Environmental Drivers of Bacillus-Positive Blood Cultures in a Cancer Hospital, Sapporo, Japan



Abstract
:1. Introduction
2. Materials and Methods
2.1. Blood Culture Sampling
2.2. Microbiological Method
2.3. Environmental Variables
2.4. Statistical Analysis
2.5. Ethical Consideration
3. Results
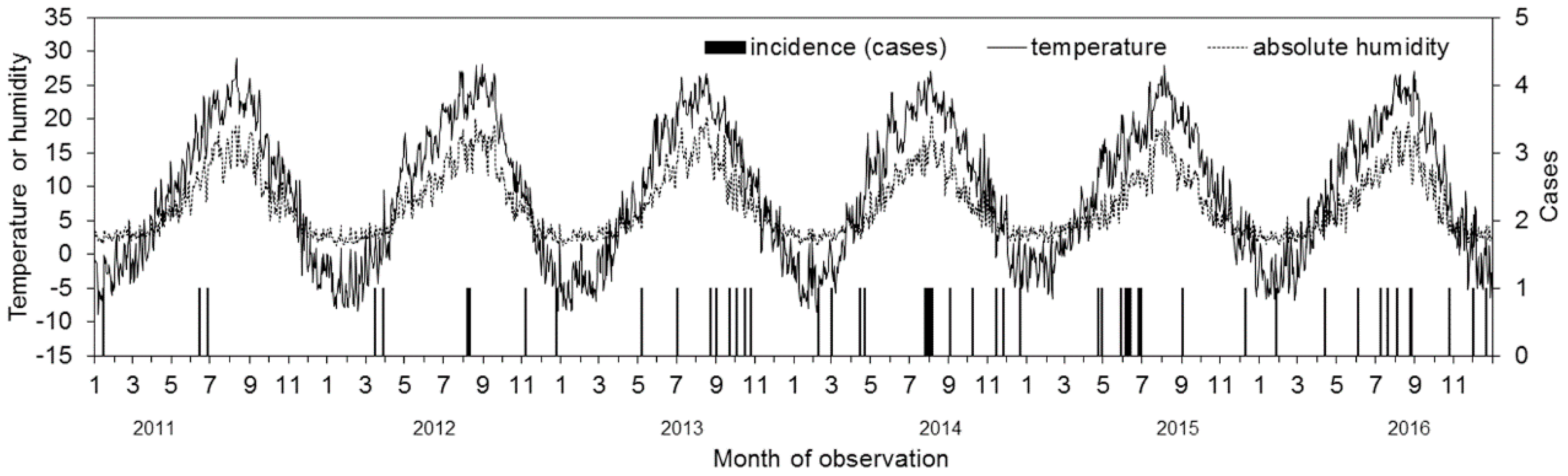
3.1. Descriptive Data
3.2. Univariate Analysis
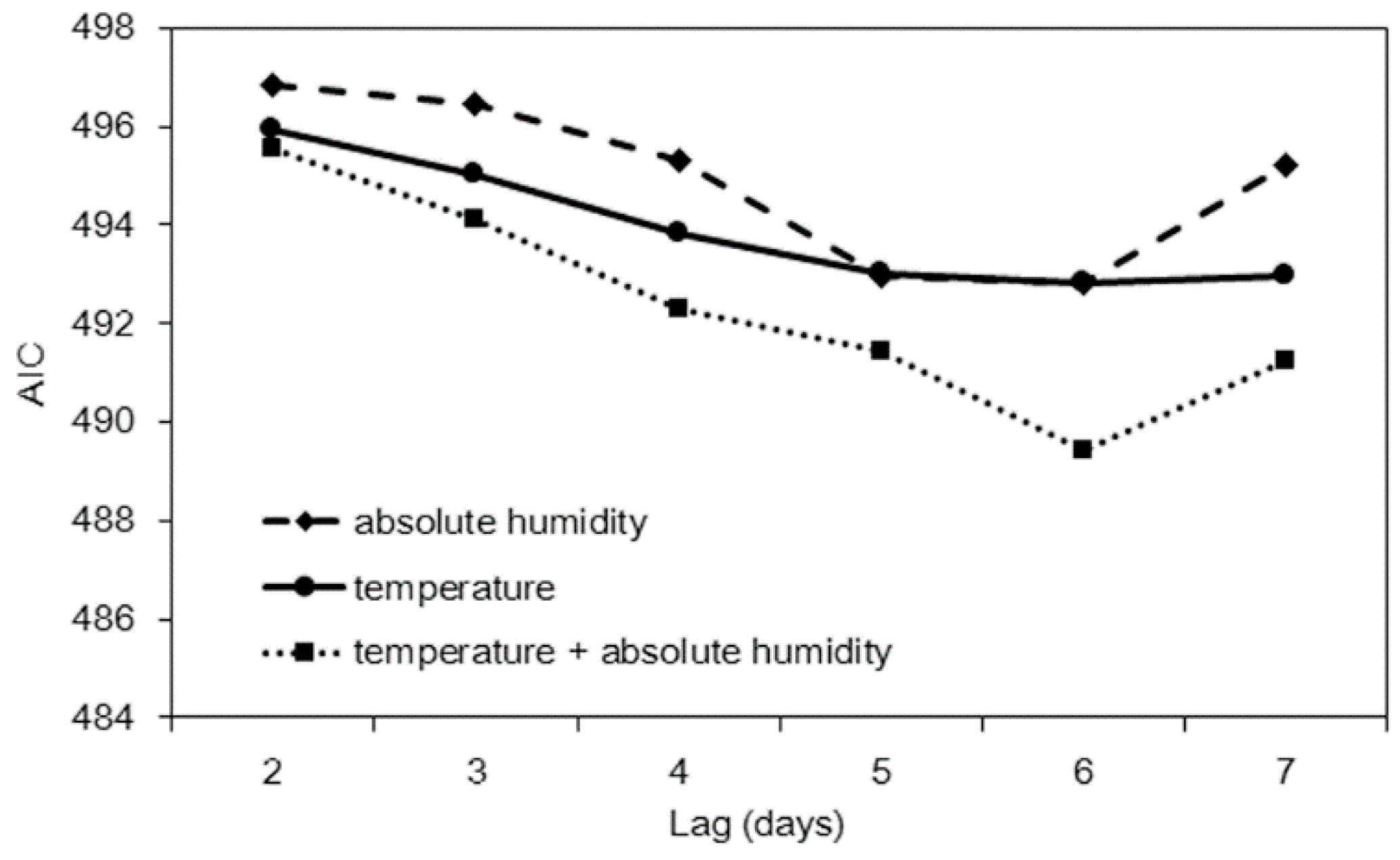
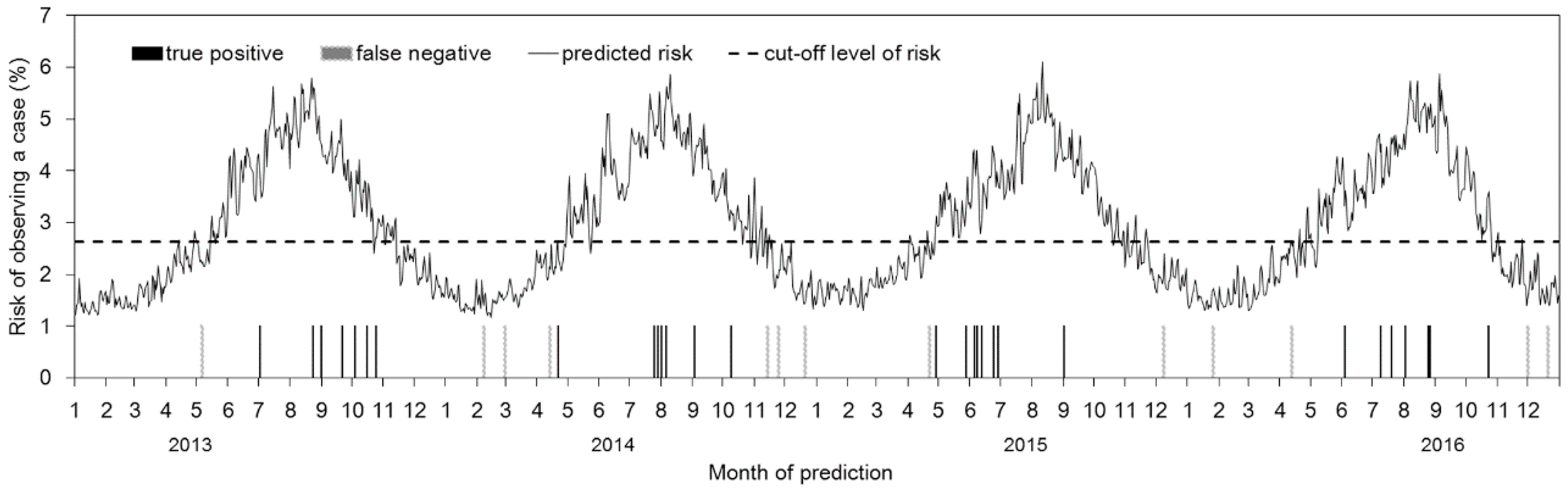
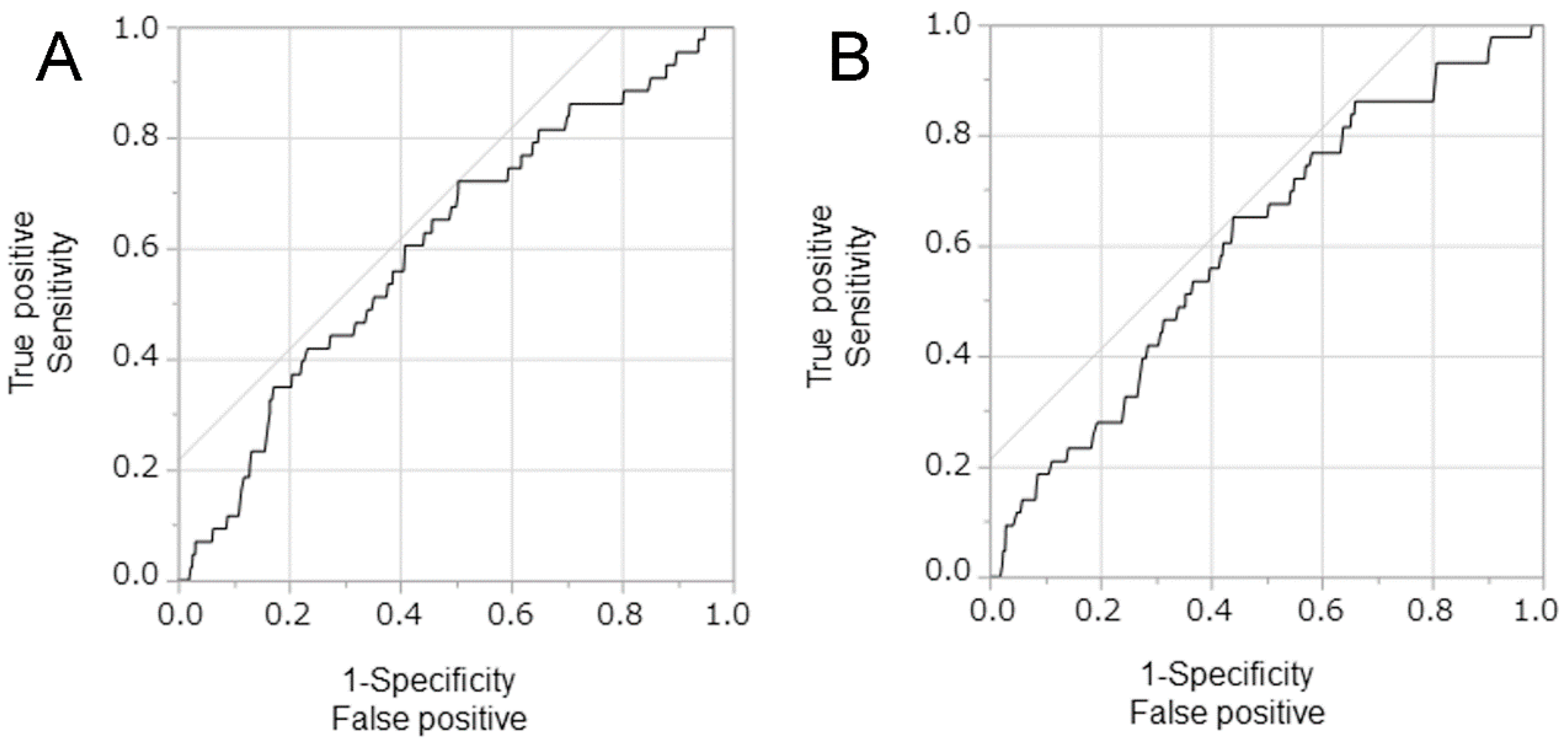
3.3. Multivariate Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Drobniewski, F.A. Bacillus cereus and related species. Clin. Microbiol. Rev. 1993, 6, 324–338. [Google Scholar] [CrossRef] [PubMed]
- Bottone, E.J. Bacillus cereus, a volatile human pathogen. Clin. Microbiol. Rev. 2010, 23, 382–398. [Google Scholar] [CrossRef] [PubMed]
- Sliman, R.; Rehm, S.; Shlaes, D.M. Serious infections caused by Bacillus species. Medicine 1987, 66, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Bryce, E.A.; Smith, J.A.; Tweeddale, M.; Andruschak, B.J.; Maxwell, M.R. Dissemination of Bacillus cereus in an intensive care unit. Infect. Control Hosp. Epidemiol. 1993, 14, 459–462. [Google Scholar] [CrossRef] [PubMed]
- Gray, J.; George, R.H.; Durbin, G.M.; Ewer, A.K.; Hocking, M.D.; Morgan, M.E. An outbreak of Bacillus cereus respiratory tract infections on a neonatal unit due to contaminated ventilator circuits. J. Hosp. Infect. 1999, 41, 19–22. [Google Scholar] [CrossRef]
- Barrie, D.; Wilson, J.A.; Hoffman, P.N.; Kramer, J.M. Bacillus cereus meningitis in two neurosurgical patients: An investigation into the source of the organism. J. Infect. 1992, 25, 291–297. [Google Scholar] [CrossRef]
- Loeb, M.; Wilcox, L.; Thornley, D.; Gun-Munro, J.; Richardson, H. Bacillus species pseudobacteremia following hospital construction. Can. J. Infect. Control. 1995, 10, 37–40. [Google Scholar] [PubMed]
- Boix-Palop, L.; Nicolás, C.; Xercavins, M.; Riera, M.; Prim, N.; Freixas, N.; Pérez, J.; Calbo, E. Bacillus species pseudo-outbreak: Construction works and collateral damage. J. Hosp. Infect. 2017, 95, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Sasahara, T.; Hayashi, S.; Morisawa, Y.; Sakihama, T.; Yoshimura, A.; Hirai, Y. Bacillus cereus bacteremia outbreak due to contaminated hospital linens. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Saito, N.; Kondo, J.; Haruki, S.; Itoga, M.; Yamamoto, A.; Kimura, M.; Tsutaya, S.; Kojima, K.; Ueki, S. Possible involvement of reusable towels in the high rate of Bacillus species-positive blood cultures in Japanese hospitals. J. Infect. Chemother. 2016, 22, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Matsumura, Y.; Yamamoto, M.; Nagao, M.; Ito, Y.; Takakura, S.; Ichiyama, S. Seasonal trend and clinical presentation of Bacillus cereus bloodstream infection: Association with summer and indwelling catheter. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1371–1379. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, M.; Yagihara, Y.; Tatsuno, K.; Okazaki, M.; Okugawa, S.; Moriya, K. Clinical characteristics and antimicrobial susceptibility of Bacillus cereus blood stream infections. Ann. Clin. Microbiol. Antimicrob. 2015, 14, 43. [Google Scholar] [CrossRef] [PubMed]
- Ashkenazi-Hoffnung, L.; Kaufman, Z.; Bromberg, M.; Block, C.; Keller, N.; Dictar, R.; Goldberg, A.; Green, M.S. Seasonality of Bacillus species isolated from blood cultures and its potential implications. Am. J. Infect. Control. 2009, 37, 495–499. [Google Scholar] [CrossRef] [PubMed]
- Mercaldo, N.D.; Lau, K.F.; Zhou, X.H. Confidence intervals for predictive values with an emphasis to case-control studies. Stat. Med. 2007, 26, 2170–2183. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Kutsuna, S.; Hayakawa, K.; Kita, K.; Katanami, Y.; Imakita, N.; Kasahara, K.; Seto, M.; Akazawa, K.; Shimizu, M.; Kano, T.; et al. Risk factors of catheter-related bloodstream infection caused by Bacillus cereus: Case-control study in 8 teaching hospitals in Japan. Am. J. Infect. Control 2017, 45, 1281–1283. [Google Scholar] [CrossRef] [PubMed]
- Horii, T.; Notake, S.; Tamai, K.; Yanagisawa, H. Bacillus cereus from blood cultures: Virulence genes, antimicrobial susceptibility and risk factors for blood stream infection. FEMS Immunol. Med. Microbiol. 2011, 63, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Sakihama, T.; Tokuda, Y. Use of Peripheral Parenteral Nutrition Solutions as a Risk Factor for Bacillus cereus Peripheral Venous Catheter-Associated Bloodstream Infection at a Japanese Tertiary Care Hospital: A Case-Control Study. Jpn. J. Infect. Dis. 2016, 69, 531–533. [Google Scholar] [CrossRef] [PubMed]
- Dohmae, S.; Okubo, T.; Higuchi, W.; Takano, T.; Isobe, H.; Baranovich, T.; Kobayashi, S.; Uchiyama, M.; Tanabe, Y.; Itoh, M.; et al. Bacillus cereus nosocomial infection from reused towels in Japan. J. Hosp. Infect. 2008, 69, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Hosein, I.K.; Hoffman, P.N.; Ellam, S.; Asseez, T.-M.; Fakokunde, A.; Silles, J.; Devereux, E.; Kaur, D.; Bosanquet, J. Summertime Bacillus cereus colonization of hospital newborns traced to contaminated, laundered linen. J. Hosp. Infect. 2013, 85, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Balm, M.N.D.; Jureen, R.; Teo, C.; Yeoh, A.E.J.; Lin, R.T.P.; Dancer, S.J.; Fisher, D.A. Hot and steamy: Outbreak of Bacillus cereus in Singapore associated with construction work and laundry practices. J. Hosp. Infect. 2012, 81, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Ohsaki, Y.; Koyano, S.; Tachibana, M.; Shibukawa, K.; Kuroki, M.; Yoshida, I.; Ito, Y. Undetected Bacillus pseudo-outbreak after renovation work in a teaching hospital. J. Infect. 2007, 54, 617–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Odds Ratio (95% CI †) | p-Value |
|---|---|---|
| Mean temperature (Celsius) | 1.04 (1.01, 1.08) | 0.018 |
| Absolute humidity (g/m3) | 1.07 (1.00, 1.13) | 0.033 |
| Hours of sunlight (hours) | 1.02 (0.94, 1.10) | 0.621 |
| Speed of wind (m/s) | 0.94 (0.75, 1.13) | 0.516 |
| Variable (Lag Days) | Sensitivity | Specificity | PPV | NPV | AUC | AIC |
|---|---|---|---|---|---|---|
| Mean temperature (Celsius) (6 days) | 72.1 (56.3, 84.7) | 49.5 (46.8, 52.1) | 4.1 (2.8, 5.8) | 98.3 (97.1, 99.1) | 0.61 (0.59, 0.64) | 492.8 |
| Absolute humidity (g/m3) (6 days) | 72.1 (56.3, 84.7) | 48.8 (46.1, 51.4) | 4.1 (2.8 5.8) | 98.3 (97.0 99.1) | 0.59 (0.57, 0.62) | 492.8 |
| Mean temperature + Absolute humidity (6 days) | 65.1 (49.1, 79.0) | 56.0 (53.3, 58.6) | 4.3 (2.9, 6.1) | 98.1 (97.0, 99.0) | 0.61 (0.58, 0.63) | 489.4 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujita, T.; Nishiura, H. Environmental Drivers of Bacillus-Positive Blood Cultures in a Cancer Hospital, Sapporo, Japan. Int. J. Environ. Res. Public Health 2018, 15, 2201. https://doi.org/10.3390/ijerph15102201
Fujita T, Nishiura H. Environmental Drivers of Bacillus-Positive Blood Cultures in a Cancer Hospital, Sapporo, Japan. International Journal of Environmental Research and Public Health. 2018; 15(10):2201. https://doi.org/10.3390/ijerph15102201
Chicago/Turabian StyleFujita, Takahiro, and Hiroshi Nishiura. 2018. "Environmental Drivers of Bacillus-Positive Blood Cultures in a Cancer Hospital, Sapporo, Japan" International Journal of Environmental Research and Public Health 15, no. 10: 2201. https://doi.org/10.3390/ijerph15102201
APA StyleFujita, T., & Nishiura, H. (2018). Environmental Drivers of Bacillus-Positive Blood Cultures in a Cancer Hospital, Sapporo, Japan. International Journal of Environmental Research and Public Health, 15(10), 2201. https://doi.org/10.3390/ijerph15102201