
Assessing the Racial and Ethnic Disparities in Breast Cancer Mortality in the United States

 ,
,  ,
,
Abstract
:1. Introduction
2. Methodology
3. Results and Discussion
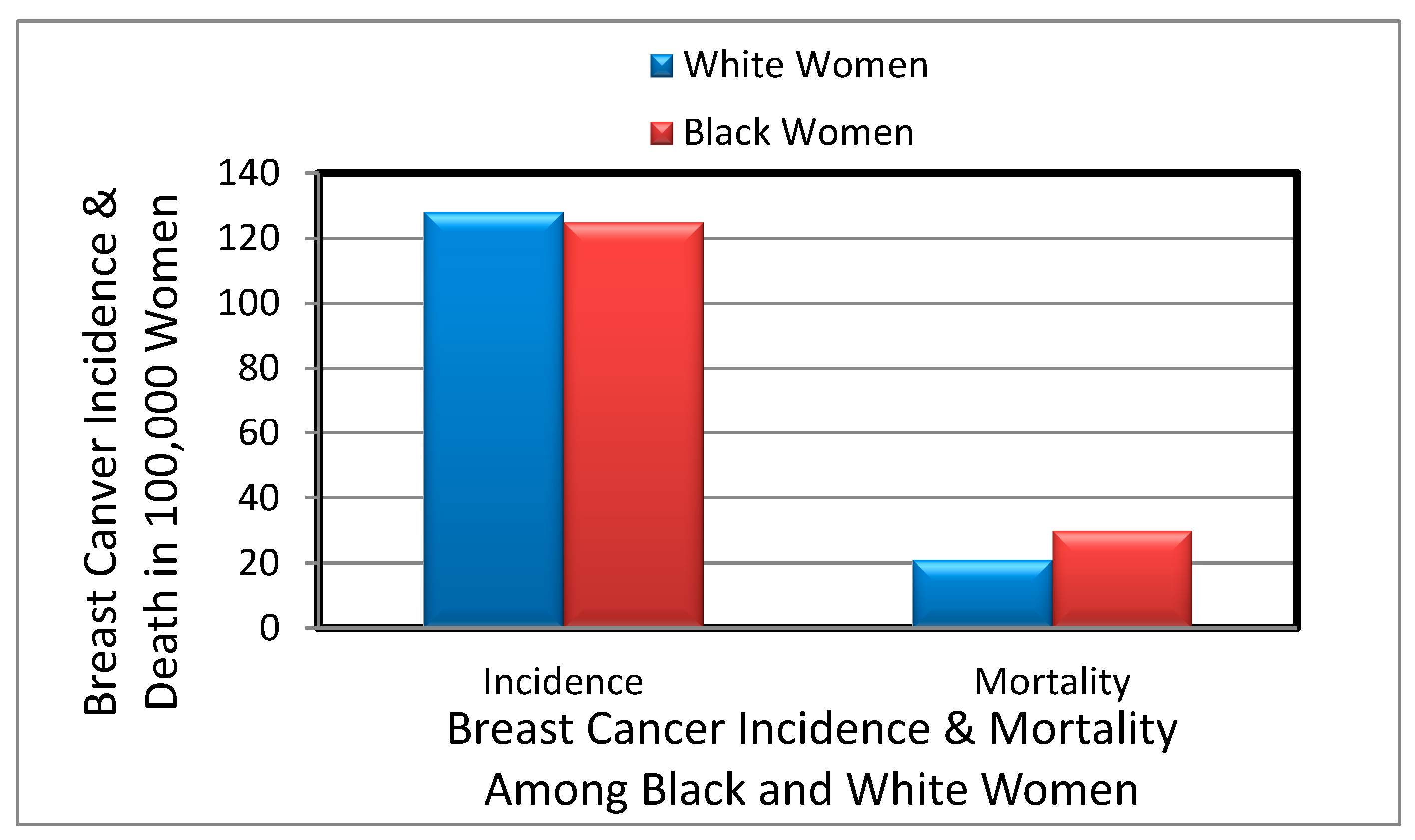
3.1. Overview of Breast Cancer
3.2. Racial/Ethnic Disparities in Breast Cancer
3.3. Majors Risk Factors in Breast Cancer Affecting Minority Populations
3.3.1. Age and Sex Risk Factors in Breast Cancer
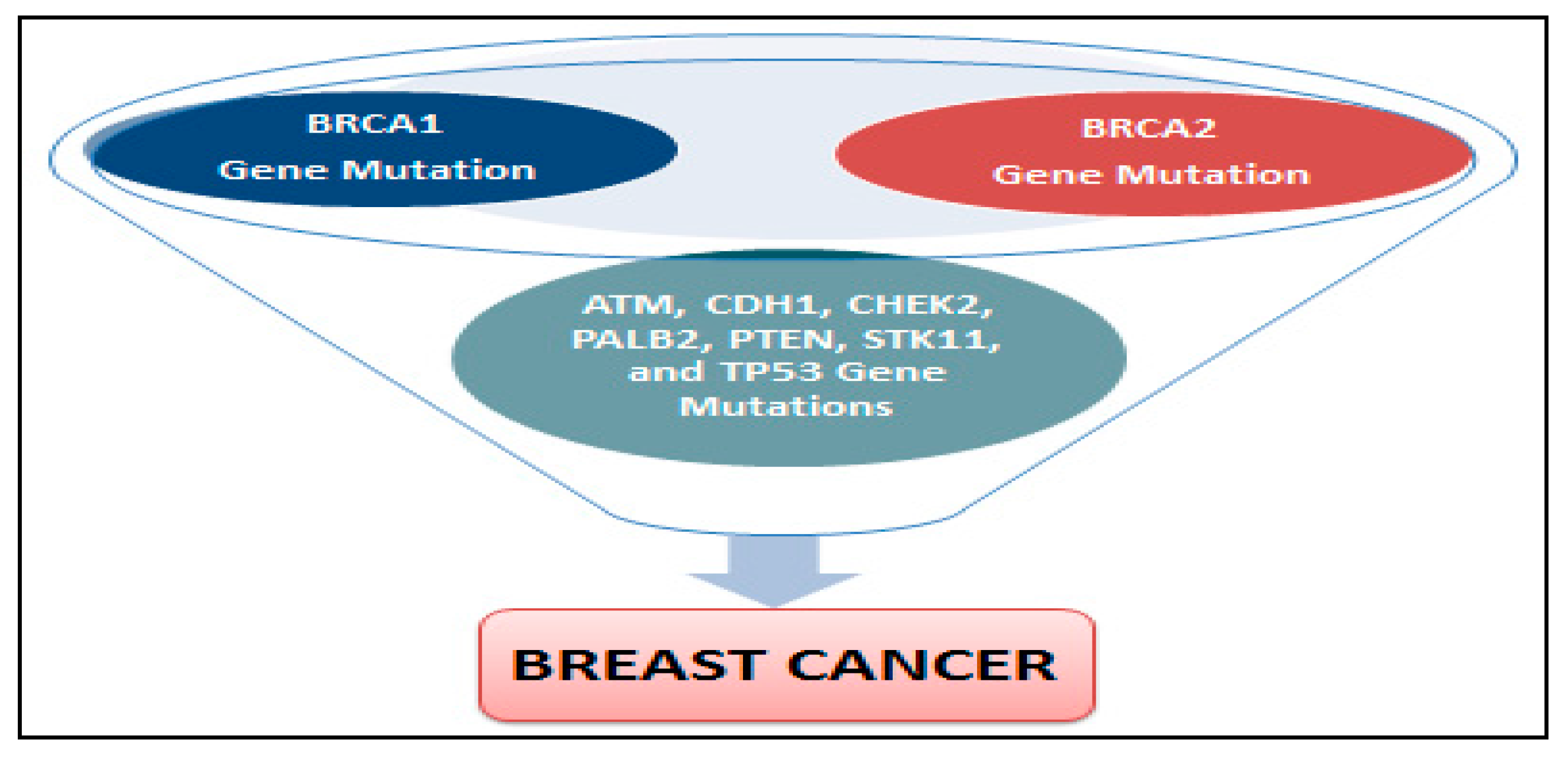
3.3.2. Genetic Risk Factors in Breast Cancer
3.3.3. Lack of Physical Activity Risk Factors in Breast Cancer
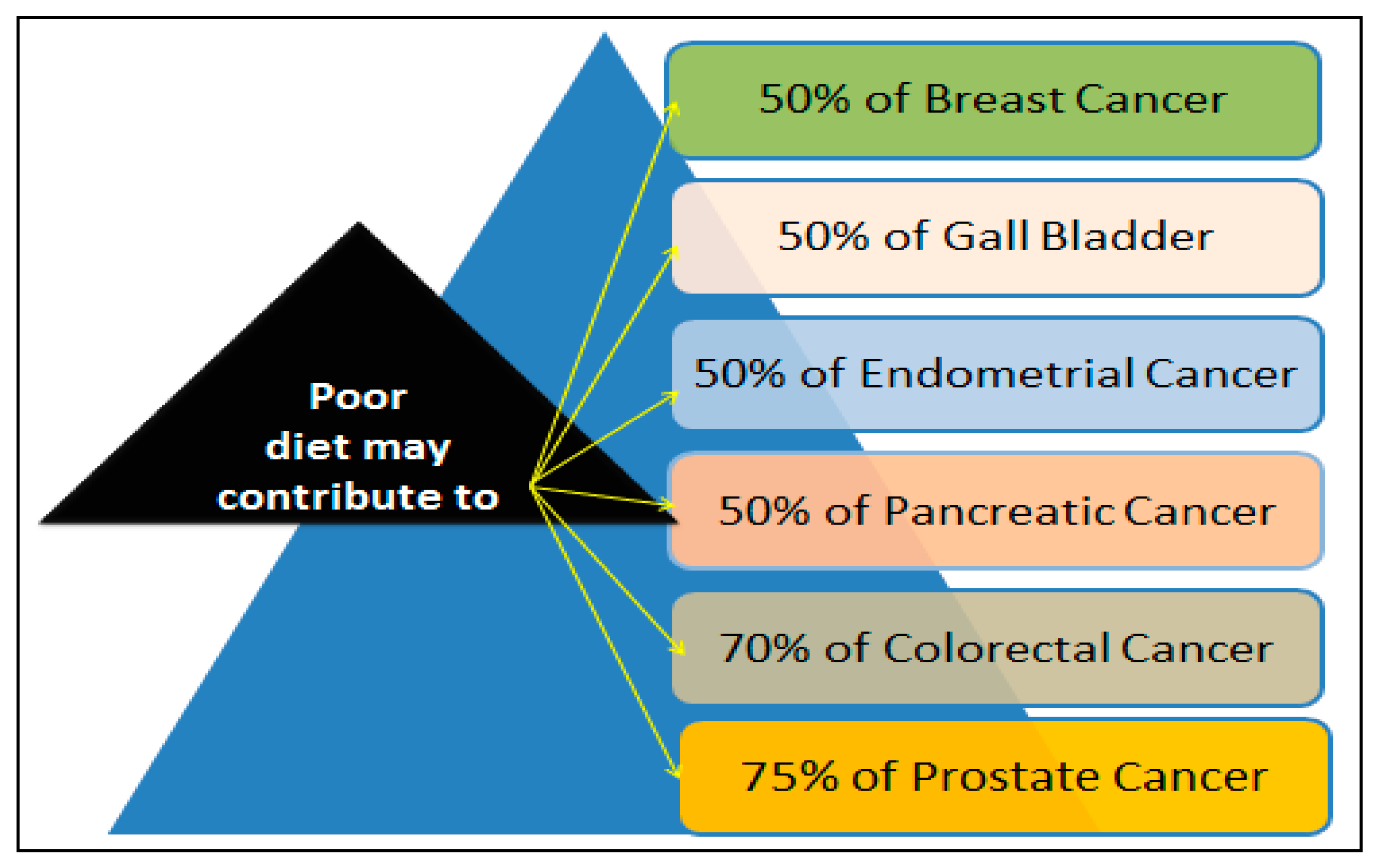
3.3.4. Poor Diet, Obesity, and alcohol Consumption Risk Factors in Breast Cancer
3.4. Breast Cancer Prevention, Treatment and Health Disparity
3.5. Mechanisms of Apoptosis Resistance in Breast Cancer Treatment
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stata Database: Incidence SEER 18 Regs Research Data + Hurricane Katrina Impacted Louisiana Cases, Nov. 2013 Sub (20002011) <Katrina/Rita Population Adjustment> Linked to County Attributes Total US, 19692012 Counties; National Cancer Institute, Division of Cancer Control and Population Sciences, Surveillance Research Program, Surveillance Systems Branch: Bethesda, MD, USA, 2014.
- Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Mortality—All COD, Aggregated With State Total US (19692010) <Katrina/Rita Population Adjustment>; National Cancer Institute, Division of Cancer Control and Population Sciences, Surveillance Research Program, Surveillance Systems Branch: Bethesda, MD, USA, 2013.
- Pinheiro, S.P.; Holmes, M.D.; Pollak, M.N.; Barbieri, R.L.; Hankinson, S.E. Racial differences in premenopausal endogenous hormones. Cancer Epidemiol. Biomark. Prev. 2005, 14, 2147–2153. [Google Scholar] [CrossRef] [PubMed]
- Hall, I.J.; Moorman, P.G.; Millikan, R.C.; Newman, B. Comparative analysis of breast cancer risk factors among African-American women and White women. Am. J. Epidemiol. 2005, 161, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Chlebowski, R.T.; Chen, Z.; Anderson, G.L.; Rohan, T.; Aragaki, A.; Lane, D.; Dolan, N.C.; Paskett, E.D.; McTiernan, A.; Hubbell, F.A.; et al. Ethnicity and breast cancer: Factors influencing differences in incidence and outcome. J. Natl. Cancer Inst. 2005, 97, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Haiman, C.A.; Chen, G.K.; Vachon, C.M.; Canzian, F.; Dunning, A.; Millikan, R.C.; Wang, X.; Ademuyiwa, F.; Ahmed, S.; Ambrosone, C.B.; et al. A common variant at the TERT-CLPTM1L locus is associated with estrogen receptor-negative breast cancer. Nat. Genet. 2011, 43, 1210–1214. [Google Scholar] [CrossRef] [PubMed]
- Kato, I.; Cichon, M.; Yee, C.L.; Land, S.; Korczak, J.F. African American-preponderant single nucleotide polymorphisms (SNPs) and risk of breast cancer. Cancer Epidemiol. 2009, 33, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Ray, M.; Polite, B.N. Triple-negative breast cancers: A view from 10,000 feet. Cancer J. 2010, 16, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Setiawan, V.W.; Monroe, K.R.; Wilkens, L.R.; Kolonel, L.N.; Pike, M.C.; Henderson, B.E. Breast cancer risk factors defined by estrogen and progesterone receptor status: The multiethnic cohort study. Am. J. Epidemiol. 2009, 169, 1251–1259. [Google Scholar] [CrossRef] [PubMed]
- Dunnwald, L.K.; Rossing, M.A.; Li, C.I. Hormone receptor status, tumor characteristics, and prognosis: A prospective cohort of breast cancer patients. Breast Cancer Res. 2007, 9, R6. [Google Scholar] [CrossRef] [PubMed]
- Porter, P.L.; Lund, M.J.; Lin, M.G.; Yuan, X.; Liff, J.M.; Flagg, E.W.; Coates, R.J.; Eley, J.W. Racial differences in the expression of cell cycle-regulatory proteins in breast carcinoma. Cancer 2004, 100, 2533–2542. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.N.; Boersma, B.J.; Yi, M.; Reimers, M.; Howe, T.M.; Yfantis, H.G.; Tsai, Y.C.; Williams, E.H.; Lee, D.H.; Stephens, R.M.; et al. Differences in the tumor microenvironment between African-American and European-American breast cancer patients. PLoS ONE 2009, 4, e4531. [Google Scholar] [CrossRef] [PubMed]
- Gukas, I.D.; Girling, A.C.; Mandong, B.M.; Prime, W.; Jennings, B.A.; Leinster, S.J. A comparison of clinicopathological features and molecular markers in British and Nigerian women with breast cancer. Clin. Med. Oncol. 2008, 2, 347–351. [Google Scholar] [CrossRef]
- Mehrotra, J.; Ganpat, M.M.; Kanaan, Y.; Fackler, M.J.; McVeigh, M.; Lahti-Domenici, J.; Polyak, K.; Argani, P.; Naab, T.; Garrett, E.; et al. Estrogen receptor/progesterone receptor-negative breast cancers of young African-American women have a higher frequency of methylation of multiple genes than those of Caucasian women. Clin. Cancer Res. 2004, 10, 2052–2057. [Google Scholar] [CrossRef] [PubMed]
- Dookeran, K.A.; Dignam, J.J.; Ferrer, K.; Sekosan, M.; McCaskill-Stevens, W.; Gehlert, S. p53 as a marker of prognosis in African-American women with breast cancer. Ann. Surg. Oncol. 2010, 17, 1398–1405. [Google Scholar] [CrossRef] [PubMed]
- Loo, L.W.; Wang, Y.; Flynn, E.M.; Lund, M.J.; Bowles, E.J.; Buist, D.S.; Liff, J.M.; Flagg, E.W.; Coates, R.J.; Eley, J.W.; et al. Genome-wide copy number alterations in subtypes of invasive breast cancers in young white and African American women. Breast Cancer Res. Treat. 2011, 127, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Yip, C.H.; Smith, R.A.; Anderson, B.O.; Miller, A.B.; Thomas, D.B.; Ang, E.S.; Caffarella, R.S.; Corbex, M.; Kreps, G.L.; McTiernan, A. Guideline implementation for breast healthcare in low- and middle-income countries: Early detection resource allocation. Cancer 2008, 113, 2244–2256. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Tammemagi, C.M. Racial/ethnic disparities in breast and gynecologic cancer treatment and outcomes. Curr. Opin. Obstet. Gynecol. 2007, 19, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Hirschman, J.; Whitman, S.; Ansell, D. The Black:White disparity in breast cancer mortality: The example of Chicago. Cancer Causes Control 2007, 18, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Coleman, M.P.; Quaresma, M.; Berrino, F.; Lutz, J.M.; De Angelis, R.; Capocaccia, R.; Baili, P.; Rachet, B.; Gatta, G.; Hakulinen, T.; et al. Cancer survival in five continents: A worldwide population-based study (CONCORD). Lancet Oncol. 2008, 9, 730–756. [Google Scholar] [CrossRef]
- Howlader, N.; Noone, A.M.; Krapch, O.M.; Miller, D.; Bishop, K.; Altekruse, S.F.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; et al. SEER Cancer Statistics Review, 1975–2013; National Cancer Institute: Bethesda, MD, USA, 2016.
- American Cancer Society. Breast Cancer Facts & Figures, 2015–2016; American Cancer Society: Atlanta, GA, USA, 2015. [Google Scholar]
- American Cancer Society. Cancer Facts and Figures for African Americans 2016–2018; American Cancer Society: Atlanta, GA, USA, 2016. [Google Scholar]
- Ademuyiwa, F.O.; Groman, A.; O’Connor, T.; Ambrosone, C.; Watroba, N.; Stephen, B.; Edge, S.B. Impact of body mass index on clinical outcomes in triple negative breast cancer. Cancer 2011, 117, 4132–4140. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society (ACS). Cancer Facts and Figures for African Americans 2011–2012; American Cancer Society: Atlanta, GA, USA, 2011. [Google Scholar]
- Gail, M.H.; Costantino, J.P.; Bryant, J.; Croyle, R.; Freedman, L.; Helzlsouer, K.; Vogel, V. Weighing the risks and benefits of Tamoxifen treatment for preventing breast cancer. J. Natl. Cancer Inst. 1999, 91, 1829–1846. [Google Scholar] [CrossRef] [PubMed]
- Connor, C.S.; Touijer, A.K.; Krishnan, L.; Mayo, M.S. Local recurrence following breast conservation therapy in African-American women with invasive breast cancer. Am. J. Surg. 2000, 179, 22–26. [Google Scholar] [CrossRef]
- American Cancer Society (ACS). African American 2013–2014 Cancer Facts; ACS: Atlanta, GA, USA, 2013. [Google Scholar]
- Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: North American Association of Central Caner Registries (NAACCR) Incidence-CiNA Analytic File, 1995–2012, Custom File with County, North American Association of Central Cancer Registries; National Cancer Institute, Division of Cancer Control and Population Sciences, Surveillance Research Program, Cancer Statistics Branch: Bethesda, MD, USA, 2015.
- Parkin, D.M.; Boyd, L.; Walker, L.C. The fraction of cancer attributable to lifestyle and environmental factors in the UK in 2010. Br. J. Cancer 2011, 105, S77–S81. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Noone, A.M.; Krapcho Garshell, J.; Miller, D.; Altekruse, S.F.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; et al. SEER Cancer Statistics Review, 1975–2012; Based on November 2014 SEER Data Submission, Posted to the SEER Web Site April 2015; National Cancer Institute: Bethesda, MD, USA, 2015.
- Hartmann, L.C.; Sellers, T.A.; Frost, M.H.; Frost, M.H.; Lingle, W.L.; Degnim, A.C.; Ghosh, K.; Vierkant, R.A.; Maloney, S.D.; Pankratz, V.S.; et al. Benign breast disease and the risk of breast cancer. N. Engl. J. Med. 2005, 353, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Eberl, M.M.; Sunga, A.Y.; Farrell, C.D.; Mahoney, M.C. Patients with a Family History of Cancer: Identification and Management. JABFM 2005, 18, 211–217. [Google Scholar] [CrossRef]
- Campeau, P.M.; Foulkes, W.D.; Tischkowitz, M.D. Hereditary breast cancer: New genetic developments, new therapeutic avenues. Hum. Genet. 2008, 124, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Pal, T.; Permuth-Wey, J.; Betts, J.A.; Krischer, J.P.; Fiorica, J.; Arango, H.; LaPolla, J.; Hoffman, M.; Martino, M.A.; Wakeley, K.; et al. BRCA1 and BRCA2 mutations account for a large proportion of ovarian carcinoma cases. Cancer 2005, 104, 2807–2816. [Google Scholar] [CrossRef] [PubMed]
- Emedicinehealth. Breast Cancer. Available online: http://www.emedicinehealth.com/breast_cancer/page2_em.htm (accessed on 20 March 2010).
- Easton, D.F. How many more breast cancer predisposition genes are there? Breast Cancer Res. 1999, 1, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Bièche, I.; Lidereau, R. Genetic alterations in breast cancer. Genes Chrom. Cancer 1995, 14, 227–251. [Google Scholar] [CrossRef] [PubMed]
- McBride, O.W.; Merry, D.; Givol, D. The gene for human p53 cellular tumor antigen is located on chromosome 17 short arm (17p13). Proc. Natl. Acad. Sci. USA 1986, 83, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.; Mohandas, T.; Wolf, D.; Prokocimer, M.; Rotter, V.; Koeffler, H.P. Human p53 gene localized to short arm of chromosome 17. Nature 1986, 319, 783–784. [Google Scholar] [CrossRef] [PubMed]
- Miki, Y.; Swensen, J.; Shattuck-Eidens, D.; Futreal, P.A.; Harshman, K.; Tavtigian, S.; Liu, Q.; Cochran, C.; Bennett, L.M.; Ding, W.; et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science 1994, 266, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Wooster, R.; Bignell, G.; Lancaster, J.; Swift, S.; Seal, S.; Mangion, J.; Collins, N.; Gregory, S.; Gumbs, C.; Micklem, G. Identification of the breast cancer susceptibility gene BRCA2. Nature 1995, 378, 789–792. [Google Scholar] [CrossRef] [PubMed]
- Elledge, R.M.; Clark, G.M.; Chamness, G.C.; Osborne, C.K. Tumor biologic factors and breast cancer prognosis among white, Hispanic, and black women in the United States. J. Natl. Cancer Inst. 1994, 86, 705–712. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Genetics of Breast and Gynecologic Cancers (PDQ®)—Health Professional Version. Available online: http://www.cancer.gov/types/breast/hp/breast-ovarian-genetics-pdq#section/88 (accessed on 30 March 2017).
- Irigaray, P.; Newby, J.A.; Clapp, R.; Hardell, L.; Howard, V.; Montagnier, L.; Epstein, S.; Belpomme, D. Lifestyle-related factors and environmental agents causing cancer: An overview. Biomed. Pharmacother. 2007, 61, 640–658. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Oguma, Y. Physical activity. In Cancer Epidemiology and Prevention, 3rd ed.; Schottenfeld, D., Fraumeni, J.F., Eds.; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- McTiernan, A. (Ed.) Cancer Prevention and Management through Exercise and Weight Control; Taylor & Francis Group, LLC: Boca Raton, FL, USA, 2006. [Google Scholar]
- Lynch, B.M.; Neilson, H.K.; Friedenreich, C.M. Physical activity and breast cancer prevention. Recent Results Cancer Res. 2011, 186, 13–42. [Google Scholar] [PubMed]
- Albuquerque, R.C.; Baltar, V.T.; Marchioni, D.M. Breast cancer and dietary patterns: A systematic review. Nutr. Rev. 2014, 72, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, P.; Rinaldi, S.; Jenab, M.; Lukanova, A.; Olsen, A.; Tjønneland, A.; Overvad, K.; Clavel-Chapelon, F.; Fagherazzi, G.; Touillaud, M.; et al. Dietary fiber intake and risk of hormonal receptor-defined breast cancer in the European Prospective Investigation into Cancer and Nutrition study. Am. J. Clin. Nutr. 2013, 97, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Deschasaux, M.; Zelek, L.; Pouchieu, C.; His, M.; Hercberg, S.; Galan, P.; Latino-Martel, P.; Touvier, M. Prospective association between dietary fiber intake and breast cancer risk. PLoS ONE 2013, 8, e79718. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Chan, D.S.; Vieira, A.R.; Rosenblatt, D.A.; Vieira, R.; Greenwood, D.C.; Norat, T. Fruits, vegetables and breast cancer risk: A systematic review and meta-analysis of prospective studies. Breast Cancer Res. Treat. 2012, 134, 479–493. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Chiuve, S.E.; Willett, W.C.; Hankinson, S.E.; Hu, F.B.; Holmes, M.D. Intake of specific fruits and vegetables in relation to risk of estrogen receptor-negative breast cancer among post-menopausal women. Breast Cancer Res. Treat. 2013, 138, 925–930. [Google Scholar] [CrossRef] [PubMed]
- Stolley, M.R.; Sharp, L.K.; Wells, A.M.; Simon, N.; Schiffer, L. Health behaviors and breast cancer: Experiences of urban African American women. Health Educ. Behav. 2006, 33, 604–624. [Google Scholar] [CrossRef] [PubMed]
- Ligibel, J. Obesity and Breast Cancer. Oncology 2011, 25, 994–1000. [Google Scholar] [PubMed]
- Smith-Warner, S.A.; Spiegelman, D.; Adami, H.O.; Beeson, W.L.; van den Brandt, P.A.; Folsom, A.R.; Fraser, G.E.; Freudenheim, J.L.; Goldbohm, R.A.; Graham, S.; et al. Types of dietary fat and breast cancer: A pooled analysis of cohort studies. Int. J. Cancer 2001, 92, 767–774. [Google Scholar] [CrossRef]
- Willett, W.C. Diet and cancer. Oncologist 2000, 5, 393–404. [Google Scholar] [CrossRef] [PubMed]
- Bowlin, S.J.; Leske, M.C.; Varma, A.; Nasca, P.; Weinstein, A.; Caplan, L. Breast cancer risk and alcohol consumption: Results from a large case–control study. Int. J. Epidemiol. 1997, 26, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Ewertz, M. Alcohol consumption and breast cancer risk in Denmark. Cancer Causes Control 1991, 2, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Nagata, C.; Kabuto, M.; Takatsuka, N.; Shimizu, H. Associations of alcohol, height, and reproductive factors with serum hormone concentrations in postmenopausal Japanese women. Steroid hormones in Japanese postmenopausal women. Breast Cancer Res. Treat. 1997, 44, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Collaborative Group on Hormonal Factors in Breast Cancer. Alcohol, tobacco and breast cancer—Collaborative reanalysis of individual data from 53 epidemiological studies, including 58,515 women with breast cancer and 95067 women without the disease. Br. J. Cancer 2002, 87, 1234–1245. [Google Scholar]
- Connolly, B.S.; Barnett, C.; Vogt, K.N.; Li, T.; Stone, J.; Boyd, N.F. A meta-analysis of published literature on waist-to-hip ratio and risk of breast cancer. Nutr. Cancer 2002, 44, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Rose, D.P.; Komninou, D.; Stephenson, G.D. Obesity, adipocytokines, and insulin resistance in breast cancer. Obes. Rev. 2004, 5, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Lamon-Fava, S.; Barnett, J.B.; Woods, M.N.; McCormack, C.; McNamara, J.R.; Schaefer, E.J.; Longcope, C.; Rosner, B.; Gorbach, S.L. Differences in serum sex hormone and plasma lipid levels in Caucasian and African-American premenopausal women. J. Clin. Endocrinol. Metab. 2005, 90, 4516–4520. [Google Scholar] [CrossRef] [PubMed]
- Sephton, S.E.; Sapolsky, R.M.; Kraemer, H.C.; Spiegel, D. Diurnal cortisol rhythm as a predictor of breast cancer survival. J. Natl. Cancer Inst. 2000, 92, 994–1000. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Prevalence of regular physical activity among adults—United States, 2001 and 2005. Morb. Mortal. Wkly. Rep. 2007, 56, 1209–1212. [Google Scholar]
- Colditz, G.A.; Bohlke, K. Priorities for the primary prevention of breast cancer. CA Cancer J. Clin. 2014, 64, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Optenberg, S.A.; Thompson, I.M.; Friedrichs, P.; Wojcik, B.; Stein, C.R.; Kramer, B. Race, treatment, and long-term survival from prostate cancer in an equal-access medical care delivery system. JAMA 1995, 274, 1599–1605. [Google Scholar] [CrossRef] [PubMed]
- Eley, J.W.; Hill, H.A.; Chen, V.W.; Austin, D.F.; Wesley, M.N.; Muss, H.B.; Greenberg, R.S.; Coates, R.J.; Correa, P.; Redmond, C.K.; et al. Racial differences in survival from breast cancer: Results of the National Cancer Institute Black/White Cancer Survival Study. J. Natl. Cancer Inst. 1995, 87, 1686–1693. [Google Scholar] [CrossRef]
- Carey, L.A.; Perou, C.M.; Livasy, C.A.; Dressler, L.G.; Cowan, D.; Conway, K.; Karaca, G.; Troester, M.A.; Tse, C.K.; Edmiston, S.; et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA 2006, 295, 2492–2502. [Google Scholar] [CrossRef] [PubMed]
- Harlan, L.C.; Coates, R.J.; Block, G.; Greenberg, R.S.; Ershow, A.; Forman, M.; Heymsfield, S.D. Estrogen receptor status and dietary intakes in breast cancer patients. Epidemiology 1993, 4, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Van Ryn, M.; Burke, J. The effect of patient race and socio-economic status on physician perceptions of patients. Soc. Sci. Med. 2000, 50, 813–828. [Google Scholar] [CrossRef]
- Hair, B.Y.; Hayes, S.; Tse, C.K.; Bell, M.B.; Olshan, A.F. Racial differences in physical activity among breast cancer survivors: Implications for breast cancer care. Cancer 2014, 120, 2174–2182. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.L.; Owusu, C.; Nock, N.L.; Li, L.; Berger, N.A. Race, age, and obesity disparities in adult physical activity levels in breast cancer patients and controls. Front. Public Health 2014, 2, 150. [Google Scholar] [CrossRef] [PubMed]
- Stout, N.L.; Binkley, J.M.; Schmitz, K.H.; Andrews, K.; Hayes, S.C.; Campbell, K.L.; McNeely, M.L.; Soballe, P.W.; Berger, A.M.; Cheville, A.L.; et al. A prospective surveillance model for rehabilitation for women with breast cancer. Cancer 2012, 118, 2191–2200. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.H.; Hefand, S.L. New tricks of an old molecule: Lifespan regulation by p53. Aging Cell 2006, 5, 437–440. [Google Scholar] [CrossRef] [PubMed]
- Gasco, M.; Shami, S.; Crook, T. The p53 pathway in breast cancer. Breast Cancer Res. 2002, 4, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Morris, G.J.; Naidu, S.; Topham, A.K.; Guiles, F.; Xu, Y.; McCue, P.; Schwartz, G.F.; Park, P.K.; Rosenberg, A.L.; Brill, K.; et al. Differences in breast carcinoma characteristics in newly diagnosed African-American and Caucasian patients: A single-institution compilation compared with the National Cancer Institute’s Surveillance, Epidemiology, and End Results database. Cancer 2007, 110, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Donninger, H.; Vos, M.D.; Clark, G.J. The RASSF1A tumor suppressor. J. Cell Sci. 2007, 120, 3163–3172. [Google Scholar] [CrossRef] [PubMed]
- Krop, I.; Parker, M.T.; Bloushtain-Qimron, N.; Porter, D.; Gelman, R.; Sasaki, H.; Maurer, M.; Terry, M.B.; Parsons, R.; Polyak, K. HIN-1, an inhibitor of cell growth, invasion, and AKT activation. Cancer Res. 2005, 65, 9659–9669. [Google Scholar] [CrossRef] [PubMed]
- Lund, M.J.; Trivers, K.F.; Porter, P.L.; Coates, R.J.; Leyland-Jones, B.; Brawley, O.W.; Flagg, E.W.; O’Regan, R.M.; Gabram, S.G.; Eley, J.W. Race and triple negative threats to breast cancer survival: A population-based study in Atlanta, GA. Breast Cancer Res. Treat. 2009, 113, 357–370. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, N.H.; Arnerlov, C.; Emdin, S.O.; Landberg, G. Cyclin E overexpression, a negative prognostic factor in breast cancer with strong correlation to oestrogen receptor status. Br. J. Cancer 1996, 74, 874–880. [Google Scholar] [CrossRef] [PubMed]
- Morton, J.P.; Timpson, P.; Karim, S.A.; Ridgway, R.A.; Athineos, D.; Doyle, B.; Jamieson, N.B.; Oien, K.A.; Lowy, A.M.; Brunton, V.G.; et al. Mutant p53 drives metastasis and overcomes growth arrest/senescence in pancreatic cancer. Proc. Natl. Acad. Sci. USA 2010, 107, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Videira, M.; Reis, R.L.; Brito, M.A. Deconstructing breast cancer cell biology and the mechanisms of multidrug resistance. Biochim. Biophys. Acta 2014, 1846, 312–325. [Google Scholar] [CrossRef] [PubMed]
- Filipova, A.; Seifrtova, M.; Mokry, J.; Dvorak, J.; Rezacova, M.; Filip, S.; Diaz-Gracia, D. Breast cancer and cancer stem cells: A mini-review. Tumori 2014, 100, 363–369. [Google Scholar] [PubMed]
- Booy, E.P.; Henson, E.S.; Gibson, S.B. Epidermal growth factor regulates Mcl-1 expression through the MAPK-Elk-1 signalling pathway contributing to cell survival in breast cancer. Oncogene 2011, 30, 2367–2378. [Google Scholar] [CrossRef] [PubMed]
- Oakes, S.R.; Vaillant, F.; Lim, E.; Lee, L.; Breslin, K.; Feleppa, F.; Deb, S.; Ritchie, M.E.; Takano, E.; Ward, T.; et al. Sensitization of BCL-2-expressing breast tumors to chemotherapy by the BH3 mimetic ABT-737. Proc. Natl. Acad. Sci. USA 2012, 109, 2766–2771. [Google Scholar] [CrossRef] [PubMed]
- Elfadl, D.; Hodgkinson, V.C.; Long, E.D.; Scaife, L.; Drew, P.J.; Lind, M.J.; Cawkwell, L. A pilot study to investigate the role of the 26S proteasome in radiotherapy resistance and loco-regional recurrence following breast conserving therapy for early breast cancer. Breast 2011, 20, 334–337. [Google Scholar] [CrossRef] [PubMed]
- Panischeva, L.A.; Kakpakova, E.S.; Rybalkina, E.Y.; Stavrovskaya, A.A. Influence of proteasome inhibitor bortezomib on the expression of multidrug resistance genes and AKT kinase activity. Biochemistry 2011, 76, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, R.M.; Muqbil, I.; Lowe, L.; Yedjou, C.; Hsu, H.Y.; Lin, L.T.; Siegelin, M.D.; Fimognari, C.; Kumar, N.B.; Dou, Q.P.; et al. Broad targeting of resistance to apoptosis in cancer. Semin. Cancer Biol. 2015, 35, S78–S103. [Google Scholar] [CrossRef] [PubMed]
- Maskarinec, G.; Sen, C.; Koga, K.; Conroy, S.M. Ethnic differences in breast cancer survival: Status and determinants. Women’s Health 2011, 7, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Ooi, S.L.; Martinez, M.E.; Li, C.I. Disparities in breast cancer characteristics and outcomes by race/ethnicity. Breast Cancer Res. Treat. 2011, 127, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Tannenbaum, S.L.; KoruSengul, T.; Miao, F.; Byrne, M.M. Disparities in survival after female breast cancer diagnosis: A population based study. Cancer Causes Control 2013, 24, 1705–1715. [Google Scholar] [CrossRef] [PubMed]
- Wray, C.J.; Phatak, U.R.; Robinson, E.K.; Wiatek, R.L.; Rieber, A.G.; Gonzalez, A.; Ko, T.C.; Kao, L.S. The effect of age related breast cancer survival disparities. Ann. Surg. Oncol. 2013, 20, 2541–2547. [Google Scholar] [CrossRef] [PubMed]
- DeSantis, C.; Ma, J.; Bryan, L.; Jemal, A. Breast cancer statistics, 2013. CA Cancer J. Clin. 2014, 64, 52–62. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Male | Female | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Cancer | NH Black Rate a | NH White Rate a | Absolute Difference b | Rate Ratio c | Cancer | NH Black Rate a | NH White Rate a | Absolute Difference b | Rate Ratio c |
| Kaposi sarcoma | 1.7 | 0.5 | 1.2 | 3.57 d | Kaposi sarcoma | 0.2 | <0.1 | 0.1 | 3.96 d |
| Myeloma | 14.8 | 7.0 | 7.8 | 2.11 d | Myeloma | 11.1 | 4.3 | 6.8 | 2.58 d |
| Stomach | 15.1 | 7.8 | 7.3 | 1.93 d | Stomach | 8.0 | 3.5 | 4.5 | 2.30 d |
| Liver & IHB | 16.5 | 9.3 | 7.2 | 1.77 d | Liver & IHB | 4.8 | 3.2 | 1.6 | 1.52 d |
| Prostate | 208.7 | 123.0 | 85.7 | 1.70 d | Uterine cervix | 10.0 | 7.1 | 2.9 | 1.41 d |
| Larynx | 9.3 | 6.3 | 3.0 | 1.48 d | Pancreas | 14.4 | 10.6 | 3.8 | 1.36 d |
| Breast | 2.0 | 1.4 | 0.6 | 1.45 d | Esophagus | 2.5 | 1.8 | 0.7 | 1.34 d |
| Colon & rectum | 60.3 | 47.4 | 12.9 | 1.27 d | Colon & rectum | 44.1 | 36.2 | 7.9 | 1.22 d |
| Pancreas | 17.2 | 14.0 | 3.2 | 1.23 d | Kidney & renal pelvis | 13.0 | 11.3 | 1.7 | 1.15 d |
| Lung & bronchus | 93.4 | 79.3 | 14.1 | 1.18 d | Breast | 124.3 | 128.1 | −3.8 | 0.97 d |
| Kidney & renal pelvis | 24.2 | 21.8 | 2.4 | 1.11 d | Uterine corpus | 23.0 | 25.5 | −2.5 | 0.90 d |
| Hodgkin lymphoma | 3.2 | 3.4 | −0.2 | 0.95 d | Hodgkin lymphoma | 2.4 | 2.7 | −0.3 | 0.88 d |
| Esophagus | 8.0 | 8.8 | −0.8 | 0.90 d | Lung & bronchus | 51.4 | 58.7 | −7.3 | 0.87 d |
| Oral cavity & pharynx | 15.3 | 18.1 | −2.8 | 0.84 d | Leukemia | 8.6 | 10.7 | −2.1 | 0.80 d |
| Leukemia | 13.2 | 17.7 | −4.5 | 0.75 d | Oral cavity & pharynx | 5.2 | 6.7 | −1.5 | 0.78 d |
| Non-Hodgkin lymphoma | 17.2 | 24.1 | −6.9 | 0.71 d | Ovary | 9.6 | 12.4 | −2.8 | 0.77 d |
| Brain & ONS | 4.9 | 8.8 | −3.9 | 0.56 d | Non-Hodgkin lymphoma | 12.0 | 16.6 | −4.6 | 0.72 d |
| Urinary bladder | 19.8 | 40.2 | −20.4 | 0.49 d | Urinary bladder | 6.7 | 9.9 | −3.2 | 0.68 d |
| Thyroid | 3.7 | 7.7 | −4.0 | 0.48 d | Thyroid | 12.9 | 21.9 | −9.0 | 0.59 d |
| Testis | 1.4 | 6.8 | −5.4 | 0.21 d | Brain & ONS | 3.6 | 6.3 | −2.7 | 0.58 d |
| Melanoma of the skin | 1.1 | 31.3 | −30.2 | 0.04 d | Melanoma of the skin | 1.0 | 20.6 | −19.6 | 0.05 d |
| All sites | 592.3 | 528.9 | 63.4 | 1.12 d | All sites | 408.1 | 436.2 | −28.1 | 0.94 d |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yedjou, C.G.; Tchounwou, P.B.; Payton, M.; Miele, L.; Fonseca, D.D.; Lowe, L.; Alo, R.A. Assessing the Racial and Ethnic Disparities in Breast Cancer Mortality in the United States. Int. J. Environ. Res. Public Health 2017, 14, 486. https://doi.org/10.3390/ijerph14050486
Yedjou CG, Tchounwou PB, Payton M, Miele L, Fonseca DD, Lowe L, Alo RA. Assessing the Racial and Ethnic Disparities in Breast Cancer Mortality in the United States. International Journal of Environmental Research and Public Health. 2017; 14(5):486. https://doi.org/10.3390/ijerph14050486
Chicago/Turabian StyleYedjou, Clement G., Paul B. Tchounwou, Marinelle Payton, Lucio Miele, Duber D. Fonseca, Leroy Lowe, and Richard A. Alo. 2017. "Assessing the Racial and Ethnic Disparities in Breast Cancer Mortality in the United States" International Journal of Environmental Research and Public Health 14, no. 5: 486. https://doi.org/10.3390/ijerph14050486
APA StyleYedjou, C. G., Tchounwou, P. B., Payton, M., Miele, L., Fonseca, D. D., Lowe, L., & Alo, R. A. (2017). Assessing the Racial and Ethnic Disparities in Breast Cancer Mortality in the United States. International Journal of Environmental Research and Public Health, 14(5), 486. https://doi.org/10.3390/ijerph14050486