Spatio-Temporal Pattern and Risk Factor Analysis of Hand, Foot and Mouth Disease Associated with Under-Five Morbidity in the Beijing–Tianjin–Hebei Region of China


Abstract
:1. Introduction
2. Methods
2.1. Material
2.2. Scan Statistics
2.3. GeoDetector
- Enhance: if q(A∩B) > q(A) or q(B)
- Enhance, bivariate: if q(A∩B) > q(A) and q(B)
- Enhance, nonlinear: if q(A∩B) > q(A) + q(B)
- Weaken: if q(A∩B) < q(A) + q(B)
- Weaken, univariate: if q(A∩B) < q(A) or q(B)
- Weaken, nonlinear: if q(A∩B) < q(A) and q(B)
- Independent: if q(A∩B) = q(A) + q(B)
2.4. Spatial Paneled Model
3. Results
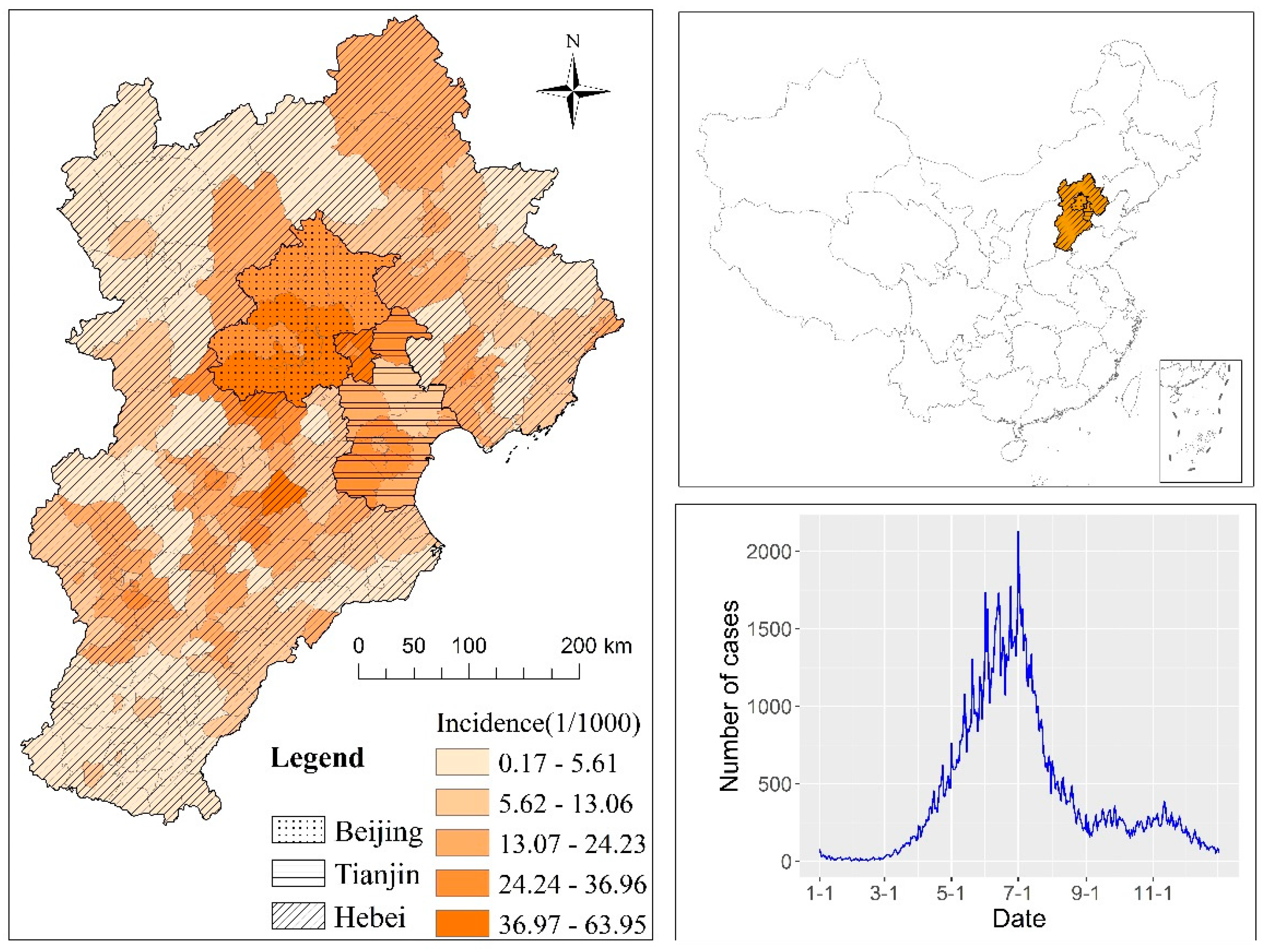
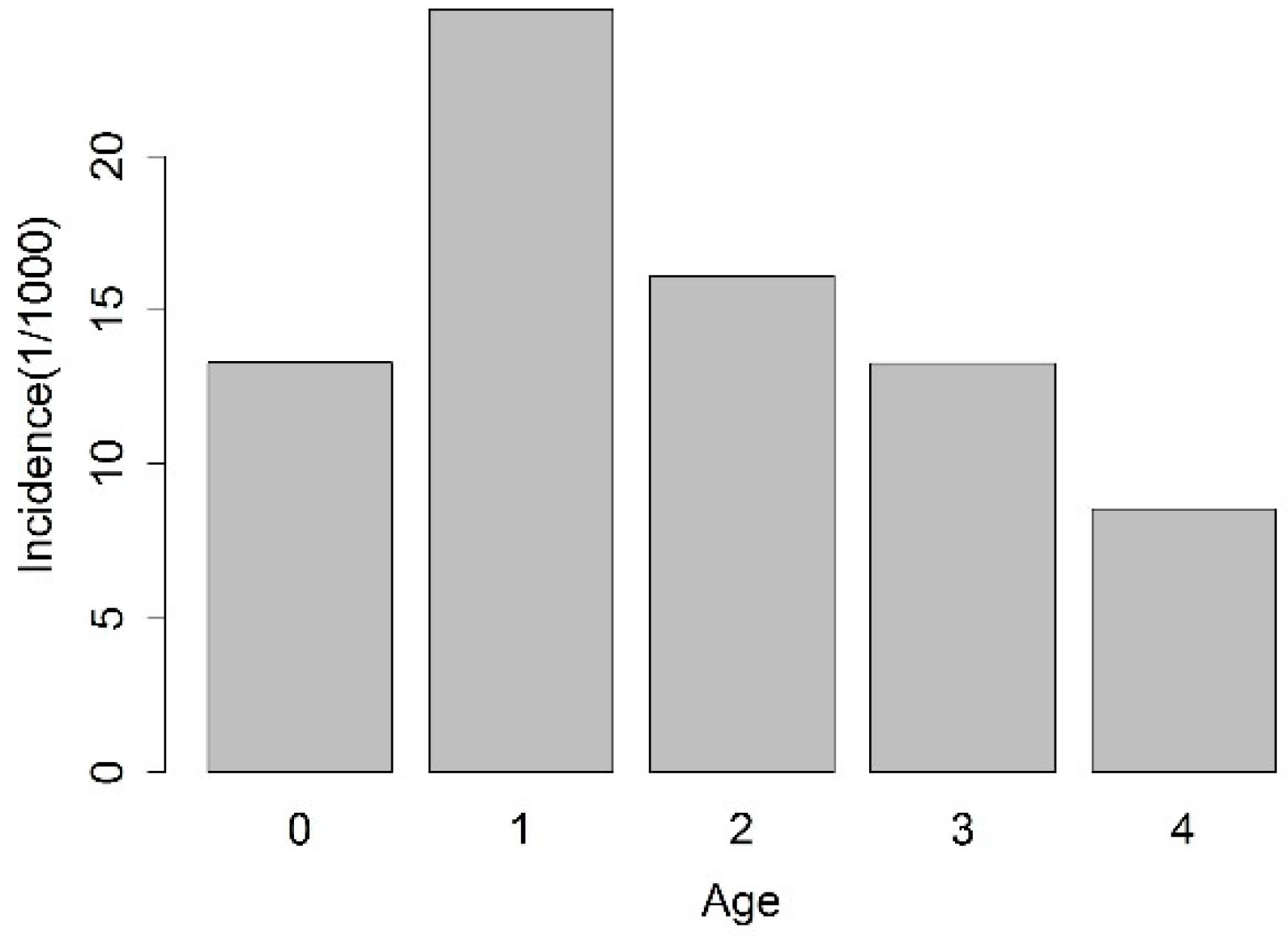
3.1. Descriptive Statistics
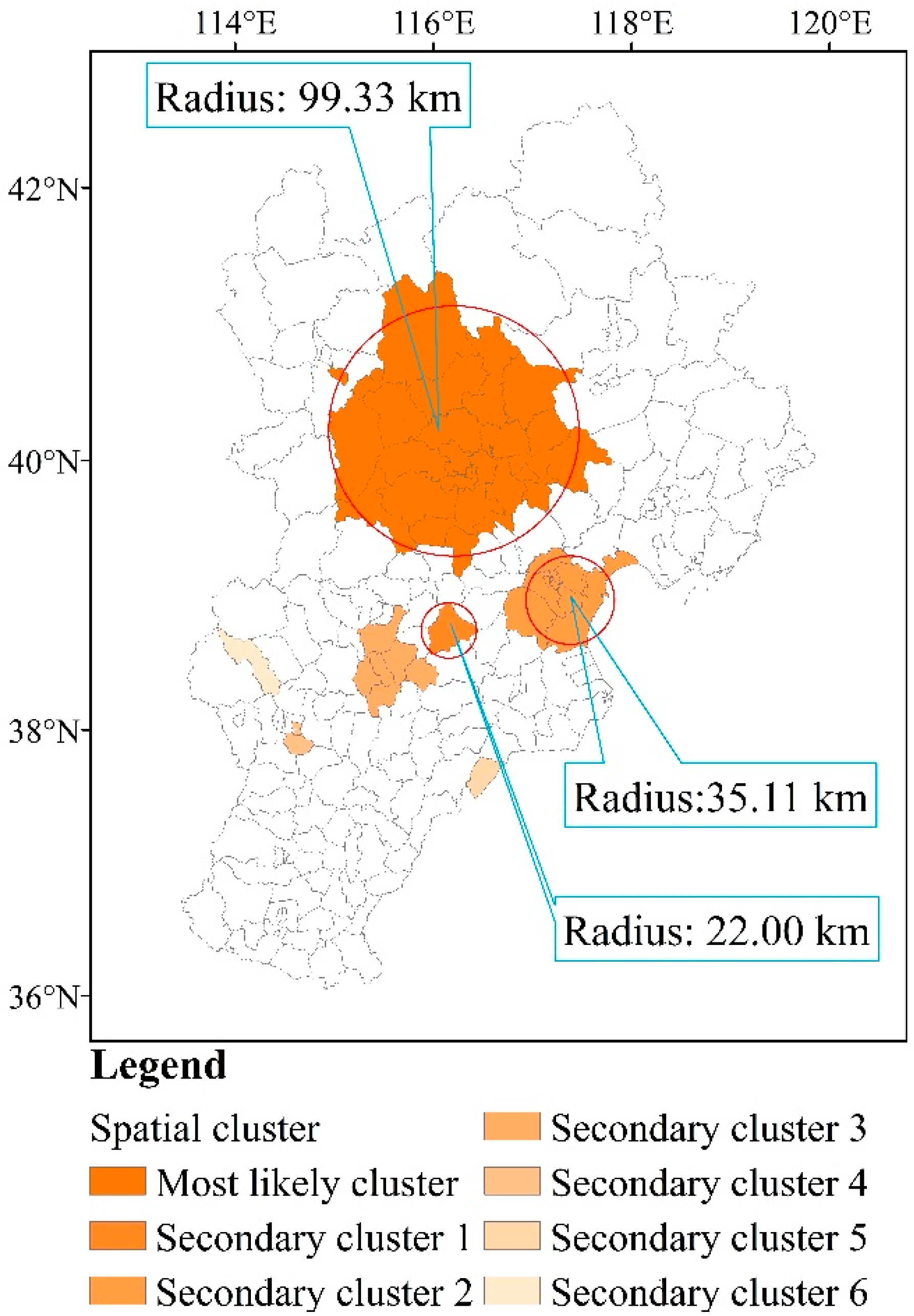
3.2. Spatial Clusters
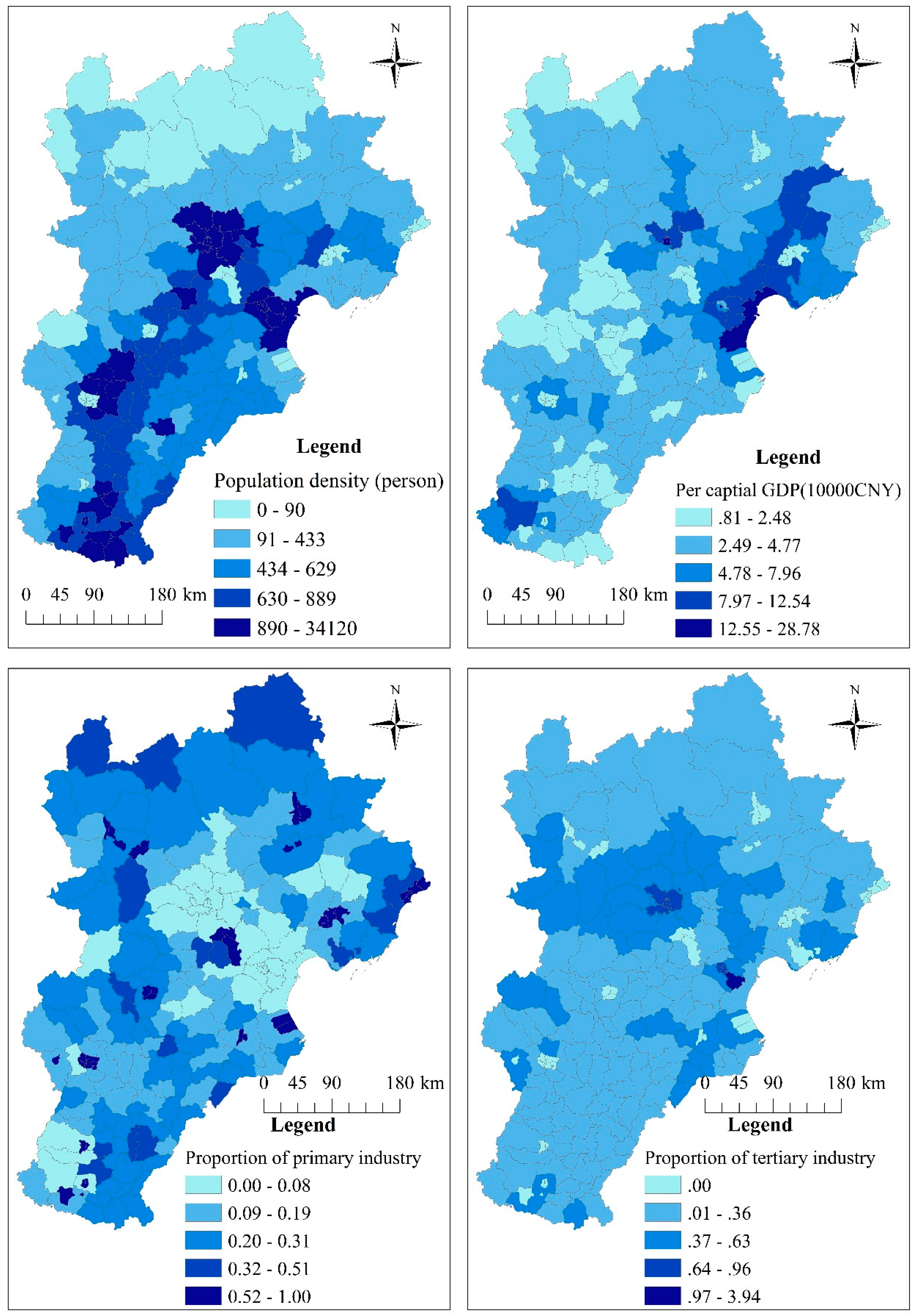
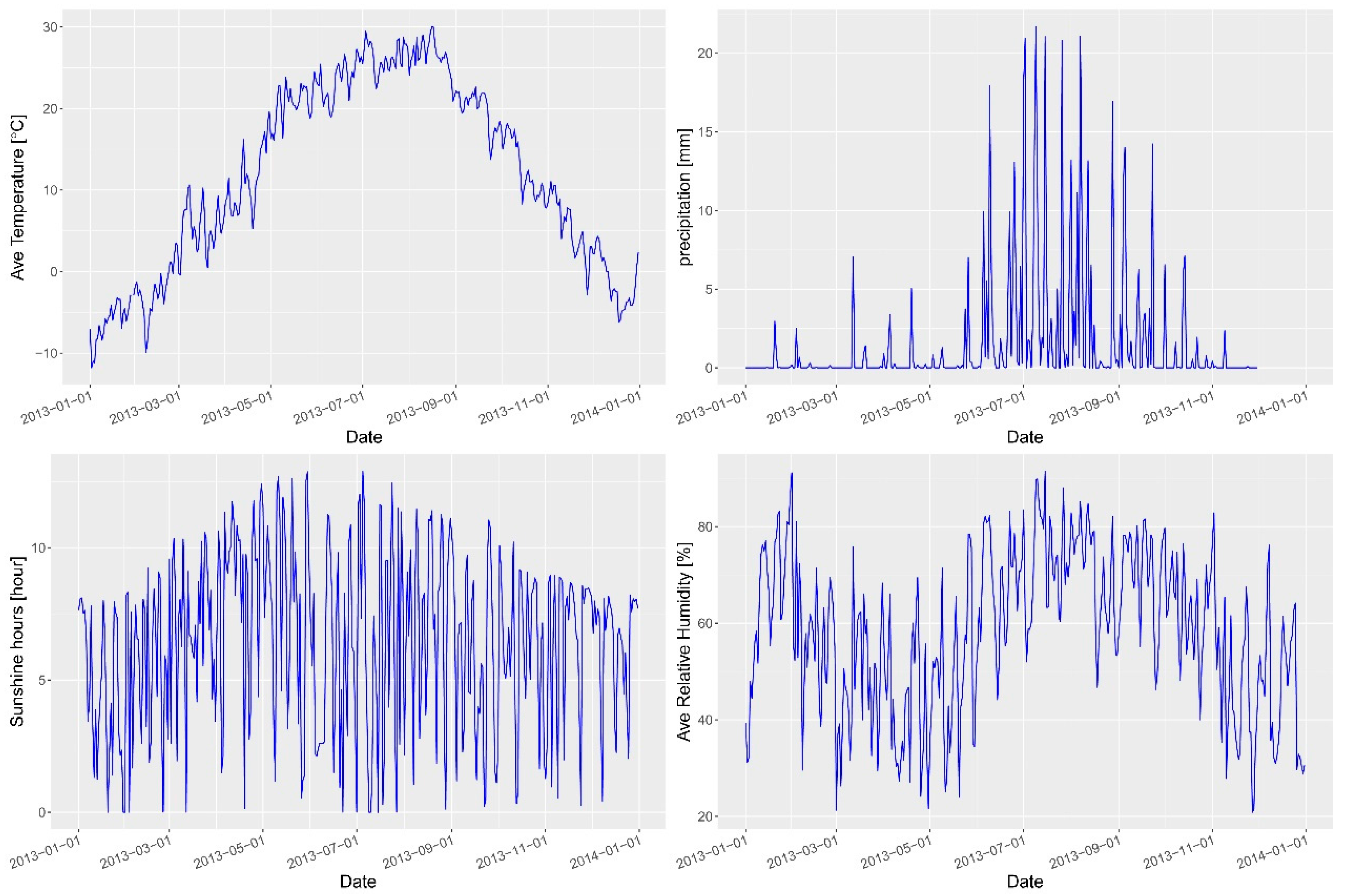
3.3. Risk Factor Detection
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Conflicts of Interest
References
- Xing, W.J.; Liao, Q.H.; Viboud, C.; Zhang, J.; Sun, J.L.; Wu, J.T.; Chang, Z.R.; Liu, F.F.; Fang, V.J.; Zheng, Y.D.; et al. Hand, foot, and mouth disease in China, 2008–2012: An epidemiological study. Lancet Infect. Dis. 2014, 14, 308–318. [Google Scholar] [CrossRef]
- Wang, Y.; Feng, Z.J.; Yang, Y.; Self, S.; Gao, Y.J.; Longini, I.M.; Wakefield, J.; Zhang, J.; Wang, L.P.; Chen, X.; et al. Hand, Foot, and Mouth Disease in China Patterns of Spread and Transmissibility. Epidemiology 2011, 22, 781–792. [Google Scholar] [CrossRef] [PubMed]
- Zeng, M.; Pu, D.B.; Mo, X.W.; Zhu, C.M.; Gong, S.T.; Xu, Y.; Lin, G.Y.; Wu, B.Y.; He, S.L.; Jiao, X.Y.; et al. Children of rural-to-urban migrant workers in China are at a higher risk of contracting severe hand, foot and mouth disease and EV71 infection: A hospital-based study. Emerg. Microbes Infect. 2013, 2, e72. [Google Scholar] [CrossRef] [PubMed]
- National Survey of Epidemic Situation of Notifiable Communicable Diseases in 2015. Available online: http://www.nhfpc.gov.cn/jkj/s3578/201602/b9217ba14e17452aad9e45a5bcce6b65.shtml (accessed on 1 March 2017).
- Zhu, Q.; Hao, Y.T.; Ma, J.Q.; Yu, S.C.; Wang, Y. Surveillance of Hand, Foot, and Mouth Disease in Mainland China (2008–2009). Biomed. Environ. Sci. 2011, 24, 349–356. [Google Scholar] [PubMed]
- Ma, E.; Lam, T.; Chan, K.C.; Wong, C.; Chuang, S.K. Changing Epidemiology of Hand, Foot, and Mouth Disease in Hong Kong, 2001–2009. Jpn. J. Infect. Dis. 2010, 63, 422–426. [Google Scholar] [PubMed]
- Onozuka, D.; Hashizume, M. The influence of temperature and humidity on the incidence of hand, foot, and mouth disease in Japan. Sci. Total Environ. 2011, 410, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.D.; Zeng, D.J.; Wang, Q.Y.; Zheng, X.L.; Wang, F.Y. An epidemiological analysis of the Beijing 2008 Hand-Foot-Mouth epidemic. Chin. Sci. Bull. 2010, 55, 1142–1149. [Google Scholar] [CrossRef]
- Ma, E.; Lam, T.; Wong, C.; Chuang, S.K. Is hand, foot and mouth disease associated with meteorological parameters? Epidemiol. Infect. 2010, 138, 1779–1788. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Lin, H.; Li, X.; Lang, L.; Xiao, X.; Ding, P.; He, P.; Zhang, Y.; Wang, M.; Liu, Q. Short-term effects of meteorological factors on children hand, foot and mouth disease in Guangzhou, China. Int. J. Meteorol. 2014, 58, 1605–1614. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-F.; Xu, C.-D.; Tong, S.-L.; Chen, H.-Y.; Yang, W.-Z. Spatial dynamic patterns of hand-foot-mouth disease in the People’s Republic of China. Geosp. Health 2013, 7, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Hii, Y.L.; Rocklov, J.; Ng, N. Short Term Effects of Weather on Hand, Foot and Mouth Disease. PLoS ONE 2011, 6, e16798. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.G.; Li, Z.J.; Wang, J.F.; Jia, L.; Liao, Y. Determinants of the Incidence of Hand, Foot and Mouth Disease in China Using Geographically Weighted Regression Models. PLoS ONE 2012, 7, e38978. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.F.; Huang, H.M.; Xie, M.; Zhang, J.Q.; Hu, J. Epidemiological analysis of hand-foot-mouth disease in Shanghai Yangpu District during 2005–2008. Chin. J. Dis. Control Prev. 2010, 14, 512–515. [Google Scholar]
- Chen, H.M.; Kang, K.; Wang, H.F.; Wang, Y.X.; Su, J. Analysis of HFMD’s epidemic situation of 2009 in Henan province, forecast of HFMD prevalence trend, prevention and control strategy of 2010. Henan J. Prev. 2010, 21, 161–169. [Google Scholar]
- Cheng, J.; Wu, J.J.; Xu, Z.W.; Zhu, R.; Wang, X.; Li, K.S.; Wen, L.Y.; Yang, H.H.; Su, H. Associations between extreme precipitation and childhood hand, foot and mouth disease in urban and rural areas in Hefei, China. Sci. Total Environ. 2014, 497, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Du, Z.; Wang, X.; Liu, Y.; Yuan, Z.; Liu, Y.; Xue, F. Detecting the association between meteorological factors and hand, foot, and mouth disease using spatial panel data models. Int. J. Infect. Dis. 2015, 34, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Xie, X.; Chen, X.L.; Li, Y.; Lu, Y.; Mei, S.J.; Liao, Y.X.; Lin, H.L. Short-term effects of meteorological factors on hand, foot and mouth disease among children in Shenzhen, China: Non-linearity, threshold and interaction. Sci. Total Environ. 2016, 539, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Wang, J.; Bo, Y.; Xu, C.; Hu, M.; Huang, D. Identification of Health Risks of Hand, Foot and Mouth Disease in China Using the Geographical Detector Technique. Int. J. Environ. Res. Public Health 2014, 11, 3407–3423. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.I.; Ki, H.; Park, S.; Cho., E.; Chun, B.C. Effect of Climatic Factors on Hand, Foot, and Mouth Disease in South Korea, 2010–2013. PLoS ONE 2016, 11, e0157500. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Deng, T.; Yu, S.C.; Gu, J.; Huang, C.R.; Xiao, G.X.; Hao, Y.T. Effect of meteorological variables on the incidence of hand, foot, and mouth disease in children: A time-series analysis in Guangzhou, China. BMC. Infect. Dis. 2013, 13, 8. [Google Scholar] [CrossRef] [PubMed]
- Bo, Y.C.; Song, C.; Wang, J.F.; Li, X.W. Using an autologistic regression model to identify spatial risk factors and spatial risk patterns of hand, foot and mouth disease (HFMD) in Mainland China. BMC. Public Health 2014, 14, 13. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Wang, F.; Wang, B.; Tao, S.; Zhang, H.; Liu, S.; Ramirez, O.; Zeng, Q. Time series analyses of hand, foot and mouth disease integrating weather variables. PLoS ONE 2015, 10, e0117296. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.F.; Guo, Y.S.; Christakos, G.; Yang, W.Z.; Liao, Y.L.; Li, Z.J.; Li, X.Z.; Lai, S.J.; Chen, H.Y. Hand, foot and mouth disease: Spatiotemporal transmission and climate. Int. J. Health Geogr. 2011, 10, 25. [Google Scholar] [CrossRef] [PubMed]
- Kulldorff, M. A spatial scan statistic. Commun. Stat. Theory Methods 1997, 26, 1481–1496. [Google Scholar] [CrossRef]
- Wang, J.F.; Li, X.H.; Christakos., G.; Liao, Y.L.; Zhang, T.; Gu, X.; Zheng, X.Y. Geographical Detectors-Based Health Risk Assessment and its Application in the Neural Tube Defects Study of the Heshun Region, China. Int. J. Geogr. Inf. Sci. 2010, 24, 107–127. [Google Scholar] [CrossRef]
- Hu, Y.; Wang, J.F.; Li, X.H.; Ren, D.; Zhu, J. Geographical Detector-Based Risk Assessment of the Under-Five Mortality in the 2008 Wenchuan Earthquake, China. PLoS ONE 2011, 6, e21427. [Google Scholar] [CrossRef] [PubMed]
- Cao, F.; Ge, Y.; Wang, J. Optimal discretization for geographical detectors-based risk assessment. GISci. Remote Sens. 2013, 50, 78–92. [Google Scholar]
- Wang, J.F.; Zhang, T.L.; Fu, B.J. A measure of spatial stratified heterogeneity. Ecol. Indic. 2016, 67, 250–256. [Google Scholar] [CrossRef]
- Fischer, M.M.; Getis, A. Handbook of Applied Spatial Analysis: Software Tools, Methods and Applications; Springer: Berlin, Germany, 2010. [Google Scholar]
- Haining, R.P. Spatial Data Analysis: Theory and Practice; Cambridge University Press: Cambridge, UK, 2003. [Google Scholar]
- Lin, H.L.; Sun, L.M.; Lin, J.Y.; He, J.F.; Deng, A.P.; Kang, M.; Zeng, H.R.; Ma, W.J.; Zhang, Y.H. Protective effect of exclusive breastfeeding against hand, foot and mouth disease. BMC Infect. Dis. 2014, 14, 7. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.Y.; King, C.C.; Hsu, K.H.; Ning, H.C.; Tsao, K.C.; Li, C.C.; Huang, Y.C.; Shih, S.R.; Chiou, S.T.; Chen, P.Y.; et al. Risk factors of enterovirus 71 infection and associated hand, foot, and mouth disease/herpangina in children during an epidemic in Taiwan. Pediatrics 2002, 109, e88. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, J.; Zhang, X. Modeling and Preventive Measures of Hand, Foot and Mouth Disease (HFMD) in China. Int. J. Environ. Res. Pubulic Health 2014, 11, 3108–3117. [Google Scholar] [CrossRef] [PubMed]
- Openshaw, S. The Modifiable Areal Unit Problem; Geo Books: Norwich, UK, 1983; Volume 38. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cluster | Center | Number of Counties | Observed Cases | Expected Cases | LLR | RR | p Value |
|---|---|---|---|---|---|---|---|
| 1 * | (116.20° E, 40.22° N) | 29 | 35,877 | 16,059 | 11,930 | 3.04 | 0.00 |
| 2 | (116.16° E, 38.74° N) | 1 | 3507 | 1013 | 1894 | 3.55 | 0.00 |
| 3 | (117.38° E, 38.97° N) | 12 | 7969 | 5475 | 533 | 1.49 | 0.00 |
| 4 | (115.48° E, 38.45° N) | 6 | 3788 | 2575 | 257 | 1.49 | 0.00 |
| 5 | (114.63° E, 37.89° N) | 2 | 942 | 433 | 224 | 2.18 | 0.00 |
| 6 | (116.50° E, 37.66° N) | 1 | 391 | 282 | 18 | 1.38 | 0.00 |
| 7 | (114.17° E, 38.51° N) | 1 | 391 | 313 | 8 | 1.24 | 0.01 |
| Variables | Temperature | Precipitation | Relative Humidity | Sunshine Hours | Wind Speed |
|---|---|---|---|---|---|
| Temperature | 0.57 | ||||
| Precipitation | 0.60 | 0.21 | |||
| Relative humidity | 0.64 | 0.30 | 0.13 | ||
| Sunshine hours | 0.61 | 0.30 | 0.37 | 0.12 | |
| Wind speed | 0.55 | 0.23 | 0.14 | 0.15 | 0.02 |
| Variables | Coefficient | S.E. | t | p |
|---|---|---|---|---|
| spatial weight | 0.55 | 0.023 | 23.40 | 0.000 |
| average temperature (°C) | 0.076 | 0.013 | 5.53 | 0.000 |
| precipitation (mm) | −0.0038 | 0.0011 | −3.29 | 0.001 |
| sunshine hours (h) | −0.0015 | 0.00059 | −2.58 | 0.009 |
| Variables | Prim. ind. | GDP per Capita | Tert. ind. | Popu. den. |
|---|---|---|---|---|
| Prim. ind. | 0.32 | |||
| GDP per capita | 0.36 | 0.22 | ||
| Tert. ind. | 0.48 | 0.33 | 0.17 | |
| Popu. den. | 0.42 | 0.42 | 0.34 | 0.15 |
© 2017 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, C. Spatio-Temporal Pattern and Risk Factor Analysis of Hand, Foot and Mouth Disease Associated with Under-Five Morbidity in the Beijing–Tianjin–Hebei Region of China. Int. J. Environ. Res. Public Health 2017, 14, 416. https://doi.org/10.3390/ijerph14040416
Xu C. Spatio-Temporal Pattern and Risk Factor Analysis of Hand, Foot and Mouth Disease Associated with Under-Five Morbidity in the Beijing–Tianjin–Hebei Region of China. International Journal of Environmental Research and Public Health. 2017; 14(4):416. https://doi.org/10.3390/ijerph14040416
Chicago/Turabian StyleXu, Chengdong. 2017. "Spatio-Temporal Pattern and Risk Factor Analysis of Hand, Foot and Mouth Disease Associated with Under-Five Morbidity in the Beijing–Tianjin–Hebei Region of China" International Journal of Environmental Research and Public Health 14, no. 4: 416. https://doi.org/10.3390/ijerph14040416
APA StyleXu, C. (2017). Spatio-Temporal Pattern and Risk Factor Analysis of Hand, Foot and Mouth Disease Associated with Under-Five Morbidity in the Beijing–Tianjin–Hebei Region of China. International Journal of Environmental Research and Public Health, 14(4), 416. https://doi.org/10.3390/ijerph14040416