
Birth Outcomes after the Fukushima Daiichi Nuclear Power Plant Disaster: A Long-Term Retrospective Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Participants
2.2. Data Collection
2.3. Main Outcome Measures
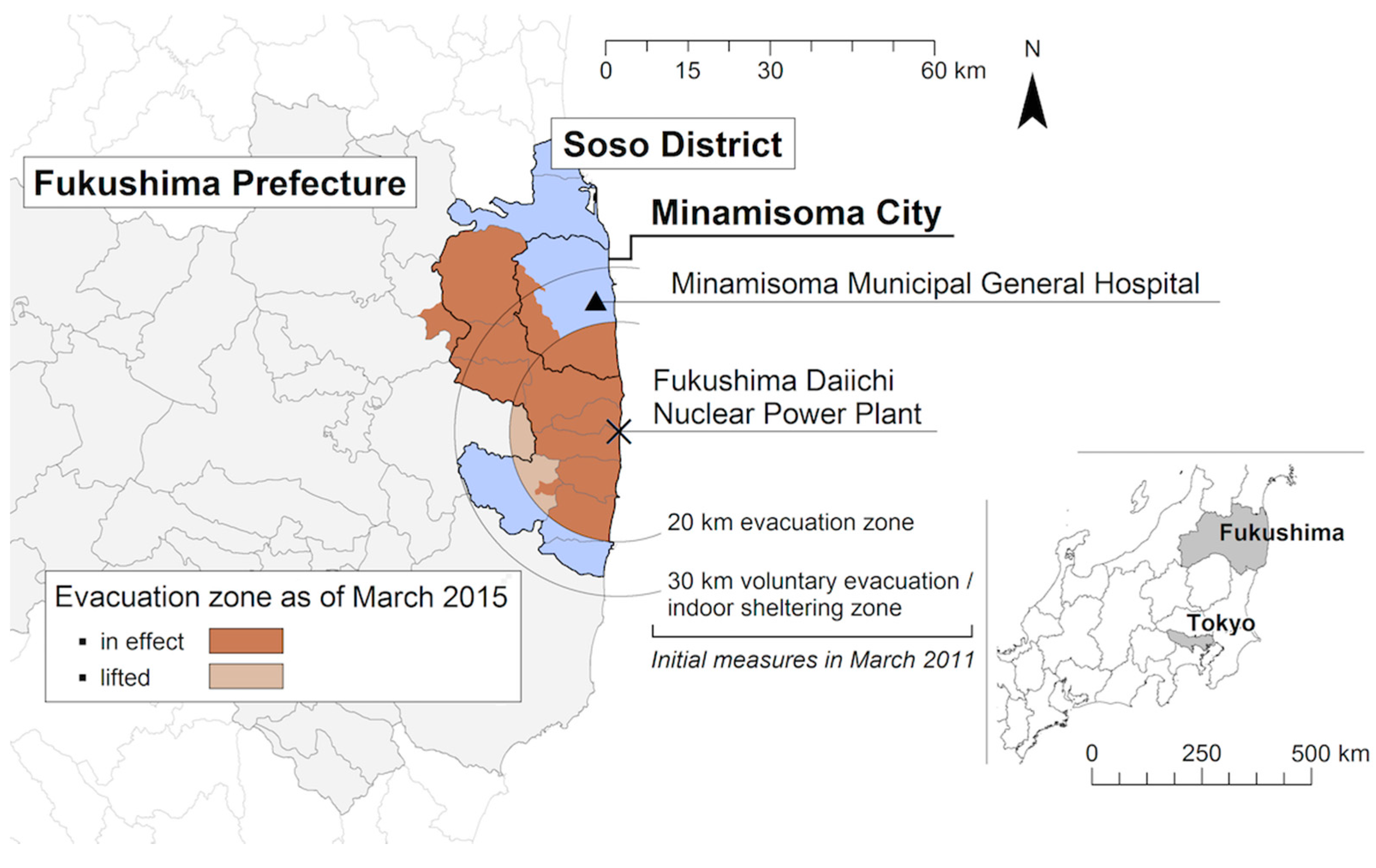
2.4. Residential Area at the Time of the Disaster
2.5. Post-Disaster Food Purchasing Patterns
2.6. Statistical Analyses
2.7. Ethics Approval
3. Results
3.1. Characteristics of Study Participants
3.2. Risk Ratios of Low Birthweight Birth and Preterm Birth
3.3. Regression Analysis
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Availability of Data and Material
References
- Saigal, S.; Doyle, L.W. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet 2008, 371, 261–269. [Google Scholar] [CrossRef]
- McCormick, M.C. The contribution of low birth weight to infant mortality and childhood morbidity. N Engl. J. Med. 1985, 312, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, K.M.; Barker, D.J. Fetal programming and adult health. Public Health Nutr. 2001, 4, 611–624. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, P.D.; Hanson, M.A.; Cooper, C.; Thornburg, K.L. Effect of in utero and early-life conditions on adult health and disease. N. Engl. J. Med. 2008, 359, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Valero De Bernabe, J.; Soriano, T.; Albaladejo, R.; Juarranz, M.; Calle, M.E.; Martinez, D.; Dominguez-Rojas, V. Risk factors for low birth weight: A review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 116, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Kim, D.; Saada, A. The social determinants of infant mortality and birth outcomes in Western developed nations: A cross-country systematic review. Int. J. Environ. Res. Public Health 2013, 10, 2296–2335. [Google Scholar] [CrossRef] [PubMed]
- Steegers, E.A.; Barker, M.E.; Steegers-Theunissen, R.P.; Williams, M.A. Societal Valorisation of New Knowledge to Improve Perinatal Health: Time to Act. Paediatr. Perinat. Epidemiol. 2016, 30, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Harville, E.; Xiong, X.; Buekens, P. Disasters and perinatal health: A systematic review. Obstet. Gynecol. Surv. 2010, 65, 713–728. [Google Scholar] [CrossRef] [PubMed]
- Tong, V.T.; Zotti, M.E.; Hsia, J. Impact of the Red River catastrophic flood on women giving birth in North Dakota, 1994–2000. Matern. Child Health J. 2011, 15, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.; Harville, E.W.; Mattison, D.R.; Elkind-Hirsch, K.; Pridjian, G.; Buekens, P. Exposure to Hurricane Katrina, post-traumatic stress disorder and birth outcomes. Am. J. Med. Sci. 2008, 336, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Torche, F. The effect of maternal stress on birth outcomes: Exploiting a natural experiment. Demography 2011, 48, 1473–1491. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.E.; Li, H.J.; Zhang, X.G.; Zhang, H.; Han, P.Y.; An, Q.; Ding, W.J.; Wang, M.Q. The impact of the Wenchuan earthquake on birth outcomes. PLoS ONE 2009, 4, e8200. [Google Scholar] [CrossRef] [PubMed]
- Sanguanklin, N.; McFarlin, B.L.; Park, C.G.; Giurgescu, C.; Finnegan, L.; White-Traut, R.; Engstrom, J.L. Effects of the 2011 flood in Thailand on birth outcomes and perceived social support. J. Obstet. Gynecol. Neonatal. Nurs. 2014, 43, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Harville, E.W.; Tran, T.; Xiong, X.; Buekens, P. Population changes, racial/ethnic disparities, and birth outcomes in Louisiana after Hurricane Katrina. Disaster Med. Public Health Prep. 2010, 4, S39–S45. [Google Scholar] [CrossRef] [PubMed]
- Harville, E.W.; Do, M. Reproductive and Birth Outcomes in Haiti before and after the 2010 Earthquake. Disaster Med. Public Health Prep. 2016, 10, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Harville, E.W.; Giarratano, G.; Savage, J.; Barcelona de Mendoza, V.; Zotkiewicz, T. Birth Outcomes in a Disaster Recovery Environment: New Orleans Women After Katrina. Matern. Child Health J. 2015, 19, 2512–2522. [Google Scholar] [CrossRef] [PubMed]
- Ohlsson, A.; Shah, P.S. Knowledge Synthesis Group of Determinants of Preterm/LBWb. Effects of the 11 September 2001 disaster on pregnancy outcomes: A systematic review. Acta Obstet. Gynecol. Scand. 2011, 90, 6–18. [Google Scholar] [CrossRef] [PubMed]
- Eskenazi, B.; Marks, A.R.; Catalano, R.; Bruckner, T.; Toniolo, P.G. Low birthweight in New York City and upstate New York following the events of 11 September. Hum. Reprod 2007, 22, 3013–3020. [Google Scholar] [CrossRef] [PubMed]
- Oyarzo, C.; Bertoglia, P.; Avendano, R.; Bacigalupo, F.; Escudero, A.; Acurio, J.; Escudero, C. Adverse perinatal outcomes after the 27 February 2010 Chilean earthquake. J. Matern Fetal Neonatal Med. 2012, 25, 1868–1873. [Google Scholar] [CrossRef] [PubMed]
- Zotti, M.E.; Williams, A.M.; Robertson, M.; Horney, J.; Hsia, J. Post-disaster reproductive health outcomes. Matern. Child Health J. 2013, 17, 783–796. [Google Scholar] [CrossRef] [PubMed]
- Maslow, C.B.; Caramanica, K.; Li, J.; Stellman, S.D.; Brackbill, R.M. Reproductive Outcomes Following Maternal Exposure to the Events of 11 September 2001, at the World Trade Center, in New York City. Am. J. Public Health 2016, 106, 1796–1803. [Google Scholar] [CrossRef] [PubMed]
- Witt, W.P.; Cheng, E.R.; Wisk, L.E.; Litzelman, K.; Chatterjee, D.; Mandell, K.; Wakeel, F. Maternal stressful life events prior to conception and the impact on infant birth weight in the United States. Am. J. Public Health 2014, 104, S81–S89. [Google Scholar] [CrossRef] [PubMed]
- Cheng, E.R.; Park, H.; Wisk, L.E.; Mandell, K.C.; Wakeel, F.; Litzelman, K.; Chatterjee, D.; Witt, W.P. Examining the link between women’s exposure to stressful life events prior to conception and infant and toddler health: The role of birth weight. J. Epidemiol. Community Health 2016, 70, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, A.; Tanigawa, K.; Ohtsuru, A.; Yabe, H.; Maeda, M.; Shigemura, J.; Ohira, T.; Tominaga, T.; Akashi, M.; Hirohashi, N.; et al. Health effects of radiation and other health problems in the aftermath of nuclear accidents, with an emphasis on Fukushima. Lancet 2015, 386, 479–488. [Google Scholar] [CrossRef]
- Nomura, S.; Blangiardo, M.; Tsubokura, M.; Ozaki, A.; Morita, T.; Hodgson, S. Postnuclear disaster evacuation and chronic health in adults in Fukushima, Japan: A long-term retrospective analysis. BMJ Open 2016, 6, e010080. [Google Scholar] [CrossRef] [PubMed]
- Gilmour, S.; Sugimoto, A.; Nomura, S.; Oikawa, T. Long-Term Changes in Stroke-Related Hospital Admissions After the Fukushima Triple Disaster. J. Am. Geriatr. Soc. 2015, 63, 2425–2426. [Google Scholar] [CrossRef] [PubMed]
- Tsubokura, M.; Hara, K.; Matsumura, T.; Sugimoto, A.; Nomura, S.; Hinata, M.; Shibuya, K.; Kami, M. The immediate physical and mental health crisis in residents proximal to the evacuation zone after Japan’s nuclear disaster: An observational pilot study. Disaster Med. Public Health Prep. 2014, 8, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Yamagata, Z.; Kawado, M.; Hashimoto, S. Effects of the Great East Japan Earthquake on Secondary Sex Ratio and Perinatal Outcomes. J. Epidemiol. 2016, 26, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Fujimori, K.; Kyozuka, H.; Yasuda, S.; Goto, A.; Yasumura, S.; Ota, M.; Ohtsuru, A.; Nomura, Y.; Hata, K.; Suzuki, K.; et al. Pregnancy and birth survey after the Great East Japan Earthquake and Fukushima Daiichi Nuclear Power Plant accident in Fukushima prefecture. Fukushima J. Med. Sci. 2014, 60, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, S.; Kyozuka, H.; Nomura, Y.; Fujimori, K.; Goto, A.; Yasumura, S.; Hata, K.; Ohira, T.; Abe, M. Influence of the Great East Japan Earthquake and the Fukushima Daiichi Nuclear Disaster on the Birth Weight of Newborns in Fukushima Prefecture: Fukushima Health Management Survey. J. Matern Fetal Neonatal Med. 2016, 9, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Ishii, K.; Goto, A.; Ota, M.; Yasumura, S.; Fujimori, K. Pregnancy and Birth Survey of the Fukushima Health Management Survey. Asia Pac. J. Public Health 2017, 29, 56S–62S. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Fujimori, K.; Yasumura, S.; Goto, A.; Nakai, A. Obstetric Outcomes in Women in Fukushima Prefecture during and after the Great East Japan Earthquake and Fukushima Nuclear Power Plant Accident: The Fukushima Health Management Survey. Open J. Obstet. Gynecol. 2016, 6, 705–713. [Google Scholar] [CrossRef]
- The National Diet of Japan. The National Diet of Japan Fukushima Nuclear Accident Independent Investigation Commission: Overview of the Damage and How It Spread; Executive Summary; The National Diet of Japan: Tokyo, Japan, 2012. [Google Scholar]
- Ministry of Education Culture Sports Science and Technology (MEXT): Document 1: Outlook of Evacuation in Fukushima Prefecture, 14th Meeting of the Examining Committee for Nuclear Power Restitution Disputes. Available online: http://www.mext.go.jp/b_menu/shingi/chousa/kaihatu/016/shiryo/1311103.htm (accessed on 8 November 2016).
- Little, J. The Chernobyl accident, congenital anomalies and other reproductive outcomes. Paediatr. Perinat. Epidemiol. 1993, 7, 121–151. [Google Scholar] [CrossRef] [PubMed]
- Dolk, H.; Nichols, R. Evaluation of the impact of Chernobyl on the prevalence of congenital anomalies in 16 regions of Europe. EUROCAT Working Group. Int. J. Epidemiol. 1999, 28, 941–948. [Google Scholar] [CrossRef] [PubMed]
- United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR). Developments since the 2013 UNSCEAR Report on the Levels and Effects of Radiation Exposure due to the Nuclear Accident Following the Great East-Japan Earthquake and Tsunami: A 2015 White Paper to Guide the Scientific Committee’s Future Programme of Work; United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR): New York, NY, USA, 2015. [Google Scholar]
- Levi, R.; Lundberg, U.; Hanson, U.; Frankenhacuser, M. Anxiety during pregnancy after the Chernobyl accident as related to obstetric outcome. J. Psychosom. Obstet. Gynecol. 1989, 10, 221–230. [Google Scholar] [CrossRef]
- Dancause, K.N.; Laplante, D.P.; Oremus, C.; Fraser, S.; Brunet, A.; King, S. Disaster-related prenatal maternal stress influences birth outcomes: Project Ice Storm. Early Hum. Dev. 2011, 87, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, B.E.; Sutton, P.D.; Mathews, T.J.; Martin, J.A.; Ventura, S.J. The effect of Hurricane Katrina: Births in the U.S. Gulf Coast region, before and after the storm. Natl. Vital Stat. Rep. 2009, 58, 1–28. [Google Scholar] [PubMed]
- Hasegawa, R. Disaster Evacuation from Japan’s 2011 Tsunami Disaster and the Fukushima Nuclear Accident. Available online: https://orbi.ulg.ac.be/bitstream/2268/195804/1/STUDY0513_RH_DEVAST report-1.pdf (accessed on 15 April 2017).
- Minamisoma City Office: Evacuation Status of Minamisoma City. Available online: https://www.city.minamisoma.lg.jp/index.cfm/10,853,58,html (accessed on 26 March 2017).
- Zhang, H.; Yan, W.; Oba, A.; Zhang, W. Radiation-driven migration: The case of Minamisoma City, Fukushima, Japan, after the Fukushima nuclear accident. Int J. Environ. Res. Public Health 2014, 11, 9286–9305. [Google Scholar] [CrossRef] [PubMed]
- Samuels, J. 3.11: Disaster and Change in Japan; Cornell University Press: Ithaca, NY, USA, 2013. [Google Scholar]
- Tateno, S.; Yokoyama, H.M. Public anxiety, trust, and the role of mediators in communicating risk of exposure to low dose radiation after the Fukushima Daiichi Nuclear Plant explosion. J. Sci. Commun. 2013, 12, 1–22. [Google Scholar]
- Goto, A.; Bromet, E.J.; Fujimori, K. Pregnancy, Birth Survey Group of Fukushima Health Management S: Immediate effects of the Fukushima nuclear power plant disaster on depressive symptoms among mothers with infants: A prefectural-wide cross-sectional study from the Fukushima Health Management Survey. BMC Psychiatry 2015, 15, 59. [Google Scholar]
- Muramatsu, N.; Akiyama, H. Japan: Super-aging society preparing for the future. Gerontologist 2011, 51, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Van Aalst, M.K. The impacts of climate change on the risk of natural disasters. Disasters 2006, 30, 5–18. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | 2008 | 2009 | 2010 | 2012 | 2013 | 2014 | p-Value for Percentage Difference * |
|---|---|---|---|---|---|---|---|
| Low Birthweight | 0.67 | ||||||
| No | 217 (92.0) | 203 (91.9) | 202 (94.4) | 85 (94.4) | 152 (93.8) | 161 (90.5) | |
| Yes | 19 (8.1) | 18 (8.1) | 12 (5.6) | 5 (5.6) | 10 (6.2) | 17 (9.6) | |
| Preterm Birth | 0.51 | ||||||
| No | 223 (94.5) | 212 (95.9) | 201 (93.9) | 88 (97.8) | 153 (94.4) | 173 (97.2) | |
| Yes | 13 (5.5) | 9 (4.1) | 13 (6.1) | 2 (2.2) | 9 (5.6) | 5 (2.8) | |
| Sex of Neonate | 0.37 | ||||||
| Male | 120 (51.3) | 104 (47.7) | 119 (56.1) | 40 (44.9) | 77 (47.8) | 94 (53.1) | |
| Female | 114 (48.7) | 114 (52.3) | 93 (43.9) | 49 (55.1) | 84 (52.2) | 83 (46.9) | |
| Mode of Delivery | 0.26 | ||||||
| Vaginal delivery | 183 (77.5) | 179 (81.0) | 158 (73.8) | 75 (83.3) | 123 (75.9) | 131 (73.6) | |
| Caesarean section | 53 (22.5) | 42 (19.0) | 56 (26.2) | 15 (16.7) | 39 (24.1) | 47 (26.4) | |
| Maternal Age (year) | <0.05 | ||||||
| –35] | 201 (85.2) | 181 (81.9) | 183 (85.5) | 67 (74.4) | 122 (75.3) | 143 (79.2) | |
| (35– | 35 (14.8) | 40 (18.1) | 31 (14.5) | 23 (25.6) | 40 (24.7) | 37 (20.8) | |
| Number of Previous Deliveries | <0.001 | ||||||
| 0 | 44 (18.6) | 94 (42.5) | 90 (42.1) | 34 (37.8) | 74 (45.7) | 97 (54.5) | |
| 1 | 31 (13.1) | 86 (38.9) | 88 (41.1) | 39 (43.3) | 59 (36.4) | 52 (29.2) | |
| 2 or more | 161 (68.2) | 41 (18.6) | 36 (16.8) | 17 (18.9) | 29 (17.9) | 29 (16.3) | |
| Residential Area † | <0.001 | ||||||
| Inside the mandatory evacuation zone | 84 (35.6) | 92 (41.6) | 79 (36.9) | 11 (12.2) | 16 (9.9) | 26 (14.6) | |
| Inside the sheltering/voluntary evacuation zone | 44 (18.6) | 39 (17.7) | 40 (18.7) | 28 (31.1) | 78 (48.2) | 79 (44.4) | |
| Inside areas of Soso District under no evacuation orders | 32 (13.6) | 28 (12.7) | 23 (10.8) | 32 (35.6) | 53 (32.7) | 48 (27.0) | |
| Outside Soso District | 76 (32.2) | 62 (28.1) | 72 (33.6) | 19 (21.1) | 15 (9.3) | 25 (14.0) | |
| Season of Delivery | 0.25 | ||||||
| Spring | 57 (24.2) | 66 (29.9) | 57 (26.6) | 15 (16.7) | 36 (22.2) | 52 (29.2) | |
| Summer | 59 (25.0) | 55 (24.9) | 58 (27.1) | 18 (20.0) | 39 (24.1) | 43 (24.2) | |
| Autumn | 60 (25.4) | 45 (20.4) | 52 (24.3) | 26 (28.9) | 40 (24.7) | 42 (23.6) | |
| Winter | 60 (25.4) | 55 (24.9) | 47 (22.0) | 31 (34.4) | 47 (29.0) | 41 (23.0) | |
| Birth Outcome | Risk Ratio | 95% CI | p-Value |
|---|---|---|---|
| Low Birthweight | |||
| 2012 | 0.71 | 0.29–1.75 | 0.46 |
| 2013 | 0.80 | 0.42–1.55 | 0.52 |
| 2014 | 1.28 | 0.76–2.17 | 0.35 |
| Preterm Birth | |||
| 2012 | 0.40 | 0.10–1.64 | 0.20 |
| 2013 | 1.01 | 0.49–2.05 | 0.99 |
| 2014 | 0.52 | 0.21–1.30 | 0.16 |
| Variable | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| Year | |||
| 2012 | reference | ||
| 2013 | 0.83 | 0.15–4.41 | 0.82 |
| 2014 | 1.69 | 0.38–7.63 | 0.44 |
| Sex of Neonate | |||
| Male | reference | ||
| Female | 3.15 | 0.77–12.87 | 0.11 |
| Mode of Delivery | |||
| Vaginal delivery | reference | ||
| Caesarean section | 4.27 | 0.81–22.47 | 0.09 |
| Maternal Age (year) | |||
| –35] | reference | ||
| (35– | 1.06 | 0.28–4.01 | 0.93 |
| Number of Previous Deliveries | |||
| 0 | reference | ||
| 1 | 0.73 | 0.20–2.57 | 0.62 |
| More than 2 | 0.56 | 0.10–3.08 | 0.51 |
| Residential Area | |||
| Inside the mandatory evacuation zone | 0.91 | 0.11–7.17 | 0.93 |
| Inside the sheltering/voluntary evacuation zone | 1.00 | 0.19–5.31 | 1.00 |
| Inside areas of Soso District under no evacuation orders | 0.54 | 0.08–3.60 | 0.52 |
| Outside Soso District | reference |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leppold, C.; Nomura, S.; Sawano, T.; Ozaki, A.; Tsubokura, M.; Hill, S.; Kanazawa, Y.; Anbe, H. Birth Outcomes after the Fukushima Daiichi Nuclear Power Plant Disaster: A Long-Term Retrospective Study. Int. J. Environ. Res. Public Health 2017, 14, 542. https://doi.org/10.3390/ijerph14050542
Leppold C, Nomura S, Sawano T, Ozaki A, Tsubokura M, Hill S, Kanazawa Y, Anbe H. Birth Outcomes after the Fukushima Daiichi Nuclear Power Plant Disaster: A Long-Term Retrospective Study. International Journal of Environmental Research and Public Health. 2017; 14(5):542. https://doi.org/10.3390/ijerph14050542
Chicago/Turabian StyleLeppold, Claire, Shuhei Nomura, Toyoaki Sawano, Akihiko Ozaki, Masaharu Tsubokura, Sarah Hill, Yukio Kanazawa, and Hiroshi Anbe. 2017. "Birth Outcomes after the Fukushima Daiichi Nuclear Power Plant Disaster: A Long-Term Retrospective Study" International Journal of Environmental Research and Public Health 14, no. 5: 542. https://doi.org/10.3390/ijerph14050542
APA StyleLeppold, C., Nomura, S., Sawano, T., Ozaki, A., Tsubokura, M., Hill, S., Kanazawa, Y., & Anbe, H. (2017). Birth Outcomes after the Fukushima Daiichi Nuclear Power Plant Disaster: A Long-Term Retrospective Study. International Journal of Environmental Research and Public Health, 14(5), 542. https://doi.org/10.3390/ijerph14050542