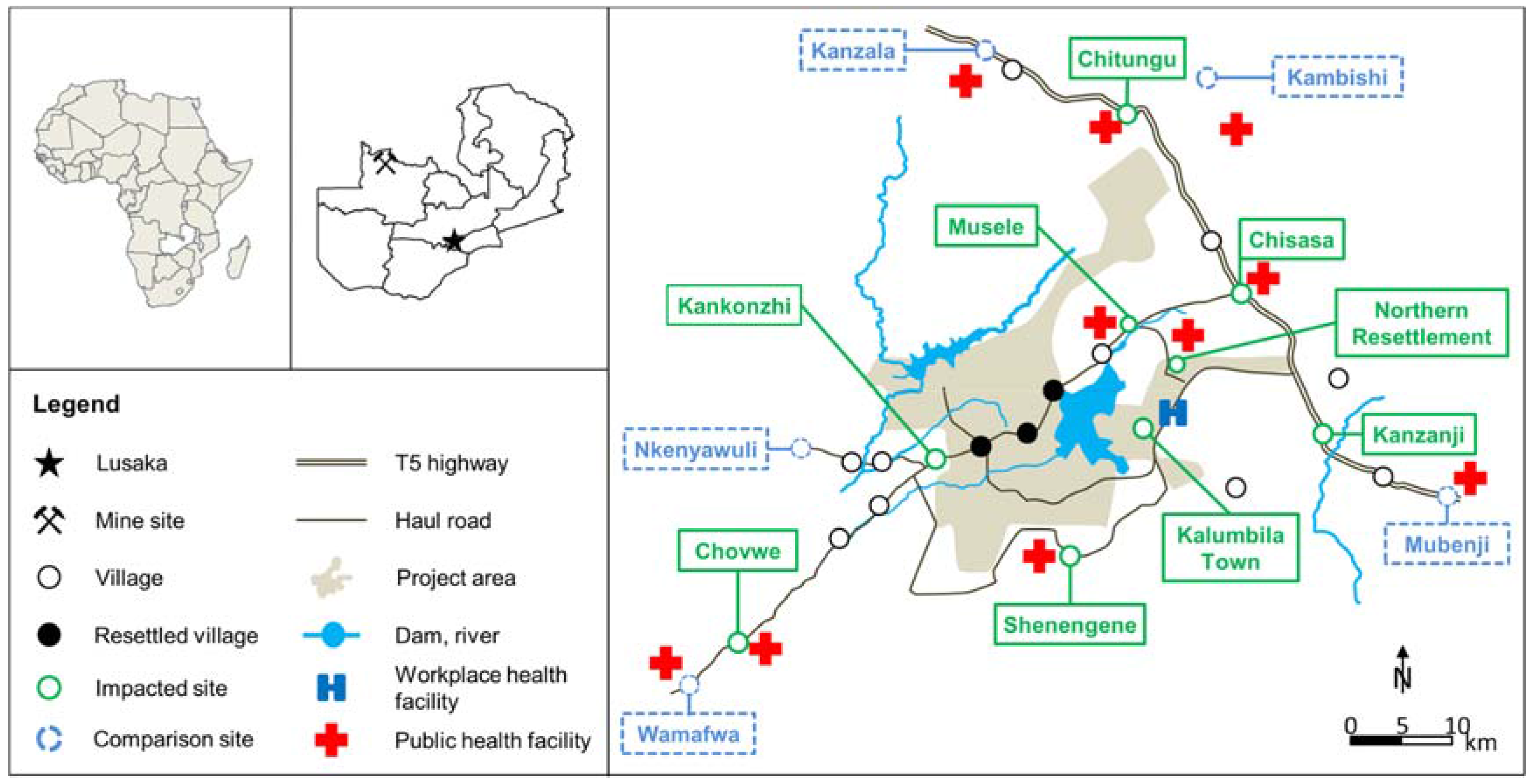
2.2. Study Area and Community Profile
2.3. Study Design and Sampling Method
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Study Population
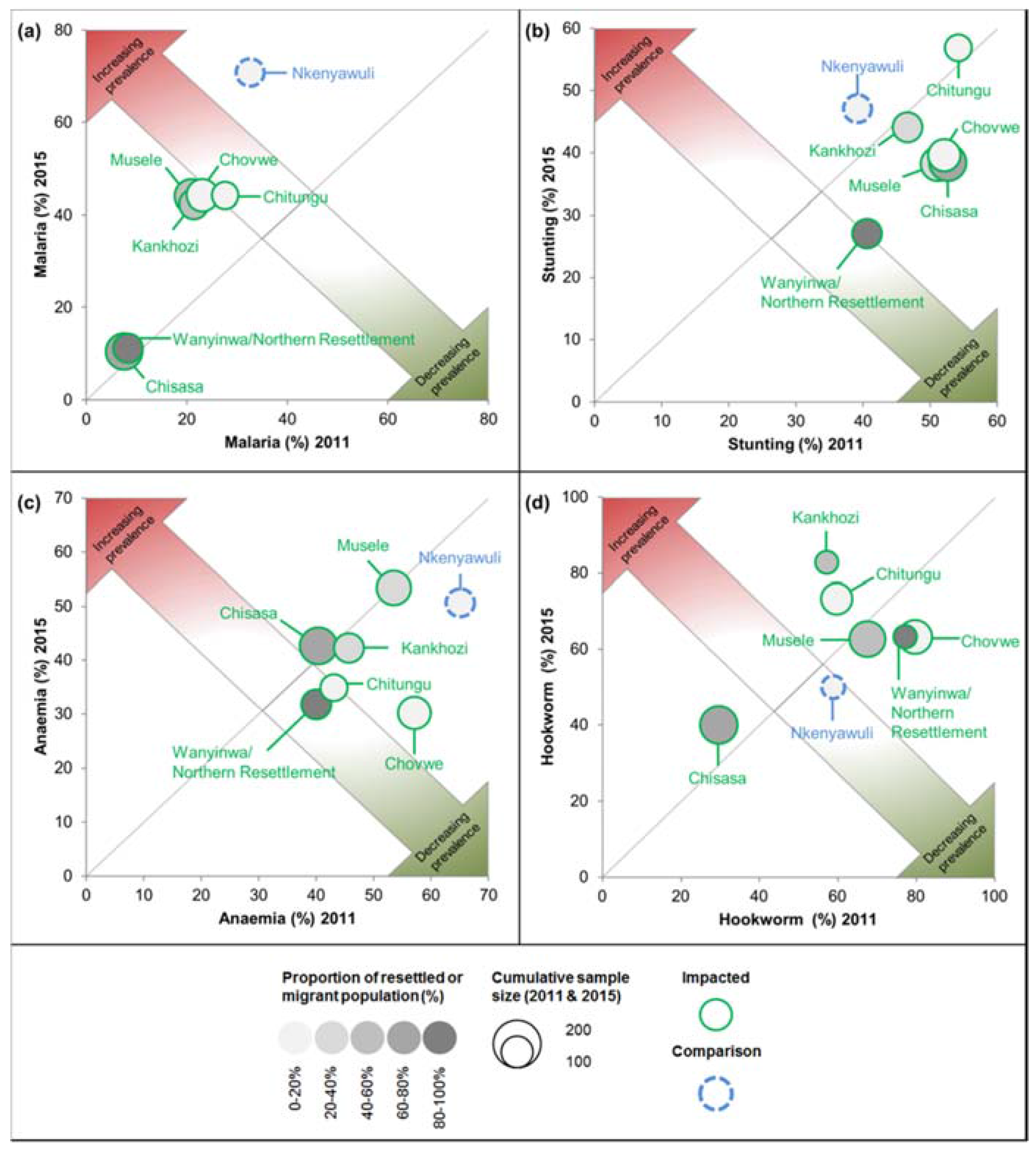
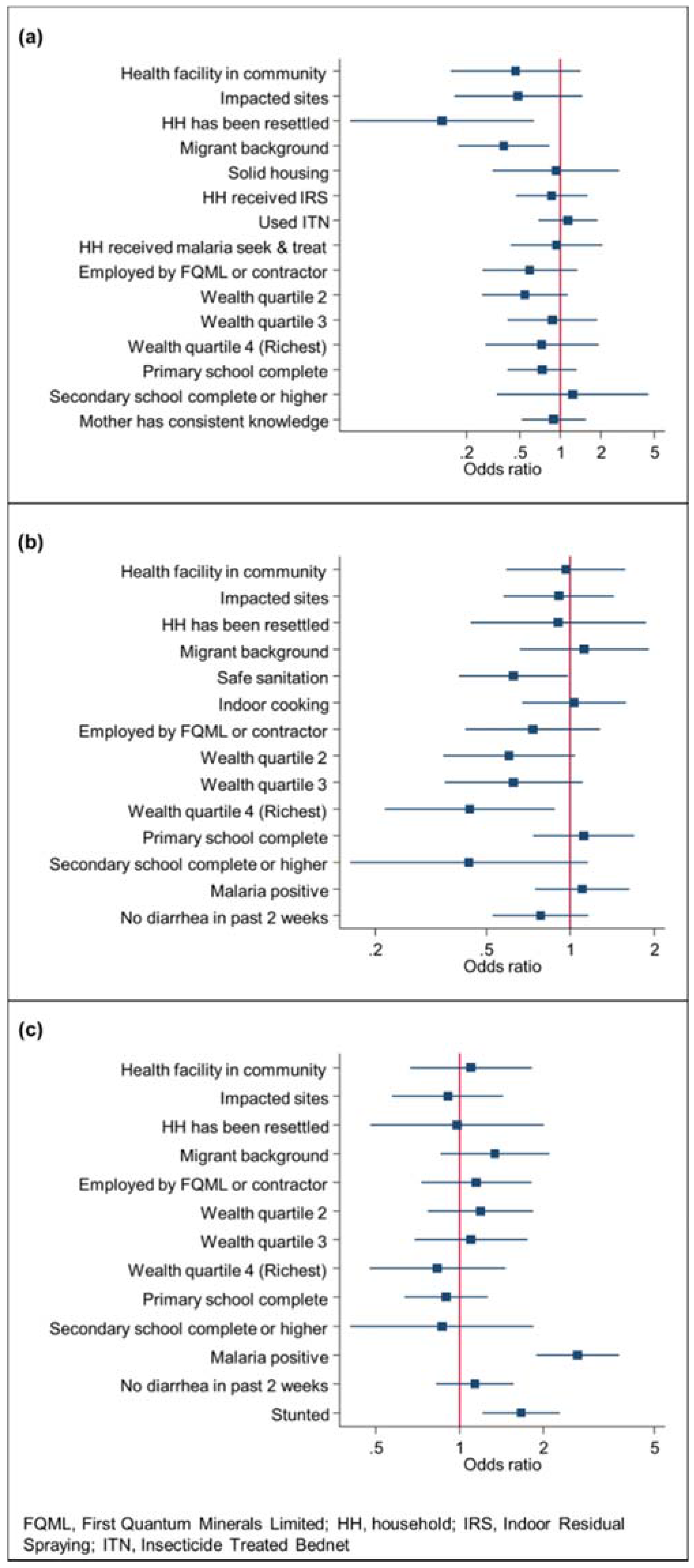
3.2. P. falciparum Infection Prevalence
3.3. Stunting Prevalence
3.4. Anaemia Prevalence
3.5. Hookworm Infection Prevalence
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Central Statistical Office. Zambia 2010 Census of Population and Housing; Central Statistical Office: Lusaka, Zambia, 2011.
- Negi, R. ‘You cannot make a camel drink water’: Capital, geo-history and contestations in the Zambian copperbelt. Geoforum 2013, 45, 240–247. [Google Scholar] [CrossRef]
- Barrick Gold Corporation. Managing in-Migration at Lumwana. Available online: http://barrickbeyondborders.com/mining/2012/12/managing-in-migration-at-lumwana/ (accessed on 5 March 2016).
- First Quantum Minerals Limited. Sustainability Report; First Quantum Minerals Limited: Vancouver, BC, Canada, 2014. [Google Scholar]
- First Quantum Minerals Limited. Development Projects: Trident. Available online: http://www.first-quantum.com/Our-Business/Development-Projects/Trident/default.aspx (accessed on 6 September 2015).
- Coastal & Environmental Services. Trident Project, Northwestern Province, Zambia: Socioeconomic Specialist Report; Coastal & Environmental Services: Grahamstown, South Africa, 2010. [Google Scholar]
- Owuor, M.; Knoblauch, A.M.; Archer, C.; Divall, M.J. Trident Project: Health Impact Assessment Follow-Up Health Survey; SHAPE Consulting Limited: St Peters, Russia, 2015. [Google Scholar]
- International Finance Corporation. Projects and People: A Handbook for Addressing Project-Induced In-Migration; International Finance Corporation: Washington, DC, USA, 2009. [Google Scholar]
- Divall, M.J.; Barnes, D.; Knoblauch, A.M. First Quantum Minerals Limited: Health Impact Assessment Scoping Study Trident Project; NewFields LLC: Denver, CO, USA, 2010. [Google Scholar]
- Gibb, H.; O’Leary, K.G. Mercury exposure and health impacts among individuals in the artisanal and small-scale gold mining community: A comprehensive review. Environ. Health Perspect. 2014, 122, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Westwood, E.; Orenstein, M. Does resource development increase community sexually transmitted infections? An environmental scan. Extr. Ind. Soc. 2016, 3, 240–248. [Google Scholar] [CrossRef]
- African Natural Resources Center; African Development Bank. AGA Malaria and Public-Private Partnerships in Ghana’s Health Sector to Obtain Value from Extractives Projects: A Case Study. Available online: https://www.afdb.org/fileadmin/uploads/afdb/Documents/Publications/anrc/AGA_Malaria_and_public_private_parternships_in_Ghana_s_Health_sector_to_obtain_value_from_extractives_projects.pdf (accessed on 15 March 2017).
- Kemm, J. Health Impact Assessment: Past Achievement, Current Understanding, and Future Progress; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Winkler, M.S.; Krieger, G.R.; Divall, M.J.; Cissé, G.; Wielga, M.; Singer, B.H.; Tanner, M.; Utzinger, J. Untapped potential of health impact assessment. Bull. World Health Organ. 2013, 91, 298–305. [Google Scholar] [CrossRef]
- Winkler, M.S.; Divall, M.J.; Krieger, G.R.; Balge, M.Z.; Singer, B.H.; Utzinger, J. Assessing health impacts in complex eco-epidemiological settings in the humid tropics: The centrality of scoping. Environ. Impact Assess. Rev. 2011, 31, 310–319. [Google Scholar] [CrossRef]
- Winkler, M.S.; Knoblauch, A.M.; Righetti, A.A.; Divall, M.J.; Koroma, M.M.; Fofanah, I.; Turay, H.; Hodges, M.H.; Utzinger, J. Baseline health conditions in selected communities of northern Sierra Leone as revealed by the health impact assessment of a biofuel project. Int. Health 2014, 6, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Winkler, M.S.; Divall, M.J.; Krieger, G.R.; Schmidlin, S.; Magassouba, M.L.; Knoblauch, A.M.; Singer, B.H.; Utzinger, J. Assessing health impacts in complex eco-epidemiological settings in the humid tropics: Modular baseline health surveys. Environ. Impact Assess. Rev. 2012, 33, 15–22. [Google Scholar] [CrossRef]
- Quigley, R.L.; den Broeder, P.; Furu, A.; Bond, B.; Cave, B.; Bos, R. Health Impact Assessment International Best Practice Principles; International Association for Impact Assessment: Fargo, ND, USA, 2006. [Google Scholar]
- Winkler, M.S.; Divall, M.J.; Krieger, G.R.; Balge, M.Z.; Singer, B.H.; Utzinger, J. Assessing health impacts in complex eco-epidemiological settings in the humid tropics: Advancing tools and methods. Environ. Impact Assess. Rev. 2010, 30, 52–61. [Google Scholar] [CrossRef]
- Parry, J.; Stevens, A. Prospective health impact assessment: Pitfalls, problems, and possible ways forward. BMJ 2001, 323, 1177–1182. [Google Scholar] [CrossRef] [PubMed]
- Grimes, D.A.; Schulz, K.F. An overview of clinical research: The lay of the land. Lancet 2002, 359, 57–61. [Google Scholar] [CrossRef]
- Petticrew, M.; Cummins, S.; Sparks, L.; Findlay, A. Validating health impact assessment: Prediction is difficult (especially about the future). Environ. Impact Assess. Rev. 2007, 27, 101–107. [Google Scholar] [CrossRef]
- Ministry of Health Zambia. Zambia National Malaria Indicator Survey 2012; Ministry of Health Zambia: Lusaka, Zambia, 2012.
- Kleinschmidt, I.; Schwabe, C.; Benavente, L.; Torrez, M.; Ridl, F.C.; Segura, J.L.; Ehmer, P.; Nchama, G.N. Marked increase in child survival after four years of intensive malaria control. Am. J. Trop. Med. Hyg. 2009, 80, 882–888. [Google Scholar] [PubMed]
- Tuno, N.; Okeka, W.; Minakawa, N.; Takagi, M.; Yan, G. Survivorship of Anopheles gambiae sensu stricto (Diptera: Culicidae) larvae in western Kenya highland forest. J. Med. Entomol. 2005, 42, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Afrane, Y.A.; Zhou, G.; Lawson, B.W.; Githeko, A.K.; Yan, G. Effects of microclimatic changes caused by deforestation on the survivorship and reproductive fitness of Anopheles gambiae in western Kenya highlands. Am. J. Trop. Med. Hyg. 2006, 74, 772–778. [Google Scholar] [PubMed]
- Martens, P.; Hall, L. Malaria on the move: Human population movement and malaria transmission. Emerg. Infect. Dis. 2000, 6, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Awolola, T.S.; Oduola, A.O.; Obansa, J.B.; Chukwurar, N.J.; Unyimadu, J.P. Anopheles gambiae s.s. breeding in polluted water bodies in urban Lagos, southwestern Nigeria. J. Vector Borne Dis. 2007, 44, 241–244. [Google Scholar] [PubMed]
- Central Statistics Office; Ministry of Health; ICF International. Zambia Demographic and Health Survey 2013–2014; Central Statistics Office; Ministry of Health; ICF International: Rockville, MD, USA, 2014.
- Crawley, J. Reducing the burden of anemia in infants and young children in malaria-endemic countries of Africa: From evidence to action. Am. J. Trop. Med. Hyg. 2004, 71, 25–34. [Google Scholar] [PubMed]
- Korenromp, E.L.; Armstrong-Schellenberg, J.R.; Williams, B.G.; Nahlen, B.L.; Snow, R.W. Impact of malaria control on childhood anaemia in Africa—A quantitative review. Trop. Med. Int. Health 2004, 9, 1050–1065. [Google Scholar] [CrossRef] [PubMed]
- Naing, C.; Whittaker, M.A.; Nyunt-Wai, V.; Reid, S.A.; Wong, S.F.; Mak, J.W.; Tanner, M. Malaria and soil-transmitted intestinal helminth co-infection and its effect on anemia: A meta-analysis. Trans. R. Soc. Trop. Med. Hyg. 2013, 107, 672–683. [Google Scholar] [CrossRef] [PubMed]
- Tolentino, K.; Friedman, J.F. An update on anemia in less developed countries. Am. J. Trop. Med. Hyg. 2007, 77, 44–51. [Google Scholar] [PubMed]
- Yap, P.; Fürst, T.; Müller, I.; Kriemler, S.; Utzinger, J.; Steinmann, P. Determining soil-transmitted helminth infection status and physical fitness of school-aged children. J. Vis. Exp. 2012, 66, e3966. [Google Scholar] [CrossRef] [PubMed]
- Winkler, M.S.; Krieger, G.R.; Divall, M.J.; Singer, B.H.; Utzinger, J. Health impact assessment of industrial development projects: A spatio-temporal visualization. Geospat. Health 2012, 6, 299–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karagiannis-Voules, D.A.; Biedermann, P.; Ekpo, U.F.; Garba, A.; Langer, E.; Mathieu, E.; Midzi, N.; Mwinzi, P.; Polderman, A.M.; Raso, G.; et al. Spatial and temporal distribution of soil-transmitted helminth infection in sub-Saharan Africa: A systematic review and geostatistical meta-analysis. Lancet Infect. Dis. 2015, 15, 74–84. [Google Scholar] [CrossRef]
- Moonen, B.; Cohen, J.M.; Snow, R.W.; Slutsker, L.; Drakeley, C.; Smith, D.L.; Abeyasinghe, R.R.; Rodriguez, M.H.; Maharaj, R.; Tanner, M.; et al. Operational strategies to achieve and maintain malaria elimination. Lancet 2010, 376, 1592–1603. [Google Scholar] [CrossRef]
- Tusting, L.S.; Ippolito, M.M.; Willey, B.A.; Kleinschmidt, I.; Dorsey, G.; Gosling, R.D.; Lindsay, S.W. The evidence for improving housing to reduce malaria: A systematic review and meta-analysis. Malar. J. 2015, 14, 209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health Zambia. Zambia National Malaria Indicator Survey 2010; Ministry of Health Zambia: Lusaka, Zambia, 2010.
- Pascual, M.; Ahumada, J.A.; Chaves, L.F.; Rodo, X.; Bouma, M. Malaria resurgence in the East African highlands: Temperature trends revisited. Proc. Natl. Acad. Sci. USA 2006, 103, 5829–5834. [Google Scholar] [CrossRef] [PubMed]
- Reiner, R.C.; Geary, M.; Atkinson, P.M.; Smith, D.L.; Gething, P.W. Seasonality of Plasmodium falciparum transmission: A systematic review. Malar. J. 2015, 14. [Google Scholar] [CrossRef] [PubMed]
- Knoblauch, A.M.; Hodges, M.H.; Bah, M.S.; Kamara, H.I.; Kargbo, A.; Paye, J.; Turay, H.; Nyorkor, E.D.; Divall, M.J.; Zhang, Y.; et al. Changing patterns of health in communities impacted by a bioenergy project in northern Sierra Leone. Int. J. Environ. Res. Public Health 2014, 11, 12997–13016. [Google Scholar] [CrossRef] [PubMed]
- Corsi, D.J.; Mejia-Guevara, I.; Subramanian, S.V. Risk factors for chronic undernutrition among children in India: Estimating relative importance, population attributable risk and fractions. Soc. Sci. Med. 2016, 157, 165–185. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.; Arnold, B.F.; Afreen, S.; Goto, R.; Huda, T.M.N.; Haque, R.; Raqib, R.; Unicomb, L.; Ahmed, T.; Colford, J.M., Jr.; et al. Household environmental conditions are associated with enteropathy and impaired growth in rural Bangladesh. Am. J. Trop. Med. Hyg. 2013, 89, 130–137. [Google Scholar] [CrossRef] [PubMed]
- International Conference on Primary Health Care. International Conference on Primary Health Care. Declaration of Alma-Ata. In International Conference on Primary Health Care; World Health Organization: Alma-Ata, Kazakhstan, 1978. [Google Scholar]
- Stoltzfus, R.J.; Chwaya, H.M.; Tielsch, J.M.; Schulze, K.J.; Albonico, M.; Savioli, L. Epidemiology of iron deficiency anemia in Zanzibari schoolchildren: The importance of hookworms. Am. J. Clin. Nutr. 1997, 65, 153–159. [Google Scholar] [PubMed]
- Jiraanankul, V.; Aphijirawat, W.; Mungthin, M.; Khositnithikul, R.; Rangsin, R.; Traub, R.J.; Piyaraj, P.; Naaglor, T.; Taamasri, P.; Leelayoova, S. Incidence and risk factors of hookworm infection in a rural community of central Thailand. Am. J. Trop. Med. Hyg. 2011, 84, 594–598. [Google Scholar] [CrossRef] [PubMed]
- World Health Organzation. Health of Migrants; World Health Organzation: Geneva, Switzerland, 2007. [Google Scholar]
- Benkhalti Jandu, M.; Canuto De Medeiros, B.; Bourgeault, I.; Tugwell, P. The inclusion of migrants in health impact assessments: A scoping review. Environ. Impact Assess. Rev. 2015, 50, 16–24. [Google Scholar] [CrossRef]
- Erlanger, T.; Sayasone, S.; Krieger, G.R.; Kaul, S.; Sananikhom, P.; Tanner, M. Baseline health situation of communities affected by the Nam Theun 2 hydroelectric project in central Lao PDR and indicators for monitoring. Int. J. Environ. Health Res. 2008, 18, 223–242. [Google Scholar] [CrossRef] [PubMed]
- The Inspection Panel. Investigation Report: Cameroon Petroleum Development and Pipeline Project (Loan No. 7020-CM) and Petroleum Environment Capacity Enhancement (CAPECE) Project (Credit No. 3372-CM); The Inspection Panel: Washington, DC, USA, 2003. [Google Scholar]
- Knoblauch, A.M.; Divall, M.J.; Owuor, M.; Musunka, G.; Pascall, A.; Nduna, K.; Ng’uni, H.; Utzinger, J.; Winkler, M.S. Experience and lessons from health impact assessment guiding prevention and control of HIV/AIDS in a copper mine project, Northwestern Zambia. Infect. Dis. Poverty 2017. under review. [Google Scholar]
- World Health Organization Regional Office for Europe/European Centre for Health Policy. Health Impact Assessment: Main Concepts and Suggested Approach; World Health Organization Regional Office for Europe, European Centre for Health Policy: Copenhagen, Denmark, 1999. [Google Scholar]
- Equator Principles Association. The Equator Principles. Available online: http://www.equator-principles.com/ (accessed on 5 March 2016).
- Glinz, D.; Silué, K.D.; Knopp, S.; Lohourignon, L.K.; Yao, K.P.; Steinmann, P.; Rinaldi, L.; Cringoli, G.; N’Goran, E.K.; Utzinger, J. Comparing diagnostic accuracy of Kato-Katz, Koga agar plate, ether-concentration, and FLOTAC for Schistosoma mansoni and soil-transmitted helminths. PLoS Negl. Trop. Dis. 2010, 4, e754. [Google Scholar] [CrossRef] [PubMed]
- United Nations. The 2030 Agenda for Sustainable Development; United Nations: Geneva, Switzerland, 2015. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicator | Definition and Measurement Methods | Relevance to Children’s Health and the Local Project Context |
|---|---|---|
| Plasmodium falciparum infection prevalence in children aged 6–59 months | P. falciparum infection is defined as the detection of the P. falciparum histidine-rich protein II antigen in capillary blood using a rapid diagnostic test (RDT; SD BIOLINE Malaria Ag P.f; Standard Diagnostics Inc., Gyeonggi-do, Republic of Korea) [23]. | Improved local economy, vector control measures implemented by the project and better infrastructure (e.g., roads, health facilities) can improve access to vector control measures and health care [12,24]. Environmental alteration due to project activities can potentially increase the number of vector breeding sites [25,26]. Camp follower settlements may develop with poor associated environmental health conditions potentially increasing vector breeding sites and human-vector contact if not managed appropriately [27,28]. |
| Stunting prevalence in in children aged 0–59 months | Stunting, or low height-for-age, is defined as -2 standard deviation units from the WHO reference population median and measured using a digital scale and portable stadiometer (Seca 877; Seca GmbH, Hamburg, Germany) [29]. | Improved local economy can improve nutritional status. Reduced access to agricultural land for local populations and food price inflations due to increased purchasing power can increase the burden of malnutrition |
| Anaemia prevalence in children aged 6–59 months | Anaemia is defined as haemoglobin (Hb) < 11 g/dL in capillary blood assessed using a HemoCue® 201+ testing device (HemoCue Hb 201 System; HemoCue AB, Ängelholm, Sweden) [23]. Age was recorded based on the date of birth given in the child’s vaccination card, if available, or based on parents report. | Anaemia is used as a proxy indicator for general health and well-being, because of its multifactorial aetiology (e.g., intake and uptake of dietary iron, parasitic infections and prevalence of sickle cell disease) [30,31,32]. Epidemiology of infectious diseases, access to health care and diets potentially change due to the project development which, in turn, influences rates of anaemia [33]. |
| Hookworm infection prevalence in children aged 9–14 years | Hookworm infection is defined as detection of hookworm eggs in a single thick-smear of a fresh, morning stool sample prepared and examined by the Kato-Katz technique within 20–40 min after slide preparation (using 41.7 mg templates) [34]. Intensity of infection was determined by counting hookworm eggs per slide and multiplied by a factor of 24 to obtain eggs per gram of stool (EPG). | Project-induced in-migration may place pressure on existing sanitation, which poses a risk for the transmission of diarrhoeal diseases and intestinal parasites. Increased income coupled with behaviour change can lead to protection through wearing of footwear. First-time inhabitation of native soil (e.g., new settlements or resettlement), increased use of footwear (due to increased income) and intensive circulation of top soil (due to project-associated activities) can lower exposure to hookworm eggs in the environment. |
| Sentinel Sites | Households | Children Aged < 6 Months | Children Aged 6–59 Months | School-Going Children Aged 9–14 Years | Proportion of Households that Have Been Resettled due to the Project | Proportion of Migrant Households (in the Area for <5 years) | Proportion of Households that Use Improved Sanitation | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Year | 2011 | 2015 | 2011 | 2015 | 2011 | 2015 | 2011 | 2015 | 2015 | 2015 | 2015 |
| Wanyinwa (2011)/Northern Resettlement (2015) | 35 | 34 | 4 | 7 | 60 | 63 | 35 | 30 | 97.1 | 2.9 | 97.1 |
| Musele 1 | 30 | 66 | 2 | 18 | 43 | 116 | 40 | 59 | 3.0 | 30.3 | 34.9 |
| Chisasa 1 | 66 | 65 | 3 | 16 | 94 | 96 | 44 | 60 | 1.5 | 66.2 | 47.7 |
| Kankonzhi 1 | 36 | 30 | 3 | 7 | 70 | 52 | 35 | 29 | 3.3 | 36.7 | 50.0 |
| Chitungu 1 | 30 | 33 | 1 | 8 | 58 | 43 | 57 | 30 | 0.0 | 0.0 | 21.2 |
| Chovwe 1 | 61 | 32 | 3 | 10 | 91 | 43 | 64 | 30 | 0.0 | 6.3 | 43.8 |
| Kalumbila Town | NA | 30 | NA | 7 | NA | 36 | NA | 30 | 0.0 | 100.0 | 100.0 |
| Shenengene | NA | 32 | NA | 4 | NA | 48 | NA | 30 | 96.9 | 3.1 | 93.8 |
| Kanzanji | NA | 32 | NA | 8 | NA | 51 | NA | 29 | 3.1 | 43.8 | 6.3 |
| Total impacted | 258 | 354 | 16 | 85 | 416 | 548 | 275 | 327 | 19.5 | 34.5 | 52.3 |
| Nkenyawuli 1 | 31 | 32 | 8 | 3 | 43 | 65 | 34 | 30 | 0.0 | 6.3 | 37.5 |
| Wamafwa | NA | 33 | NA | 6 | NA | 66 | NA | 30 | 0.0 | 6.1 | 33.3 |
| Kanzala | NA | 32 | NA | 4 | NA | 52 | NA | 30 | 0.0 | 15.6 | 21.9 |
| Kambishi | NA | 32 | NA | 8 | NA | 51 | NA | 30 | 0.0 | 0.0 | 3.1 |
| Mubenji | NA | 33 | NA | 6 | NA | 55 | NA | 30 | 0.0 | 21.2 | 0.0 |
| Total comparison | 31 | 162 | 8 | 27 | 43 | 289 | 34 | 150 | 0.0 | 9.9 | 19.1 |
| P. Falciparum Infection in Children Aged 6–59 Months | Stunting in Children Aged 0–59 Months | |||||||
|---|---|---|---|---|---|---|---|---|
| n | Prevalence (%; 95% CI) | OR | p-Value | n | Prevalence (%; 95% CI) | OR | p-Value | |
| Difference at baseline | ||||||||
| Comparison (2011) | 43 | 32.5 (19.0–48.5) | 1.00 | 51 | 39.2 (25.8–53.8) | 1.00 | ||
| Impacted (2011) | 416 | 17.5 (14.0–21.5) | 0.33 (0.05–2.20) | 0.25 | 432 | 49.7 (44.9–54.5) | 1.61 (0.77–3.35) | 0.20 |
| Period effect 1 | ||||||||
| Comparison (2011) | 43 | 32.5 (19.0–48.5) | 1.00 | 51 | 39.2 (25.8–53.8) | 1.00 | ||
| Comparison (2015) | 65 | 70.7 (58.1–81.3) | 6.97 (2.20–22.0) | <0.01 | 68 | 47.0 (34.8–59.5) | 1.41 (0.58–3.46) | 0.44 |
| Period effect 1 | ||||||||
| Impacted (2011) | 416 | 17.5 (14.0–21.5) | 1.00 | 432 | 49.7 (44.9–54.5) | 1.00 | ||
| Impacted (2015) | 413 | 30.9 (26.5–35.6) | 2.51 (1.56–4.02) | <0.01 | 479 | 39.4 (35.0–43.9) | 0.63 (0.46–0.87) | <0.01 |
| Change over time in impacted vs. comparison sites | ||||||||
| Comparison (2011–2015) | n/a | n/a | 1.00 | n/a | n/a | 1.00 | ||
| Impacted (2011–2015) | n/a | n/a | 0.36 (0.10–1.23) | 0.10 | n/a | n/a | 0.44 (0.17–1.15) | 0.09 |
| Anaemia in Children Aged 6–59 Months | Hookworm in Children Aged 9–14 Years | |||||||
|---|---|---|---|---|---|---|---|---|
| n | Prevalence (%; 95% CI) | OR | p-Value | n | Prevalence (%; 95% CI) | OR | p-Value | |
| Difference at baseline | ||||||||
| Comparison (2011) | 43 | 65.1 (49.0–78.9) | 1.00 | 34 | 58.8 (40.6–75.3) | 1.00 | ||
| Impacted (2011) | 416 | 46.6 (41.7–51.5) | 0.47 (0.22–0.98) | 0.04 | 275 | 62.5 (56.5–68.2) | 1.16 (0.33–4.03) | 0.80 |
| Period effect 1 | ||||||||
| Comparison (2011) | 43 | 65.1 (49.0–78.9) | 1.00 | 34 | 58.8 (40.6–75.3) | 1.00 | ||
| Comparison (2015) | 65 | 50.8 (38.0–63.3) | 0.55 (0.24–1.22) | 0.14 | 30 | 50.0 (31.2–68.7) | 0.69 (0.25–1.88) | 0.47 |
| Period effect 1 | ||||||||
| Impacted (2011) | 416 | 46.6 (41.7–51.5) | 1.00 | 275 | 62.5 (56.5–68.2) | 1.00 | ||
| Impacted (2015) | 413 | 41.9 (37.0–46.8) | 0.79 (0.60–1.05) | 0.11 | 238 | 60.9 (54.4–67.1) | 1.07 (0.73–1.56) | 0.71 |
| Change over time in impacted vs. comparison sites | ||||||||
| Comparison (2011–2015) | n/a | n/a | 1.00 | n/a | n/a | 1.00 | ||
| Impacted (2011–2015) | n/a | n/a | 1.44 (0.62–3.36) | 0.39 | n/a | n/a | 1.54 (0.53–4.46) | 0.42 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knoblauch, A.M.; Divall, M.J.; Owuor, M.; Archer, C.; Nduna, K.; Ng’uni, H.; Musunka, G.; Pascall, A.; Utzinger, J.; Winkler, M.S. Monitoring of Selected Health Indicators in Children Living in a Copper Mine Development Area in Northwestern Zambia. Int. J. Environ. Res. Public Health 2017, 14, 315. https://doi.org/10.3390/ijerph14030315
Knoblauch AM, Divall MJ, Owuor M, Archer C, Nduna K, Ng’uni H, Musunka G, Pascall A, Utzinger J, Winkler MS. Monitoring of Selected Health Indicators in Children Living in a Copper Mine Development Area in Northwestern Zambia. International Journal of Environmental Research and Public Health. 2017; 14(3):315. https://doi.org/10.3390/ijerph14030315
Chicago/Turabian StyleKnoblauch, Astrid M., Mark J. Divall, Milka Owuor, Colleen Archer, Kennedy Nduna, Harrison Ng’uni, Gertrude Musunka, Anna Pascall, Jürg Utzinger, and Mirko S. Winkler. 2017. "Monitoring of Selected Health Indicators in Children Living in a Copper Mine Development Area in Northwestern Zambia" International Journal of Environmental Research and Public Health 14, no. 3: 315. https://doi.org/10.3390/ijerph14030315
APA StyleKnoblauch, A. M., Divall, M. J., Owuor, M., Archer, C., Nduna, K., Ng’uni, H., Musunka, G., Pascall, A., Utzinger, J., & Winkler, M. S. (2017). Monitoring of Selected Health Indicators in Children Living in a Copper Mine Development Area in Northwestern Zambia. International Journal of Environmental Research and Public Health, 14(3), 315. https://doi.org/10.3390/ijerph14030315