Introducing a Dynamic Workstation in the Office: Insights in Characteristics of Use and Short-Term Changes of Well-Being in a 12 Week Observational Study

Abstract
:1. Introduction
- How do employees use cycling devices in a real-life office environment?
- Does using a cycling device in a real-life office environment correspond with short-term changes in well-being?
- Do different characteristics of use (average duration of use per event, bouts of use within one event of use, speed and consistency of cycling) relate to possible short-term changes in well-being?
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Intervention
2.4. Measures
2.4.1. Characteristics of Using the Deskbike
- The date and the code of the RFID-chip card were registered to identify participants using the device at that day of the intervention period.
- The duration of use was recorded minute by minute and summarized per event.
- The total number of bouts of use was calculated as the total of all periods in which complete revolutions of the pedals per minute were recorded per event. A break was identified as a minute of zero rpm-values.
- Revolutions per minute (rpm) were recorded by the chip-card every time the pedals completed one revolution. This measurement shows the individual speed of using a Deskbike.
- Standard Deviation of rpm expresses how steadily a participant used the Deskbike in terms of the speed of cycling.
- Rated Perceived Exertion was assessed with the RPE-scale (Rated Perceived Exertion [46]). Immediately after using a Deskbike the participants were asked to rate the subjective intensity of using it from 5 (no exertion) to 20 (extremely hard) via the online survey. These outcomes were used to subjectively evaluate the intensity of using the Deskbike.
2.4.2. Short-Term Effects on Well-Being
2.5. Data-Analysis
3. Results
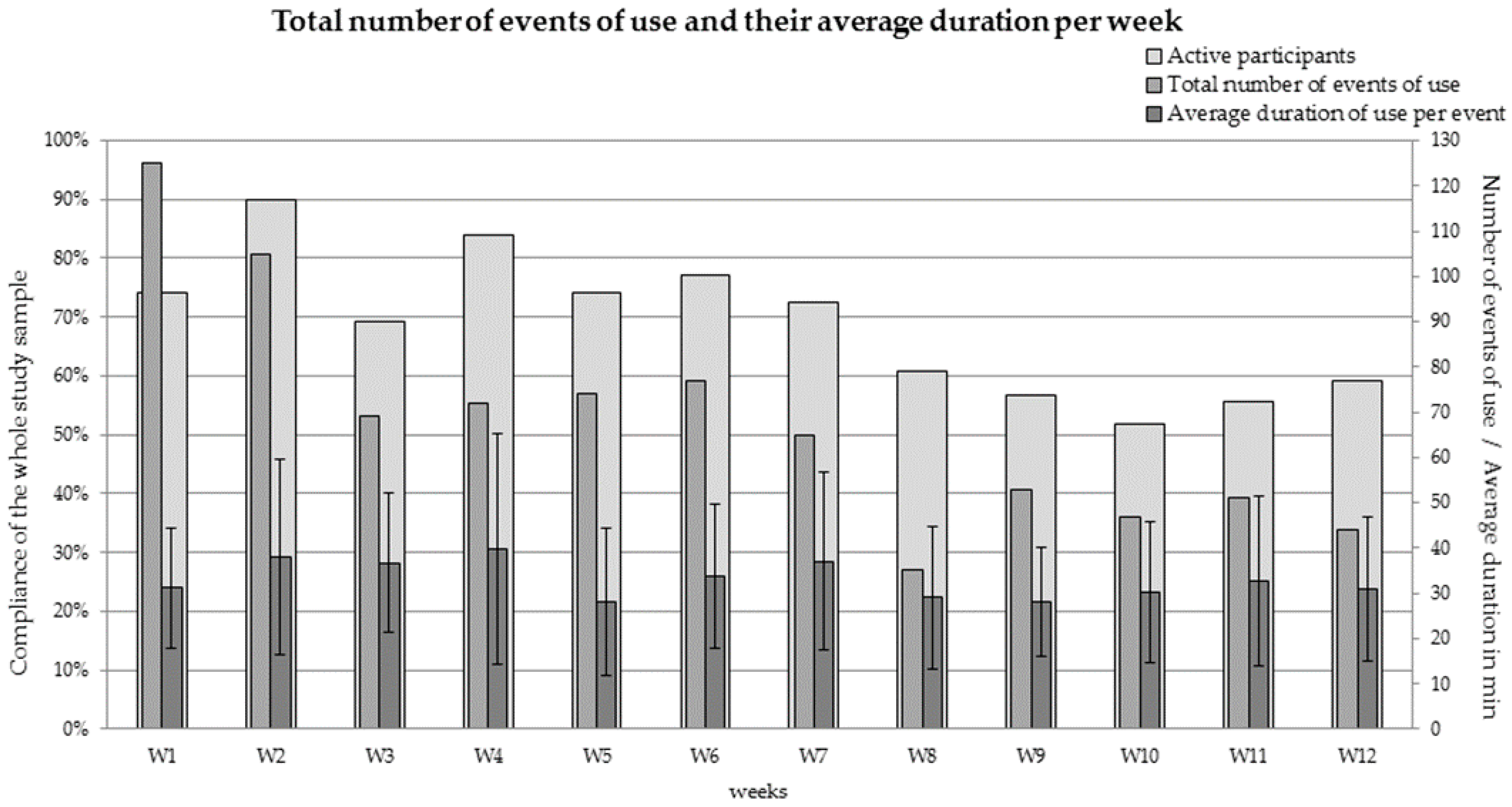
3.1. Characteristics of Use
3.2. Short-Term Changes in Well-Being
3.3. Relationships of Different Characteristics of Use with Short-Term Changes in Well-Being
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Biddle, S.J.; Bennie, J.A.; Bauman, A.E.; Chau, J.Y.; Dunstan, D.; Owen, N.; Stamatakis, E.; van Uffelen, J.G. Too much sitting and all-cause mortality: Is there a causal link? BMC Public Health 2016, 16, 635. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.M.; Lancet Physical Activity Series; Lancet Sedentary Behaviour Working Group. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Loyen, A.; Verloigne, M.; Van Hecke, L.; Hendriksen, I.; Lakerveld, J.; Steene-Johannessen, J.; Koster, A.; Donnelly, A.; Ekelund, U.; Deforche, B.; et al. Variation in population levels of physical activity in European adults according to cross-European studies: A systematic literature review within DEDIPAC. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennie, J.A.; Chau, J.Y.; van der Ploeg, H.P.; Stamatakis, E.; Do, A.; Bauman, A. The prevalence and correlates of sitting in European adults—A comparison of 32 Eurobarometer-participating countries. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 107. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.; Ainsworth, B.E.; Sallis, J.F.; Hagströmer, M.; Craig, C.L.; Bull, F.C.; Pratt, M.; Venugopal, K.; Chau, J.; Sjöström, M.; et al. The descriptive epidemiology of sitting. A 20-country comparison using the International Physical Activity Questionnaire (IPAQ). Am. J. Prev. Med. 2011, 41, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Lakerveld, J.; Loyen, A.; Schotman, N.; Peeters, C.F.W.; Cardon, G.; van der Ploeg, H.P.; Lien, N.; Chastin, S.; Brug, J. Sitting too much: A hierarchy of socio-demographic correlates. Prev. Med. 2017, 101, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Thorp, A.A.; Healy, G.N.; Owen, N.; Salmon, J.; Ball, K.; Shaw, J.E.; Zimmet, P.Z.; Dunstan, D.W. Deleterious associations of sitting time and television viewing time with cardiometabolic risk biomarkers: Australian Diabetes, Obesity and Lifestyle (AusDiab) study 2004–2005. Diabetes Care 2010, 33, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Parry, S.; Straker, L.; Gilson, N.D.; Smith, A.J. Participatory workplace interventions can reduce sedentary time for office workers—A randomised controlled trial. PLoS ONE 2013, 8, e78957. [Google Scholar] [CrossRef] [PubMed]
- Tennant, C. Work-related stress and depressive disorders. J. Psychosomat. Res. 2001, 51, 697–704. [Google Scholar] [CrossRef]
- Morgan, W.P.; Goldston, S.E. Exercise and Mental Health; Hemisphere Publishing Corporation: Philadelphia, PA, USA, 1987; ISBN 9700891165644. [Google Scholar]
- Hearing, C.M.; Chang, W.C.; Szuhany, K.L.; Deckersbach, T.; Nierenberg, A.A.; Sylvia, L.G. Physical Exercise for Treatment of Mood Disorders: A Critical Review. Curr. Behav. Neurosci. Rep. 2016, 3, 350–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mammen, G.; Faulkner, G. Physical activity and the prevention of depression: A systematic review of prospective studies. Am. J. Prev. Med. 2013, 45, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Biddle, S.J.H.; Mutrie, N. Psychology of Physical Activity: Determinants, Well-Being, and Interventions, 2nd ed.; Routledge: New York, NY, USA, 2008. [Google Scholar] [CrossRef]
- Gerber, M.; Pühse, U. Review article: Do exercise and fitness protect against stress-induced health complaints? A review of the literature. Scand. J. Public Health 2009, 37, 801–819. [Google Scholar] [CrossRef] [PubMed]
- Arent, S.M.; Landers, D.M.; Etnier, J.L. The effects of exercise on mood in older adults: A meta-analytic review. J. Aging Phys. Act. 2000, 8, 407–430. [Google Scholar] [CrossRef]
- Biddle, S.J.H. Emotion, mood and physical activity. In Physical Activity and Psychological Well-Being; Biddle, S.J.H., Fox, K.R., Boutcher, S.H., Eds.; Routledge: London, UK, 2000; pp. 63–87. [Google Scholar]
- Ekeland, E.; Heian, F.; Hagen, K.; Coren, E. Can exercise improve self esteem in children and young people? A systematic review of randomised controlled trials. Br. J. Sports Med. 2005, 39, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Spence, J.C.; McGannon, K.R.; Poon, P. The effect of exercise on global self-esteem: A quantitative review. J. Sport Exerc. Psychol. 2005, 27, 311–334. [Google Scholar] [CrossRef]
- Fox, K.R. Self-Esteem, Self-Perceptions and Exercise. Int. J. Sport Psychol. 2000, 31, 228–240. [Google Scholar]
- Leith, L.M. Foundation of Exercise and Mental Health; Fitness Information Technology: Morgantown, WV, USA, 1994; ISBN 978-1885693419. [Google Scholar]
- Sani, S.H.Z.; Fathirezaie, Z.; Brand, S.; Pühse, U.; Holsboer-Trachsler, E.; Gerber, M.; Talepasand, S. Physical activity and self-esteem: Testing direct and indirect relationships associated with psychological and physical mechanisms. Neuropsychiatr. Dis. Treat. 2016, 12, 2617–2625. [Google Scholar] [CrossRef] [PubMed]
- Penedo, F.J.; Dahn, J.R. Exercise and well-being: A review of mental and physical health benefits associated with physical activity. Curr. Opin. Psychiatry 2005, 18, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Abdin, S.; Welch, R.K.; Byron-Daniel, J.; Meyrick, J. The effectiveness of physical activity interventions in improving well-being across office-based workplace settings: A systematic review. Public Health 2018, 160, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Chu, A.H.; Koh, D.; Moy, F.M.; Muller-Riemenschneider, F. Do workplace physical activity interventions improve mental health outcomes? Occup. Med. (Lond.) 2014, 64, 235–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conn, V.S.; Hafdahl, A.R.; Cooper, P.S.; Brown, L.M.; Lusk, S.L. Meta-analysis of workplace physical activity interventions. Am. J. Prev. Med. 2009, 37, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, N.; Kukkonen-Harjula, K.T.; Verbeek, J.H.; Ijaz, S.; Hermans, V.; Bhaumik, S. Workplace interventions for reducing sitting at work. Cochrane Database Syst. Rev. 2016, 3, CD010912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuhaus, M.; Eakin, E.G.; Straker, L.; Owen, N.; Dunstan, D.W.; Reid, N.; Healy, G.N. Reducing occupational sedentary time: A systematic review and meta-analysis of evidence on activity-permissive workstations. Obes. Rev. 2014, 15, 822–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botter, J.; Ellegast, R.P.; Burford, E.M.; Weber, B.; Konemann, R.; Commissaris, D.A. Comparison of the postural and physiological effects of two dynamic workstations to conventional sitting and standing workstations. Ergonomics 2016, 59, 449–463. [Google Scholar] [CrossRef] [PubMed]
- Carr, L.J.; Maeda, H.; Luther, B.; Rider, P.; Tucker, S.J.; Leonhard, C. Acceptability and effects of a seated active workstation during sedentary work. Int. J. Workplace Health Manag. 2014, 7, 2–15. [Google Scholar] [CrossRef]
- Elmer, S.J.; Martin, J.C. A cycling workstation to facilitate physical activity in office settings. Appl. Ergon. 2014, 45, 1240–1246. [Google Scholar] [CrossRef] [PubMed]
- Straker, L.; Levine, J.; Campbell, A. The effects of walking and cycling computer workstations on keyboard and mouse performance. Hum. Factors 2009, 51, 831–844. [Google Scholar] [CrossRef] [PubMed]
- Carr, L.J.; Walaska, K.A.; Marcus, B.H. Feasibility of a portable pedal exercise machine for reducing sedentary time in the workplace. Br. J. Sports Med. 2012, 46, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Carr, L.J.; Karvinen, K.; Peavler, M.; Smith, R.; Cangelosi, K. Multicomponent intervention to reduce daily sedentary time: A randomised controlled trial. BMJ Open 2013, 3, e003261. [Google Scholar] [CrossRef] [PubMed]
- Carr, L.J.; Leonhard, C.; Tucker, S.; Fethke, N.; Benzo, R.; Gerr, F. Total Worker Health Intervention Increases Activity of Sedentary Workers. Am. J. Prev. Med. 2016, 50, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Torbeyns, T.; de Geus, B.; Bailey, S.; De Pauw, K.; Decroix, L.; Van Cutsem, J.; Meeusen, R. Bike Desks in the Office: Physical Health, Cognitive Function, Work Engagement, and Work Performance. J. Occup. Environ. Med. 2016, 58, 1257–1263. [Google Scholar] [CrossRef] [PubMed]
- Schellewald, V.; Kleinert, J.; Ellegast, R. Use and physiological responses of portable dynamic office workstations in an occupational setting—A field study. Appl. Ergon. 2018, 71, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Edelson, N.; Danoffz, J. Walking on an electric treadmill while performing VDT office work. ACM SIGCHI Bull. 1989, 21, 72–77. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Hendrick, C.A.; Duet, M.T.; Swift, D.L.; Schuna, J.M., Jr.; Martin, C.K.; Johnson, W.D.; Church, T.S. Implementation and adherence issues in a workplace treadmill desk intervention. Appl. Physiol. Nutr. Metab. 2014, 39, 1104–1111. [Google Scholar] [CrossRef] [PubMed]
- Sliter, M.; Yuan, Z. Workout at work: Laboratory test of psychological and performance outcomes of active workstations. J. Occup. Health Psychol. 2015, 20, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, E.A.; Western, M.J.; Nightingale, T.E.; Peacock, O.J.; Thompson, D. Assessment of laboratory and daily energy expenditure estimates from consumer multi-sensor physical activity monitors. PLoS ONE 2017, 12, e0171720. [Google Scholar] [CrossRef] [PubMed]
- Thompson, W.G.; Foster, R.C.; Eide, D.S.; Levinez, J.A. Feasibility of a walking workstation to increase daily walking. Br. J. Sports Med. 2008, 42, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Hassmen, P.; Koivula, N.; Uutela, A. Physical exercise and psychological well-being: A population study in Finland. Prev. Med. 2000, 30, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Netz, Y.; Wu, M.J.; Becker, B.J.; Tenenbaum, G. Physical activity and psychological well-being in advanced age: A meta-analysis of intervention studies. Psychol. Aging 2005, 20, 272–284. [Google Scholar] [CrossRef] [PubMed]
- Wicker, P.; Frick, B. The relationship between intensity and duration of physical activity and subjective well-being. Eur. J. Public Health 2015, 25, 868–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, C.J.; Stevens, L.C.; Coast, J.R. Exercise duration and mood state: How much is enough to feel better? Health Psychol. 2001, 20, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Nitsch, J.R. Die Eigenzustandsskala (EZ-Skala)—Ein Verfahren zur hierarchisch—Mehrdimensionalen Befindlichkeitsskalierung. In Beanspruchung im Sport. Beiträge zur Psychologischen Analyse Sportlicher Leistungssituationen; Nitsch, J.R., Udris, I., Eds.; Limpert: Bad Homburg, Germany, 1976; pp. 81–102. [Google Scholar]
- Nitsch, J.R. Die hierarchische Struktur des Eigenzustandes—Ein Approximationsverfahren mit Hilfe der Binärstrukturanalyse. Diagnostika 1974, 20, 142–164. [Google Scholar]
- Liang, K.-Y.; Zeger, S.L. Longitudinal Data Analysis Using Generalized Linear Models. Biometrika 1986, 73, 13–22. [Google Scholar] [CrossRef]
- Wasserkampf, A.; Silva, M.N.; Teixeira, P.J. Changing the quality of motivation over time in health and fitness settings. ACSMS Health Fit. J. 2017, 5, 33–39. [Google Scholar]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Perceived Exertion (Borg Rating of Perceived Exertion Scale); Centers for Disease Control and Prevention, U.S. Department of Health & Human Services: Atlanta, GA, USA, 2015. Available online: https://www.cdc.gov/physicalactivity/basics/measuring/exertion.htm (accessed on 7 November 2018).
- HealthLinkBC. Borg Rating of Perceived Exertion Scale. Available online: https://www.healthlinkbc.ca/physical-activity/borg-rating-perceived-exertion-scale (accessed on 7 November 2018).
- Leone, C.; Feys, P.; Moumdjian, L.; D’Amico, E.; Zappia, M.; Patti, F. Cognitive-motor dual-task interference: A systematic review of neural correlates. Neurosci. Biobehav. Rev. 2017, 75, 348–360. [Google Scholar] [CrossRef] [PubMed]
- Patela, P.; Lamarb, M.; Bhatta, T. Effect of type of cognitive task and walking speed on cognitive-motor interference during dual-task walking. Neuroscience 2014, 260, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Schott, N.; Klotzbier, T.J. Profiles of Cognitive-Motor Interference During Walking in Children: Does the Motor or the Cognitive Task Matter? Front. Psychol. 2018, 9, 947. [Google Scholar] [CrossRef] [PubMed]
- Agricola, P.M.; da Silva, M.D.G.; de Farias, J.L.F.; do Nascimento, N.L.I.; Fonteles, A.I.; da Silva, S.K.; Chao, C.H.; Fontes, E.B.; Elsangedy, H.M.; Okano, A.H. Slow Down and Enjoy: The Effects of Cycling Cadence on Pleasure. Percept. Mot. Skills 2017, 124, 233–247. [Google Scholar] [CrossRef] [PubMed]
- Stults-Kolehmainen, M.A.; Sinha, R. The effects of stress on physical activity and exercise. Sports Med. 2014, 44, 81–121. [Google Scholar] [CrossRef] [PubMed]
- Brehm, W. Stimmung und Stimmungsmanagement. In Gesundheitssport—Ein Handbuch; Bös, K., Brehm, W., Eds.; Hofmann: Schorndorf, Germany, 2006; pp. 319–333. [Google Scholar]
- Shain, M. Health Promotion in the Workplace: Framing the Concept; Reviewing the Evidence. Occup. Environ. Med. 2004, 61, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Goetzel, R.Z.; Ozminkowski, R.J. The health and cost benefits of work site health-promotion programs. Annu. Rev. Public Health 2008, 29, 303–323. [Google Scholar] [CrossRef] [PubMed]
- Kirsten, W. Making the Link between Health and Productivity at the Workplace—A Global Perspective. Ind. Health 2010, 48, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Merchant, J.A.; Kelly, K.M.; Burmeister, L.F.; Lozier, M.J.; Amendola, A.; Lind, D.P.; KcKeen, A.; Slater, T.; Hall, J.L.; Rohlman, D.S.; et al. Employment status matters: A statewide survey of quality-of-life, prevention behaviors, and absenteeism and presenteeism. J. Occup. Environ. Med. 2014, 56, 686–698. [Google Scholar] [CrossRef] [PubMed]
- Hassard, J.; Teoh, K.; Cox, T.; Dewe, P.; Cosmar, M.; Gründler, R.; Flemming, D.; Cosemans, B.; Van den Broek, K. Calculating the Cost of Work-Related Stress and Psychosocial Risks—A Literature Review; European Agency for Safety and Health at Work-EU-OSHA: Bilbao, Spain, 2014; ISBN 978-92-9240-420-8. [Google Scholar]
- Broughton, A. Work-Related Stress; Institute for Employment Studies (IES): London, UK, 2010. [Google Scholar]
- Weineck, J. Der Einfluss von Sport und Bewegung auf die Zerebrale Leistungsfähigkeit; Bayern, D.S., Ed.; ISSW Erlangen: Erlangen, Germany, 2012. [Google Scholar]
- Pfeifer, K.; Banzer, W.; Ferrari, N.; Füzéki, E.; Geidl, W.; Graf, C.; Hartung, V.; Klamroth, S.; Völker, K.; Vog, L. Empfehlungen für Bewegung. In Nationale Empfehlungen für Bewegung und Bewegungsförderung; Rütten, A., Pfeifer, K., Eds.; FAU Erlangen-Nürnberg: Erlangen-Nürnberg, Germany, 2016; pp. 18–49. ISBN 978-3-946692-30-0. [Google Scholar]
- Froböse, I.; Kleinert, J.; Akkerman, G.; Biallas, B.; Jüngling, S.; Sulprizio, M. Aktiv Sein—Für Mich. Auswirkungen von Bewegung auf die Psychische Gesundheit von Frauen; Gesundheit, Z.F., Ed.; Bundesministerium für Gesundheit: Berlin, Germany, 2012. [Google Scholar]
- Benson, H.M.D.; Klipper, M.Z. The Relaxation Response; Harper Collins: New York, NY, USA, 2000; ISBN 978-0380006762. [Google Scholar]
- Wallner, P.; Kundi, M.; Panny, M.; Tappler, P.; Hutter, H.-P. Exposure to Air Ions in Indoor Environments: Experimental Study with Healthy Adults. Int. J. Environ. Res. Public Health 2015, 12, 14301–14311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallner, P.; Kundi, M.; Arnberger, A.; Eder, R.; Allex, B.; Weitensfelder, L.; Hutter, H.-P. Reloading Pupils’ Batteries: Impact of Green Spaces on Cognition and Wellbeing. Int. J. Environ. Res. Public Health 2018, 15, 1205. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Participants | Number | Age in Years | Height in Meters | Weight in kg | BMI |
|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | M (SD) | ||
| All | 36 | 41.0 (10.7) | 1.74 (0.10) | 76.9 (18.3) | 25.2 (5.0) |
| Male | 17 | 43.2 (11.4) | 1.82 (0.08) | 86.4 (13.9) | 26.0 (2.8) |
| Female | 19 | 39.1 (10.1) | 1.71 (0.05) | 72.2 (18.0) | 24.7 (6.4) |
| Categories | Characteristics of Use | |||
|---|---|---|---|---|
| Duration of Use per Event (min) | Number of Use Bouts per Event | Mean rpm per Event | Mean SD of rpm per Event | |
| 1 | ≤22.1 | 1 | ≤35.35 | ≤5.44 |
| 2 | 22.1 to 36.13 | 1 to 4 | 35.35 to 40.40 | 5.44 to 10.38 |
| 3 | 36.13 to 51.83 | ≥4 | ≥40.40 | ≥10.38 |
| 4 | ≥51.83 | - | - | - |
| Variables | Min | Max |
|---|---|---|
| Duration of use per event in min | 1 | 151.7 |
| Total number of use bouts per event | 1 | 25 |
| Mean revolution per minute (rpm) per event of use | 1 | 46.4 |
| Mean standard deviation of rpm per event of use | 0 | 24.5 |
| Variables | Pre | Post | t-Test | ||
|---|---|---|---|---|---|
| M (SD) | M (SD) | t | p-Value | Effect Size (d) | |
| recovery | 4.50 (0.92) | 4.77 (0.64) | −1.753 | 0.089 | 0.33 |
| self-confidence | 5.08 (0.87) | 5.34 (0.59) | −2.441 | 0.020 * | 0.32 |
| calm | 5.16 (0.80) | 5.38 (0.54) | −2.991 | 0.005 * | 0.28 |
| mood | 5.00 (0.80) | 5.26 (0.61) | −3.867 | 0.001 * | 0.34 |
| willingness to perform | 4.46 (0.91) | 4.80 (0.64) | −3.094 | 0.004 * | 0.40 |
| Parameter | Category | Recovery | Self-Confidence | Calm | Mood | Willingness to Perform | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95%-CI | p | OR | 95%-CI | p | OR | 95%-CI | p | OR | 95%-CI | p | OR | 95%-CI | p | ||
| Duration of use per event in min | ≤22.1 | 1 | 1 | 1 | 1 | 1 | ||||||||||
| 22.1 to 36.13 | 1.76 | 0.90–3.42 | 0.10 | 0.88 | 0.57–1.35 | 0.55 | 1.44 | 0.73–2.83 | 0.30 | 1.07 | 0.47–2.45 | 0.87 | 1.18 | 0.72–1.94 | 0.52 | |
| 36.13 to 51.83 | 2.22 | 1.18–4.20 | 0.01 | 0.60 | 0.31–1.15 | 0.12 | 1.95 | 0.89–4.28 | 0.10 | 1.52 | 0.68–3.42 | 0.31 | 1.36 | 0.80–2.34 | 0.26 | |
| ≥51.83 | 2.21 | 0.88–5.53 | 0.09 | 1.09 | 0.50–2.38 | 0.84 | 1.21 | 0.32–4.62 | 0.78 | 1.00 | 0.41–2.46 | 1.00 | 1.38 | 0.73–2.59 | 0.32 | |
| Number of bouts of use per event | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||||
| 2 to 4 | 0.97 | 0.64–1.48 | 0.89 | 0.85 | 0.42–1.72 | 0.65 | 1.15 | 0.52–2.53 | 0.74 | 0.88 | 0.45–1.71 | 0.70 | 0.92 | 0.44–1.93 | 0.82 | |
| ≥4 | 0.59 | 0.20–1.71 | 0.33 | 0.69 | 0.10–4.66 | 0.70 | 1.26 | 0.41–3.90 | 0.69 | 0.91 | 0.30–2.76 | 0.87 | 1.81 | 0.60–5.43 | 0.29 | |
| Mean rpm per event of use | ≤35.35 | 1 | 1 | 1 | 1 | 1 | ||||||||||
| 35.35 to 40.40 | 1.60 | 1.10–2.33 | 0.01 | 0.85 | 0.56–1.29 | 0.45 | 0.77 | 0.54–1.08 | 0.13 | 0.50 | 0.32–0.78 | ≤0.01 | 0.99 | 0.59–1.66 | 0.96 | |
| ≥40.40 | 1.03 | 0.63–1.69 | 0.91 | 0.75 | 0.42–1.31 | 0.31 | 1.02 | 0.43–2.42 | 0.96 | 0.65 | 0.39–1.08 | 0.10 | 1.06 | 0.51–2.22 | 0.87 | |
| Mean SD of rpm per event of use | ≤5.44 | 1 | 1 | 1 | 1 | 1 | ||||||||||
| 5.44 to 10.38 | 1.34 | 0.93–1.92 | 0.12 | 1.50 | 1.00–2.27 | 0.052 | 1.46 | 0.76–2.77 | 0.25 | 1.61 | 1.03–2.52 | 0.04 | 0.92 | 0.61–1.38 | 0.68 | |
| ≥10.38 | 0.52 | 0.31–0.86 | 0.01 | 0.71 | 0.37–1.36 | 0.30 | 1.82 | 1.22–2.73 | ≤0.01 | 1.12 | 0.57–2.20 | 0.73 | 0.59 | 0.35–1.00 | 0.051 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schellewald, V.; Kleinert, J.; Ellegast, R. Introducing a Dynamic Workstation in the Office: Insights in Characteristics of Use and Short-Term Changes of Well-Being in a 12 Week Observational Study. Int. J. Environ. Res. Public Health 2018, 15, 2501. https://doi.org/10.3390/ijerph15112501
Schellewald V, Kleinert J, Ellegast R. Introducing a Dynamic Workstation in the Office: Insights in Characteristics of Use and Short-Term Changes of Well-Being in a 12 Week Observational Study. International Journal of Environmental Research and Public Health. 2018; 15(11):2501. https://doi.org/10.3390/ijerph15112501
Chicago/Turabian StyleSchellewald, Vera, Jens Kleinert, and Rolf Ellegast. 2018. "Introducing a Dynamic Workstation in the Office: Insights in Characteristics of Use and Short-Term Changes of Well-Being in a 12 Week Observational Study" International Journal of Environmental Research and Public Health 15, no. 11: 2501. https://doi.org/10.3390/ijerph15112501
APA StyleSchellewald, V., Kleinert, J., & Ellegast, R. (2018). Introducing a Dynamic Workstation in the Office: Insights in Characteristics of Use and Short-Term Changes of Well-Being in a 12 Week Observational Study. International Journal of Environmental Research and Public Health, 15(11), 2501. https://doi.org/10.3390/ijerph15112501