The Effects of an Urban Forest Health Intervention Program on Physical Activity, Substance Abuse, Psychosomatic Symptoms, and Life Satisfaction among Adolescents


Abstract
:1. Introduction
1.1. Urban Forests and Parks as Potential Spaces for Health Promotion
1.2. The Urban Forest Health Intervention Program for Encouraging an Active and Healthy Lifestyle
2. Materials and Methods
2.1. Study Setting and Description of UFHIP
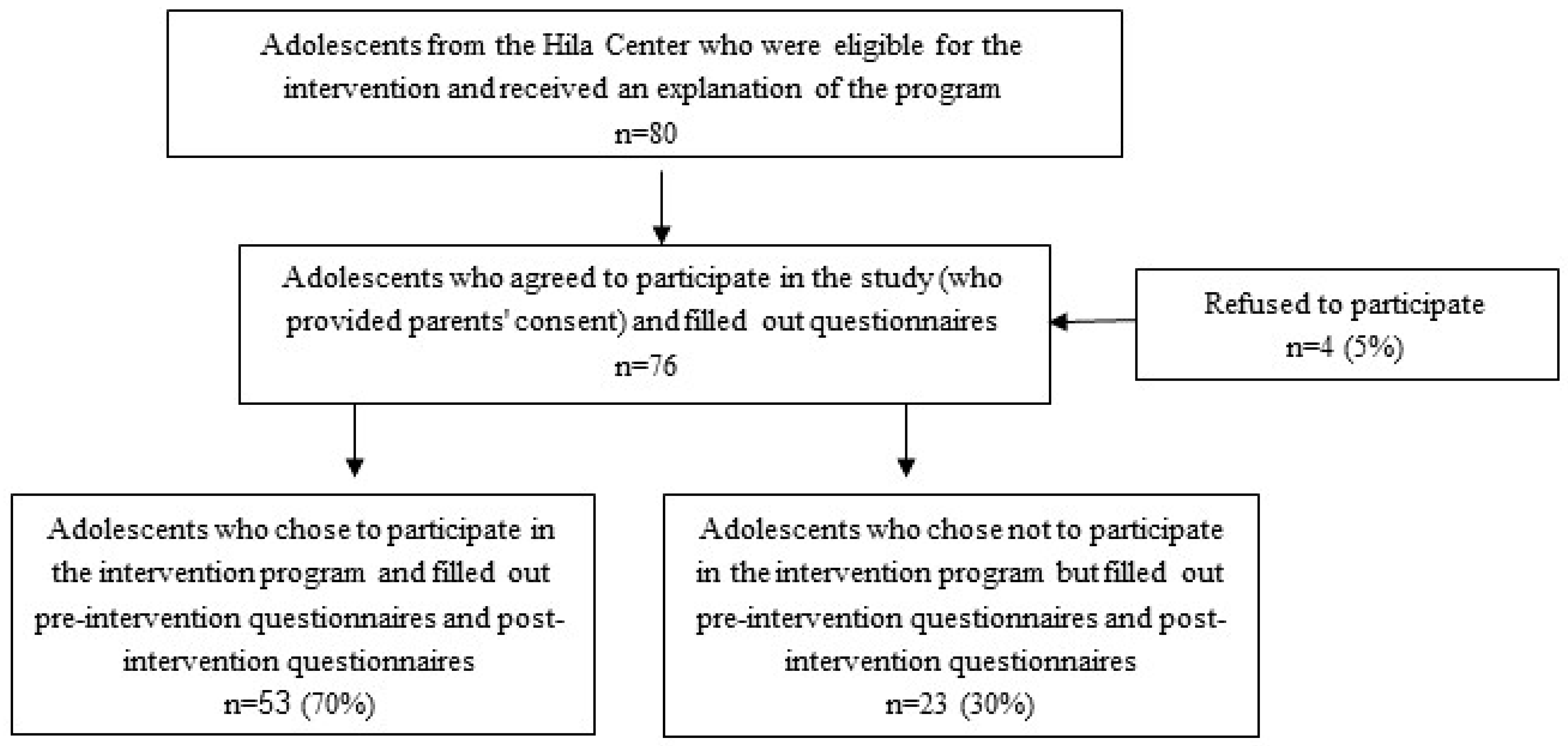
2.2. Research Design
2.3. Data Collection and Survey Instrument
Survey Content
2.4. Measures and Instruments
2.4.1. Physical Activity in the Urban Forest
2.4.2. Substance Use: Cigarette Smoking
2.4.3. Substance Use: Alcohol Consumption
2.4.4. Psychosomatic Symptoms
2.4.5. Life Satisfaction
2.5. Data Analyses
2.6. Ethical Approval
3. Results
Survey Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Grant, K.; Compas, B.E.; Thurm, A.E.; McMahon, S.D.; Gipson, P.Y. Stressors and child and adolescent psychopathology: Measurement issues and prospective effects. J. Clin. Child Adolesc. 2004, 33, 412–425. [Google Scholar] [CrossRef] [PubMed]
- Furstenberg, F.F., Jr.; Hughes, M.E. Social capital and successful development among at-risk youth. J. Marriage Fam. 1995, 580–592. [Google Scholar] [CrossRef]
- Bonny, A.E.; Britto, M.T.; Klostermann, B.K.; Hornung, R.W.; Slap, G.B. School disconnectedness: Identifying adolescents at risk. Pediatrics 2000, 106, 1017–1021. [Google Scholar] [CrossRef] [PubMed]
- Riele, K.T. Youth ‘at risk’: Further marginalizing the marginalized? J. Educ. Policy 2006, 21, 129–145. [Google Scholar] [CrossRef]
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearce, M.; Page, A.S.; Griffin, T.P.; Cooper, A.R. Who children spend time with after school: Associations with objectively recorded indoor and outdoor physical activity. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 45. [Google Scholar] [CrossRef] [PubMed]
- Glapa, A.; Grzesiak, J.; Laudanska-Krzeminska, I.; Chin, M.-K.; Edginton, C.R.; Mok, M.M.C.; Bronikowski, M. The Impact of Brain Breaks Classroom-Based Physical Activities on Attitudes toward Physical Activity in Polish School Children in Third to Fifth Grade. Int. J. Environ. Res. Public Health 2018, 15, 368. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.J.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors? A systematic review. Environ. Sci. Technol. 2011, 45, 761–772. [Google Scholar] [CrossRef] [PubMed]
- Gladwell, V.F.; Brown, D.K.; Wood, C.; Sandercock, G.R.; Barton, J.L. The great outdoors: How a green exercise environment can benefit all. Extreme Physiol. Med. 2013, 2, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christiana, R.W.; Battista, R.A.; James, J.J.; Bergman, S.M. Pediatrician prescriptions for outdoor physical activity among children: A pilot study. Prev. Med. Rep. 2017, 5, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Romar, J.E.; Enqvist, I.; Kulmala, J.; Kallio, J.; Tammelin, T. Physical activity and sedentary behaviour during outdoor learning and traditional indoor school days among Finnish primary school students. J. Adventure Educ. Outdoor Learn. 2018, 24. [Google Scholar] [CrossRef]
- Growing Up Unequal: Gender and Socioeconomic Differences in Young People’s Health and Well-Being. Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2013/2014 Survey. Available online: http://www.euro.who.int/en/publications/abstracts/growing-up-unequal.-hbsc-2016-study-20132014-survey (accessed on 6 June 2017).
- Alcohol Use among Children and Youth. The Knesset Center for Research and Information: 2010. Available online: https://www.knesset.gov.il/mmm/data/pdf/ m02406.pdf (accessed on 6 June 2017). (In Hebrew)
- Hingson, R.W.; Zha, W. Binge Drinking Above and Below Twice the Adolescent Thresholds and Health-Risk Behaviors. Alcohol. Clin. Exp. Res. 2018, 42, 904–913. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Betts, N.M.; Hampl, J.S. Clustering of lifestyle behaviors: The relationship between cigarette smoking, alcohol consumption, and dietary intake. Am. J. Health Promot. 2000, 2, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance System; U.S. Department of Health and Human Services: Atlanta, GA, USA, 2015. Available online: https://www.cdc.gov/healthyyouth/data/yrbs/index.htm (accessed on 26 March 2018).
- Beard, E.; West, R.; Michie, S.; Brown, J. Association between smoking and alcohol-related behaviours: A time–series analysis of population trends in England. Addiction 2017, 112, 1832–1841. [Google Scholar] [CrossRef] [PubMed]
- Grevenstein, D.; Nagy, E.; Kroeninger-Jungaberle, H. Development of risk perception and substance use of tobacco, alcohol and cannabis among adolescents and emerging adults: Evidence of directional influences. Subst. Use Misuse 2015, 50, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Hertz, M.F.; Everett Jones, S.; Barrios, L.; David-Ferdon, C.; Holt, M. Association between bullying victimization and health risk behaviors among high school students in the United States. J. Sch. Health 2015, 85, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Solmi, M.; Veronese, N.; Sergi, G.; Luchini, C.; Favaro, A.; Santonastaso, P.; Vancampfort, D.; Correll, C.U.; Ussher, M.; Thapa-Chhetri, N.; et al. The association between smoking prevalence and eating disorders: A systematic review and meta-analysis. Addiction 2016, 111, 1914–1922. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.E.; Norman, R.E.; Suetani, S.; Thomas, H.J.; Sly, P.D.; Scott, J.G. Consequences of bullying victimization in childhood and adolescence: A systematic review and meta-analysis. World J. Psychiatry 2017, 7, 60–76. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Zhang, D.; Wang, J. A meta-analysis of the trait resilience and mental health. Personal. Individ. Differ. 2015, 76, 18–27. [Google Scholar] [CrossRef]
- Sallis, J.F.; Owen, N.; Fisher, E. Ecological models of health behavior. Health Behav. Theory Res. Pract. 2015, 5, 43–64. [Google Scholar]
- Gifford, R.; Nilsson, A. Personal and social factors that influence pro-environmental concern and behaviour: A review. Int. J. Psychol. 2014, 49, 141–157. [Google Scholar] [CrossRef] [PubMed]
- Park, N. The role of subjective well-being in positive youth development. Ann. Am. Acad. Polit. Soc. Sci. 2004, 591, 25–39. [Google Scholar] [CrossRef]
- Bluth, K.; Campo, R.A.; Futch, W.S.; Gaylord, S.A. Age and gender differences in the associations of self-compassion and emotional well-being in a large adolescent sample. J. Youth Adolesc. 2017, 46, 840–853. [Google Scholar] [CrossRef] [PubMed]
- Ronen, T.; Hamama, L.; Rosenbaum, M.; Mishely-Yarlap, A. Subjective well-being in adolescence: The role of self-control, social support, age, gender, and familial crisis. J. Happiness Stud. 2016, 17, 81–104. [Google Scholar] [CrossRef]
- Largo, W.E.; Guardino, C.; Wludyka, P.S.; Hall, K.W.; Wight, J.T.; Merten, J.W. Nature contact at school: The impact of an outdoor classroom on children’s well-being. Int. J. Environ. Health Res. 2018, 1–14. [Google Scholar] [CrossRef]
- Pretty, J.; Rogerson, M.; Barton, J. Green mind theory: How brain-body-behaviour links into natural and social environments for healthy habits. Int. J. Environ. Res. Public Health 2017, 14, 706. [Google Scholar] [CrossRef] [PubMed]
- Cason, D.R.; Gillis, H.L. A meta-analysis of outdoor adventure programming with adolescents. J. Exp. Educ. 1994, 17, 40–47. [Google Scholar] [CrossRef]
- Proctor, C.; Linley, P.A.; Maltby, J. Very Happy Youths: Benefits of Very High Life Satisfaction among Adolescents. Soc. Indic. Res. 2010, 98, 519–532. [Google Scholar] [CrossRef]
- Kondo, M.C.; Fluehr, J.M.; McKeon, T.; Branas, C.C. Urban green space and its impact on human health. Int. J. Environ. Res. Public Health 2018, 15, 445. [Google Scholar] [CrossRef] [PubMed]
- Chawla, L. Benefits of Nature Contact for Children. J. Plan. Lit. 2015, 30, 433–452. [Google Scholar] [CrossRef]
- Haluza, D.; Schönbauer, R.; Cervinka, R. Green perspectives for public health: A narrative review on the physiological effects of experiencing outdoor nature. Int. J. Environ. Res. Public Health 2014, 11, 5445–5461. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.C.K.; Maheswaran, R. The health benefits of urban green spaces: A review of the evidence. J. Public Health 2011, 33, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.K.; Barton, J.L.; Pretty, J.; Gladwell, V.F. Walks4Work: Assessing the role of the natural environment in a workplace physical activity intervention. Scand. J. Work Environ. Health 2014, 40, 390–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lachowycz, K.; Jones, A.P.; Page, A.S.; Wheeler, B.W.; Cooper, A.R. What can global positioning systems tell us about the contribution of different types of urban greenspace to children’s physical activity? Health Place 2012, 18, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Younan, D.; Tuvblad, C.; Li, L.; Wu, J.; Lurmann, F.; Franklin, M.; Berhane, K.; McConnell, R.; Wu, A.H.; Baker, L.A. Environmental determinants of aggression in adolescents: Role of urban neighborhood greenspace. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 591–601. [Google Scholar] [CrossRef]
- Brooks, A.M.; Ottley, K.M.; Arbuthnott, K.D.; Sevigny, P. Nature-related mood effects: Season and type of nature contact. J. Environ. Psychol. 2017, 54, 91–102. [Google Scholar] [CrossRef]
- Buchner, D.; Gobster, P. Promoting Active Visits to Parks: Models and Strategies for Transdisciplinary Collaboration. J. Phys. Act. Health 2017, 4, 36–49. [Google Scholar] [CrossRef]
- Harel-Fisch, Y.; Habib, J.; Walsh, S.D.; Boniel-Nissim, M.; Djalowski, A.; Amit, S.; Tesler, R.; Mishal, R. Youth in Israel: Health, Psychological and Social Well-Being and Patterns of Risk Behavior; Results from the 6th National Survey, Trend Analysis 1994–2011 and International Comparison; The International Research Program on Health and Well-Being of Young People; School of Education, Bar Ilan University: Ramat Gan, Israel, 2013. [Google Scholar]
- Israel Central Bureau of Statistics. Population at End of May 2018. Available online: http://www.cbs.gov.il (accessed on 3 July 2018).
- Currie, C.; Inchley, J.; Molcho, M.; Lenzi, M.; Veselska, Z.; Wild, F. Health Behavior in School-Aged Children; HBSC Study Protocol: Background, Methodology and Mandatory Items for the 2013/14 Survey; CAHRU: St Andrews, UK, 2014; Available online: http://www.hbsc.org (accessed on 1 June 2018).
- Bobakova, D.; Hamrik, Z.; Badura, P.; Sigmundova, D.; Nalecz, H.; Kalman, M. Test-retest reliability of selected physical activity and sedentary behavior HBSC items in the Czech Republic, Slovakia and Poland. Int. J. Public Health 2015, 60, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Walsh, S.D.; Djalovski, A.; Boniel-Nissim, M.; Harel-Fisch, Y. Parental, peer and school experiences as predictors of alcohol drinking among first and second generation immigrant adolescents in Israel. Drug Alcohol Depend. 2014, 138, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, J.E. Truth or consequences: The intertemporal consistency of adolescent self-report on the youth risk behavior survey. Am. J. Epidemiol. 2009, 169, 1388–1397. [Google Scholar] [CrossRef] [PubMed]
- Kuntsche, E.; Kuntsche, S.; Knibbe, R.; Simons-Morton, B.; Farhat, T.; Hublet, A. Cultural and gender convergence in adolescent drunkenness: Evidence from 23 European and North American countries. Arch. Pediatr. Adolesc. Med. 2011, 165, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Haugland, S.; Wold, B. Subjective health complaints in adolescence: Reliability and validity of survey methods. J. Adolesc. 2001, 24, 611–624. [Google Scholar] [CrossRef] [PubMed]
- Levin, K.A.; Currie, C. Reliability and validity of an adapted version of the Cantril ladder for use with adolescent samples. Soc. Indic. Res. 2013. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2008; ISBN 3-900051-07-0. [Google Scholar]


{kind=link}
| Variable | Parameter/Value | Intervention Group n = 53 | Control Group n = 23 | Total n = 76 | p-Value |
|---|---|---|---|---|---|
| Age | Mean (SD) | 16.9 (0.89%) | 16.7 (0.75%) | 16.9 (0.85%) | 0.367 a |
| Gender | Male | 28 (53%) | 13 (57%) | 41 (54%) | 0.767 b |
| Country of origin | Israel | 44 (83%) | 18 (78%) | 62 (82%) | 0.623 |
| Level of religiosity | Secular | 38 (72%) | 13 (57%) | 51 (67 %) | 0.212 c |
| Traditional | 13 (25%) | 9 (39%) | 22 (29%) | ||
| Religious | 2 (4%) | 1 (4%) | 3 (4%) | ||
| Socioeconomic status | Low | 7 (13%) | 5 (22%) | 12 (16%) | 0.845 |
| Average | 36 (68%) | 11 (48%) | 47 (62%) | ||
| Good | 9 (17%) | 7 (30%) | 16 (21%) | ||
| Very good | 1 (2%) | 0 | 1 (1%) | ||
| Mother’s education | Elementary | 0 | 0 | 1 (1%) | 0.298 |
| Middle school | 2 (4%) | 1 (5%) | 4 (6%) | ||
| High school | 24 (42%) | 13 (52%) | 31 (42%) | ||
| Professional * | 14 (26%) | 6 (26%) | 20 (26%) | ||
| Academic | 15 (28%) | 4 (17%) | 19 (25%) | ||
| Father’s education | Elementary | 1 (2%) | 0 | 1 (1%) | 0.971 |
| Middle school | 4 (7%) | 1 (5%) | 5 (7%) | ||
| High school | 19 (36%) | 11 (50%) | 30 (40%) | ||
| Professional * | 18 (34%) | 4 (18%) | 22 (29%) | ||
| Academic | 11 (21%) | 6 (27%) | 17 (23%) |
| Variables | Before Intervention | After Intervention | Change | p-Value | |||
|---|---|---|---|---|---|---|---|
| Study Mean (SD) | Control Mean (SD) | Study Mean (SD) | Control Mean (SD) | Study Mean (SD) | Control Mean (SD) | ||
| 60 min PA sessions in a week | 2.28 (0.80) | 1.74 (0.81) | 3.34 (1.21) | 2.00 (1.04) | 1.07 (1.44) | 0.26 (0.81) | 0.003 |
| Total after school PA hours | 2.71 (1.11) | 2.26 (1.25) | 4.21 (1.26) | 2.39 (1.34) | 1.52 (1.75) | 0.13 (1.06) | <0.001 |
| Frequency of smoking | 2.60 (1.30) | 3.17 (1.03) | 1.72 (1.08) | 3.39 (1.03) | −0.92 (1.57) | 0.22 (1.51) | 0.005 |
| Alcohol consumption | 3.74 (1.14) | 2.99 (1.54) | 2.68 (0.79) | 2.95 (1.38) | −1.08 (1.30) | −0.09(1.79) | 0.026 |
| Psychosomatic symptoms | 2.91 (0.78) | 2.05 (0.45) | 1.54 (0.43) | 1.94 (0.60) | −1.37 (0.76) | −0.18(0.70) | <0.001 |
| Life satisfaction | 6.21 (1.75) | 6.82 (2.28) | 7.62 (1.01) | 6.45 (2.46) | 1.42 (1.99) | −0.29(2.69) | 0.013 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tesler, R.; Plaut, P.; Endvelt, R. The Effects of an Urban Forest Health Intervention Program on Physical Activity, Substance Abuse, Psychosomatic Symptoms, and Life Satisfaction among Adolescents. Int. J. Environ. Res. Public Health 2018, 15, 2134. https://doi.org/10.3390/ijerph15102134
Tesler R, Plaut P, Endvelt R. The Effects of an Urban Forest Health Intervention Program on Physical Activity, Substance Abuse, Psychosomatic Symptoms, and Life Satisfaction among Adolescents. International Journal of Environmental Research and Public Health. 2018; 15(10):2134. https://doi.org/10.3390/ijerph15102134
Chicago/Turabian StyleTesler, Riki, Pnina Plaut, and Ronit Endvelt. 2018. "The Effects of an Urban Forest Health Intervention Program on Physical Activity, Substance Abuse, Psychosomatic Symptoms, and Life Satisfaction among Adolescents" International Journal of Environmental Research and Public Health 15, no. 10: 2134. https://doi.org/10.3390/ijerph15102134
APA StyleTesler, R., Plaut, P., & Endvelt, R. (2018). The Effects of an Urban Forest Health Intervention Program on Physical Activity, Substance Abuse, Psychosomatic Symptoms, and Life Satisfaction among Adolescents. International Journal of Environmental Research and Public Health, 15(10), 2134. https://doi.org/10.3390/ijerph15102134