
Life Course Trajectories of Later-Life Cognitive Functions: Does Social Engagement in Old Age Matter?

Abstract
:1. Introduction
Present Study
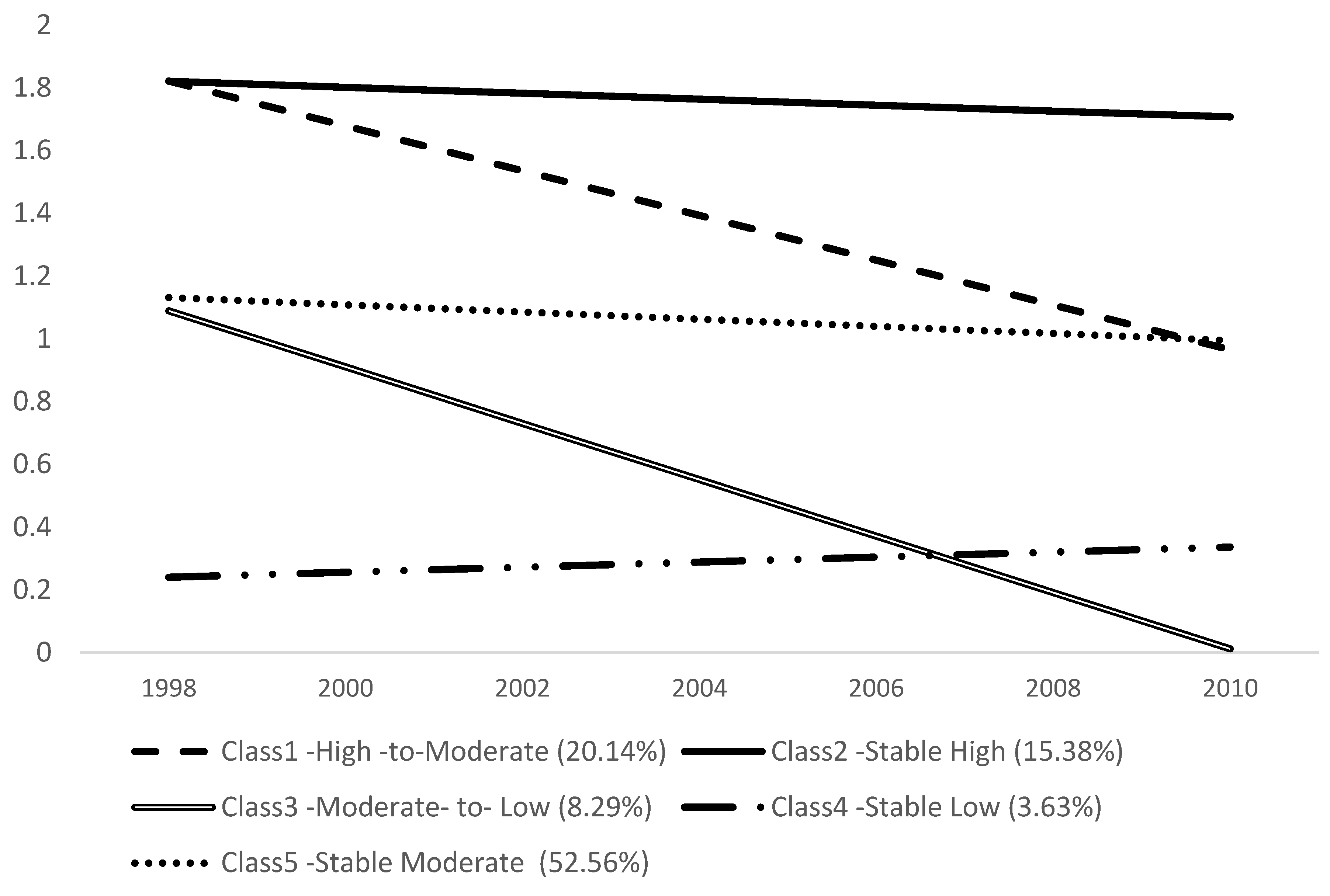
- Can different group trajectories of cognitive function among older adults be identified during the 12-year observed period? We focus on life course factors in examining change trajectories of cognitive function in old age using a cognitive scale rather than a measure of cognitive impairment [21]. We expect to find disparate trajectory groups characterized as normal, age-vulnerable, and with pathological decline linked with neurological changes, and that cognition trajectories will further diverge as a result of heterogeneous developmental life-long processes.
- Will the characteristics of later-life cognitive function trajectories vary based on a range of life course factors from childhood to old age? Based on the cumulative disadvantage perspective and prior research, we expect that disadvantages from childhood and adulthood as well as life events and health changes in old age will be associated with trajectory groups with lower levels of or declining cognitive function at baseline and over time.
- To what extent is social engagement associated with trajectories of cognitive function? Based on previous literature on social engagement, we hypothesize that increased social engagement (frequency of engagement with social network and volunteering) over time will be associated with maintaining higher levels of cognitive function, while decreases in social engagement will be related to lower levels of cognitive function.
2. Materials and Methods
2.1. Data and Sample
2.2. Measures
- ascribed factors, for which age was measured in years at baseline, gender (1 = female, 0 = male), and race/ethnicity (1 = white, 0 = non-white);
- childhood socioeconomic status (SES) measured by parents’ education level (less than 8 years = 0, greater than 8 years = 1), family poverty status (1 = poor, 0 = not poor), and childhood health through retrospective reports in which respondents were asked to assess their health before the age of 16 (excellent = 1 to poor = 5);
- achieved status in adulthood measured by years of education (0–17) and household income as a mean of log-transformed values across the observed period; and
- life events and health conditions in adulthood measured by:
- death of a spouse or divorce (0/1), nursing home admission (0/1), relocation (0/1)
- chronic health conditions using the number of chronic diseases (high blood pressure, diabetes, cancer, lung disease, heart disease, stroke, psychiatric problems, and arthritis, 0 to 8) at baseline as well as change during the observed period (none experienced a decrease)
- functional health based on the sum of activities of daily living (ADL) the respondent had problems with (difficulty with bathing, eating, dressing, walking across a room, and getting in or out of bed, 0–5) and instrumental activities of daily living (IADL) (using a telephone, taking medication, handling money, shopping, and preparing meals, 0–5). Three measures were used including number at baseline, increases during the observed period, decreases during that period.
2.3. Analysis
3. Results
3.1. Group Trajectory of Cognitive Function in Old Age
3.2. Trajectory Groups of Cognitive Function by Life Course Factors
3.3. Role of Social Environmental Factors
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kuh, D. New dynamics of ageing (NDA) preparatory network. A life course approach to healthy aging, frailty, and capability. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 717–721. [Google Scholar] [CrossRef] [PubMed]
- Lynch, J.; Smith, G.D. A life course approach to chronic disease epidemiology. Annu. Rev. Public Health 2005, 26, 1–35. [Google Scholar] [CrossRef] [PubMed]
- Elder, G.H., Jr.; Shanahan, M.J. The life course and human development. In Handbook of Child Psychology, Vol. 1: Theoretical Models of Human Development, 1st ed.; Damon, W., Lerner, R.M., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2006; pp. 665–715. [Google Scholar]
- Luo, Y.; Waite, L.J. The impact of childhood and adult SES on physical, mental, and cognitive well-being in later life. J. Gerontol. B Psychol. Sci. Soc. Sci. 2005, 60, S93–S101. [Google Scholar] [CrossRef] [PubMed]
- Turrell, G.; Lynch, J.W.; Kaplan, G.A.; Everson, S.A.; Helkala, E.L.; Kauhanen, J.; Salonen, J.T. Socioeconomic position across the lifecourse and cognitive function in late middle age. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, S43–S51. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Gu, D.; Hayward, M.D. Early life influences on cognitive impairment among oldest old Chinese. J. Gerontol. B Psychol. Sci. Soc. Sci. 2008, 63, S25–S33. [Google Scholar] [CrossRef] [PubMed]
- Kuh, D.; Ben-Shlomo, Y. A Life Course Approach to Chronic Disease Epidemiology, 2nd ed.; Oxford University Press: New York, NY, USA, 2004; pp. 1–473. [Google Scholar]
- Vidarsdottir, H.; Fang, F.; Chang, M.; Aspelund, T.; Fall, K.; Jonsdottir, M.K.; Gudnason, V. Spousal loss and cognitive function in later life: A 25-year follow-up in the AGES-Reykjavik study. Am. J. Epidemiol. 2014, 179, 674–683. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Chiao, C.; Ksobiech, K. The effects of mid-life socioeconomic disadvantage and perceived social support on trajectories of subsequent depressive symptoms among older taiwanese women. BMC Public Health 2014, 14, 384. [Google Scholar] [CrossRef] [PubMed]
- Tschanz, J.T.; Corcoran, C.D.; Schwartz, S.; Treiber, K.; Green, R.C.; Norton, M.C.; Lyketsos, J.M. Progression of cognitive, functional, and neuropsychiatric symptom domains in a population cohort with alzheimer dementia: The cache county dementia progression study. Am. J. Geriatr. Psychiatry 2011, 19, 532–542. [Google Scholar] [CrossRef] [PubMed]
- Bielak, A.A. How can we not ‘lose it’ if we still don’t understand how to ‘use it’? Unanswered questions about the influence of activity participation on cognitive performance in older age—A mini-review. Gerontology 2010, 56, 507–519. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.A.; Schneider, J.A.; Tang, Y.; Arnold, S.E.; Wilson, R.S. The effect of social networks on the relation between alzheimer’s disease pathology and level of cognitive function in old people: A longitudinal cohort study. Lancet Neurol. 2006, 5, 406–412. [Google Scholar] [CrossRef]
- James, B.D.; Wilson, R.S.; Barnes, L.L.; Bennett, D.A. Late-life social activity and cognitive decline in old age. J. Int. Neuropsychol. Soc. 2011, 17, 998–1005. [Google Scholar] [CrossRef] [PubMed]
- Beland, F.; Zunzunegui, M.V.; Alvarado, B.; Otero, A.; Del Ser, T. Trajectories of cognitive decline and social relations. J. Gerontol. B Psychol. Sci. Soc. Sci. 2005, 60, P320–P330. [Google Scholar] [CrossRef] [PubMed]
- Krueger, K.R.; Wilson, R.S.; Kamenetsky, J.M.; Barnes, L.L.; Bienias, J.L.; Bennett, D.A. Social engagement and cognitive function in old age. Exp. Aging Res. 2009, 35, 45–60. [Google Scholar] [CrossRef] [PubMed]
- Bielak, A.A.; Hughes, T.F.; Small, B.J.; Dixon, R.A. It’s never too late to engage in lifestyle activities: Significant concurrent but not change relationships between lifestyle activities and cognitive speed. J. Gerontol. B Psychol. Sci. Soc. Sci. 2007, 62, P331–P339. [Google Scholar] [CrossRef] [PubMed]
- Fratiglioni, L.; Wang, H.X.; Ericsson, K.; Maytan, M.; Winblad, B. Influence of social network on occurrence of dementia: A community-based longitudinal study. Lancet 2000, 355, 1315–1319. [Google Scholar] [CrossRef]
- Zunzunegui, M.V.; Alvarado, B.E.; Del Ser, T.; Otero, A. Social networks, social integration, and social engagement determine cognitive decline in community-dwelling Spanish older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2003, 58, S93–S100. [Google Scholar] [CrossRef] [PubMed]
- Brenowitz, W.D.; Kukull, W.A.; Beresford, S.A.; Monsell, S.E.; Williams, E.C. Social relationships and risk of incident mild cognitive impairment in U.S. alzheimer’s disease centers. Alzheimer Dis. Assoc. Disord. 2014, 28, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Glei, D.A.; Landau, D.A.; Goldman, N.; Chuang, Y.L.; Rodriguez, G.; Weinstein, M. Participating in social activities helps preserve cognitive function: An analysis of a longitudinal, population-based study of the elderly. Int. J. Epidemiol. 2005, 34, 864–871. [Google Scholar] [CrossRef] [PubMed]
- Fors, S.; Lennartsson, C.; Lundberg, O. Childhood living conditions, socioeconomic position in adulthood, and cognition in later life: Exploring the associations. J. Gerontol. B Psychol. Sci. Soc. Sci. 2009, 64, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Servais, M.A. Overview of HRS Public Data Files for Cross-Sectional and Longitudinal Analysis. Available online: http://hrsonline.isr.umich.edu/sitedocs/dmgt/OverviewofHRSPublicData.pdf (accessed on 1 December 2015).
- Walsh, E.G.; Wu, B.; Mitchell, J.B.; Berkmann, L.F. Cognitive function and acute care utilization. J. Gerontol. B Psychol. Sci. Soc. Sci. 2003, 58, S38–S49. [Google Scholar] [CrossRef] [PubMed]
- Herzog, A.R.; Wallace, R.B. Measures of cognitive functioning in the AHEAD study. J. Gerontol. B Psychol. Sci. Soc. Sci. 1997, 52, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Muthén, B.; Muthén, L.K. Integrating person-centered and variable-centered analyses: Growth mixture modeling with latent trajectory classes. Alcohol Clin. Exp. Res. 2000, 24, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Land, K.C. Introduction to the special issue on finite mixture models. Sociol. Meth. Res. 2001, 29, 275–281. [Google Scholar] [CrossRef]
- Muthén, B. Statistical and substantive checking in growth mixture modeling: Comment on Bauer and Curran (2003). Psychol. Methods 2003, 8, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Muthén, B. Latent variable analysis. In The Sage handbook of Quantitative Methodology for the Social Sciences, 1st ed.; Kaplan, D., Ed.; Sage Publications: Thousand Oaks, CA, USA, 2004; pp. 345–368. [Google Scholar]
- Jung, T.; Wickrama, K. An introduction to latent class growth analysis and growth mixture modeling. Soc. Personal. Psychol. Compass. 2008, 2, 302–317. [Google Scholar] [CrossRef]
- Elias, M.F.; Elias, P.K.; D’agostino, R.B.; Silbershatz, H.; Wolf, P.A. Role of age, education, and gender on cognitive performance in the framingham heart study: Community-based norms. Exp. Aging Res. 1997, 23, 201–235. [Google Scholar] [CrossRef] [PubMed]
- Elwood, P.C.; Gallacher, J.E.; Hopkinson, C.A.; Pickering, J.; Rabbitt, P.; Stollery, B.; Brayne, C.; Huppert, F.A.; Bayer, A. Smoking, drinking, and other life style factors and cognitive function in men in the caerphilly cohort. J. Epidemiol. Community Health 1999, 53, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Jefferson, A.L.; Gibbons, L.E.; Rentz, D.M.; Carvalho, J.O.; Manly, J.; Bennett, D.A.; Jones, R.N. A life course model of cognitive activities, socioeconomic status, education, reading ability, and cognition. J. Am. Geriatr. Soc. 2011, 59, 1403–1411. [Google Scholar] [CrossRef] [PubMed]
- Carlson, M.C.; Erickson, K.I.; Kramer, A.F.; Voss, M.W.; Bolea, N.; Mielke, M.; McGill, S.; Rebok, G.W.; Seeman, T.; Fried, L.P. Evidence for neurocognitive plasticity in at-risk older adults: The experience corps program. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 1275–1282. [Google Scholar] [CrossRef] [PubMed]
- Lovegreen, L.D.; Kahana, E.; Kahana, B. Residential relocation of amenity migrants to Florida: “Unpacking” post-amenity moves. J. Aging Health 2010, 22, 1–28. [Google Scholar] [CrossRef]


{kind=link}
| Fit Statistic | Number of Classes | |||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | |
| AIC a | 43,460.952 | 41,445.795 | 41,026.523 | 40,668.206 | 40,674.206 | |
| BIC a | 43,539.467 | 41,543.938 | 41,144.294 | 40,805.606 | 40,831.235 | |
| Entropy b | 0.81 | 0.74 | 0.75 | 0.75 | ||
| LRT c | <0.001 | <0.001 | <0.001 | <0.05 | ||
| Class proportion d | Class 1 62.9% Class 2 37% | Class 1 12% Class 2 60% Class 3 27% | Class 1 54.2% Class 2 18.5% Class 3 15.3% Class 4 11.8% | Class 1 20.14% Class 2 15.38% Class 3 8.29% Class 4 3.63% Class 5 52.56% | Class 1 20.5% Class 2 2.9% Class 3 16.1% Class 4 9.1% Class 5 0.9% Class 6 50.2% | |
| Entire | Stable High | Stable Moderate | Stable Low | High to Moderate | Moderate to Low | Statistics | |
|---|---|---|---|---|---|---|---|
| 15.38% (n = 1134) | 52.56% (n = 3876) | 3.63% (n = 268) | 20.14% (n = 1485) | 8.29% (n = 611) | |||
| Ascribed | |||||||
| Age (baseline) | 73.44 (6.39) | 70.01 (4.88) | 74.17 (6.36) | 78.79 (7.11) | 71.67 (5.31) | 77.12 (6.52) | F(47,369) = 249.84 ***,a |
| White | 87.33 | 95.24 | 86.51 | 61.94 | 91.99 | 77.74 | (4) = 302.55 *** |
| Women | 58.64 | 61.46 | 54.95 | 64.93 | 61.35 | 67.43 | (4) = 53.76 *** |
| Child hood SES | |||||||
| Parent education (<8 years) | 58.49 | 35.54 | 63.70 | 88.43 | 47.74 | 80.01 | (4) = 586.65 *** |
| Family poor | 34.28 | 29.01 | 35.55 | 45.90 | 31.31 | 37.91 | (4) = 42.40 *** |
| Self-rated health | 2.02 (1.01) | 1.81 (1.01) | 2.06 (1.01) | 2.18 (0.98) | 1.99 (1.00) | 2.13 (1.05) | F(47,369) = 5.66 *** |
| Adulthood SES | |||||||
| Education | 11.92 (3.38) | 13.46 (2.84) | 11.62 (3.19) | 7.79 (4.16) | 12.96 (2.85) | 10.30 (3.78) | F(47,369) = 270.11 *** |
| Income ($, log mean value) | 10.15 (0.74) | 10.55 (0.74) | 10.06 (0.72) | 9.42 (0.63) | 10.36 (0.67) | 9.76 (0.68) | F(47,369) = 263.69 *** |
| Life events and health | |||||||
| Widowed/divorced | 34.66 | 24.34 | 35.66 | 54.10 | 29.23 | 52.05 | (4) = 200.77 *** |
| Nursing home admission | 1.33 | 1.41 | 1.34 | 2.24 | 0.47 | 2.95 | (4) = 22.26 *** |
| Relocation | 33.84 | 39.86 | 32.79 | 22.01 | 36.84 | 27.17 | (4) = 55.05 *** |
| Chronic condition (baseline) | 1.73 (1.25) | 1.45 (1.12) | 1.82 (1.27) | 1.99 (1.38) | 1.59 (1.20) | 1.88 (1.25) | F(47,369) = 28.17 *** |
| No change | 30.07 | 27.43 | 30.91 | 36.19 | 28.28 | 31.26 | (4) = 12.51 ** |
| Increased | 69.93 | 72.57 | 69.09 | 63.81 | 71.72 | 68.74 | |
| Functional limitations (baseline) | 0.50 (1.37) | 0.20 (0.85) | 0.50 (1.33) | 2.26 (2.87) | 0.25 (0.90) | 0.81 (1.75) | F(47,369) = 153.09 *** |
| No change | 48.71 | 71.52 | 46.10 | 15.76 | 56.16 | 19.31 | (8) = 654.07 *** |
| Increased | 45.46 | 24.25 | 47.08 | 72.01 | 39.66 | 76.92 | |
| Decreased | 5.83 | 4.23 | 6.81 | 12.31 | 4.18 | 3.76 |
| Model 1 Ascribed+Childhood+Achieved | Model 2 Life Events+Health in Old Age | Model 3 Social Engagement in Old Age | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Stable High a | Stable Low | High to Moderate | Moderate to Low | Stable High | Stable Low | High to Moderate | Moderate to Low | Stable High | Stable Low | High to Moderate | Moderate to Low | |
| Relative Risk Ratio | Relative Risk Ratio | Relative Risk Ratio | ||||||||||
| Life course factors | ||||||||||||
| Childhood SES | ||||||||||||
| Parent education (<8 years) | 1.14 | 0.78 | 1.06 | 0.80 | 1.13 | 0.81 | 1.08 | 0.82 | 1.13 | 0.82 | 1.08 *** | 0.83 |
| Family poor | 1.02 | 0.95 | 1.00 | 0.96 | 1.03 | 0.93 | 1.02 | 0.97 | 1.03 | 0.94 | 1.01 | 0.97 |
| Self-rated health | 0.88 *** | 0.96 | 1.02 | 1.00 | 0.90 * | 0.93 | 1.03 | 0.99 | 0.90 ** | 0.94 | 1.02 | 0.99 |
| Adulthood SES | ||||||||||||
| Education | 1.15 *** | 0.82 *** | 1.11 *** | 0.92 *** | 1.14 *** | 0.83 *** | 1.11 *** | 0.92 *** | 1.12 *** | 0.84 *** | 1.09 *** | 0.92 *** |
| Income ($, log mean value) | 1.83 *** | 0.56 *** | 1.44 *** | 0.80 ** | 1.82 *** | 0.61 *** | 1.44 *** | 0.85 | 1.75 *** | 0.65 ** | 1.39 *** | 0.86 |
| Life events and health | ||||||||||||
| Widowed/divorced | 1.15 | 0.85 | 1.12 | 1.16 | 1.14 | 0.88 | 1.10 | 1.15 | ||||
| Nursing home admission | 1.51 | 0.94 | 0.43 * | 1.95 * | 1.51 | 1.07 | 0.43 * | 2.18 ** | ||||
| Relocation | 0.97 | 0.91 | 0.93 | 0.98 | 0.96 | 0.89 | 0.93 | 0.97 | ||||
| Chronic condition (baseline) | 0.90 ** | 0.82 *** | 0.93 | 0.91 * | 0.91 ** | 0.81 | 0.94 * | 0.91 * | ||||
| Increased(ref. no change) | 1.03 | 0.83 | 0.93 * | 0.93 | 1.04 | 0.81 *** | 0.99 | 0.90 | ||||
| Functional limitations (baseline) | 0.99 | 1.34 *** | 0.94 | 1.07 * | 1.00 | 1.32 *** | 0.96 | 1.07 * | ||||
| Increased (reference. no change) | 0.54 *** | 3.26 *** | 0.94 | 3.14 *** | 0.59 *** | 3.09 *** | 0.98 | 2.79 *** | ||||
| Decreased | 0.70 | 1.34 | 0.80 | 0.82 | 0.71 | 1.35 | 0.80 | 0.76 | ||||
| Social Engagement | ||||||||||||
| Meet Frequency (baseline) | 1.08 | 0.96 | 1.13 ** | 0.93 | ||||||||
| Increased (ref. no change) | 1.11 | 0.92 | 1.24 * | 0.76 * | ||||||||
| Decreased | 0.78 ** | 0.74 | 0.96 | 1.07 | ||||||||
| Volunteered (baseline) | 1.70 *** | 0.28 * | 1.56 *** | 0.32 *** | ||||||||
| Become volunteering (ref. no change) | 1.34 * | 0.28 * | 1.30 * | 0.46 * | ||||||||
| Become non-volunteering | 0.66 *** | 2.78 | 0.80 * | 4.00 *** | ||||||||
| Constant | 0.28 | 0.36 | 0.14 ** | 0.06 ** | 0.18 | 1.01 | 0.14 ** | 0.11 * | 0.24 | 0.73 | 0.16 * | 0.14 |
| LR chi2(32) = 2215.61 *** | LR chi2(60) = 2242.73 **** | LR chi2(84) = 2005.65 *** | ||||||||||
| ∆χ2 | - | 371.18(32) *** | 109.42(24) *** | |||||||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Kwon, E.; Lee, H. Life Course Trajectories of Later-Life Cognitive Functions: Does Social Engagement in Old Age Matter? Int. J. Environ. Res. Public Health 2017, 14, 393. https://doi.org/10.3390/ijerph14040393
Park S, Kwon E, Lee H. Life Course Trajectories of Later-Life Cognitive Functions: Does Social Engagement in Old Age Matter? International Journal of Environmental Research and Public Health. 2017; 14(4):393. https://doi.org/10.3390/ijerph14040393
Chicago/Turabian StylePark, Sojung, Eunsun Kwon, and Hyunjoo Lee. 2017. "Life Course Trajectories of Later-Life Cognitive Functions: Does Social Engagement in Old Age Matter?" International Journal of Environmental Research and Public Health 14, no. 4: 393. https://doi.org/10.3390/ijerph14040393
APA StylePark, S., Kwon, E., & Lee, H. (2017). Life Course Trajectories of Later-Life Cognitive Functions: Does Social Engagement in Old Age Matter? International Journal of Environmental Research and Public Health, 14(4), 393. https://doi.org/10.3390/ijerph14040393