Factors Associated with Satisfaction of Hospital Physicians: A Systematic Review on European Data

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Search Methods and Study Identification
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
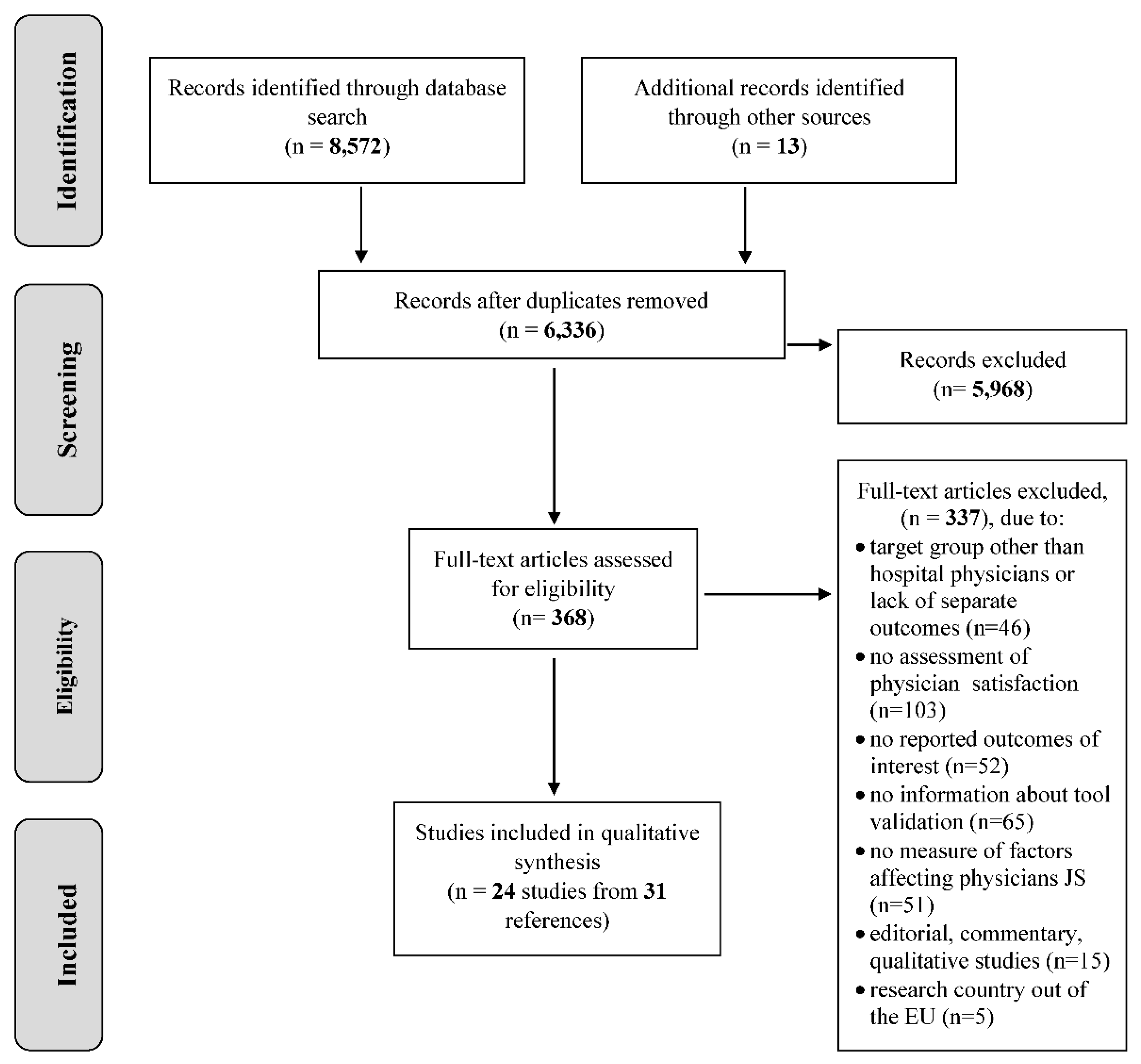
3.1. Search Results
3.2. Study Quality
3.3. Study Characteristic
3.3.1. Personal Factors
Physician Age
Gender
Years of Experience/Years of Practice
Marital Status or Having a Partner
Work-Family Conflict (WFC)
Health Status and Life Satisfaction
Coping Strategies/Psychological Construct
Being a Foreign/Internationally Trained Doctor
3.3.2. Intrinsic Factors
Specialty
Patient Interaction
Work Engagement
3.3.3. Contextual Factors: Workplace Related
Hospital Type and Structure
Management/Leadership
Opportunity for Professional Development
Colleague Support (Team Work, Team Relations)
Access to Resources
3.3.4. Contextual Factors: Job Related Factors
Workload and Job Demand
Work Control
Work Stability
Being a Chief
Income and Non-Financial Incentives
3.3.5. Contextual Factors: Others Factors
Intention to Leave
Prior Achievements
4. Discussion
4.1. Limitations
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Wallace, J.E.; Lemaire, J.B.; Ghali, W.A. Physician wellness: A missing quality indicator. Lancet 2009, 374, 1714–1721. [Google Scholar] [CrossRef]
- Escribà-Agüir, V.; Artazcoz, L.; Pérez-Hoyos, S. Effect of psychosocial work environment and job satisfaction on burnout syndrome among specialist physicians. Gac. Sanit. 2008, 22, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.; Skinner, A. Outcomes of physician job satisfaction: A narrative review, implications, and directions for future research. Health Care Manag. Rev. 2003, 28, 119–140. [Google Scholar] [CrossRef]
- Scheepers, R.A.; Boerebach, B.C.; Arah, O.A.; Heineman, M.J.; Lombarts, K.M. A Systematic Review of the Impact of Physicians’ Occupational Well-Being on the Quality of Patient Care. Int. J. Behav. Med. 2015, 22, 683–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S. Why are doctors so unhappy? Medical profession must unite to address problems. BMJ 2001, 322, 1363. [Google Scholar] [CrossRef] [PubMed]
- Friedberg, M.W.; Chen, P.G.; Van Busum, K.R.; Aunon, F.; Pham, C.; Caloyeras, J.; Mattke, S.; Pitchforth, E.; Quigley, D.D.; Brook, R.H.; et al. Factors Affecting Physician Professional Satisfaction and Their Implications for Patient Care, Health Systems, and Health Policy. Rand Health Q. 2014, 3, 1. [Google Scholar] [PubMed]
- Scheurer, D.; McKean, S.; Miller, J.; Wetterneck, T. US physician satisfaction: A systematic review. J. Hosp. Med. 2009, 4, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Hoff, T.; Young, G.; Xiang, E.; Raver, E. Understanding U.S. Physician Satisfaction: State of the Evidence and Future Directions. J. Healthc. Manag. 2015, 60, 409–427. [Google Scholar] [CrossRef] [PubMed]
- Wallace, J.E.; Lemaire, J. On physician well being-you’ll get by with a little help from your friends. Soc. Sci. Med. 2007, 64, 2565–2577. [Google Scholar] [CrossRef] [PubMed]
- Stoddard, J.; Hargraves, J.; Reed, M.; Vratil, A. Managed care, professional autonomy, and income: Effects on physician career satisfaction. J. Gen. Intern. Med. 2001, 16, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Peña-Sánchez, J.N.; Lepnurm, R.; Bermedo-Carrasco, S. Latent gender inequalities in the well-being of physicians according to payment method for practicing medicine: A cross-sectional study. J. Hosp. Adm. 2013, 2, 7–14. [Google Scholar] [CrossRef]
- Bodenheimer, T.; Grumbach, K. Understanding Health Policy: A Clinical Approach, 7th ed.; McGraw-Hill: New York, NY, USA, 2016. [Google Scholar]
- Domagała, A.; Bała, M.; Peña-Sánchez, J.N.; Storman, D.; Świerz, M.; Kaczmarczyk, M.; Storman, M. Satisfaction of physicians working in hospitals within the European Union—State of the evidence based on systematic review. Eur. J. Public Health 2018. [Google Scholar] [CrossRef] [PubMed]
- Bala, M.; Domagala, A.; Pena-Sanchez, J.N. Systematic Review of Physicians’ Job Satisfaction Working in European Hospitals, PROSPERO. Available online: http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42016053579 (accessed on 1 October 2018).
- Cook, D.A.; Beckman, T.J. Current Concepts in Validity and Reliability for, Psychometric Instruments: Theory and Application. Am. J. Med. 2006, 119, 166.e7–166.e16. [Google Scholar] [CrossRef] [PubMed]
- Center for Evidence Based Management. Critical Appraisal Checklist for Cross-Sectional Study. July 2014. Available online: http://www.cebma.org/wp-content/uploads/Critical-Appraisal-Questions-for-a-Survey.pdf (accessed on 1 October 2018).
- Aalto, A.M.; Heponiemi, T.; Vaananen, A.; Bergbom, B.; Sinervo, T.; Elovainio, M. Is working in culturally diverse working environment associated with physicians’ work-related well-being? A cross-sectional survey study among Finnish physicians. Health Policy 2014, 117, 187–194. [Google Scholar] [PubMed]
- Bauer, J.; Groneberg, D.A. Distress among physicians in hospitals—An investigation in Baden-Wurttemberg, Germany. Deutsche Medizinische Wochenschrift 2013, 138, 2401–2406. [Google Scholar] [PubMed]
- Van Beuzekom, M.; Akerboom, S.; Boer, F.; Dahan, A. Influence of latent risk factors on job satisfaction, job stress and intention to leave in anaesthesia teams: A cross-sectional survey. Eur. J. Anaesthesiol. 2013, 30, 222–228. [Google Scholar] [CrossRef] [PubMed]
- French, F.; Ikenwilo, D.; Scott, A. What influences the job satisfaction of staff and associate specialist hospital doctors? Health Serv. Manag. Res. 2007, 20, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Gaszynska, E.; Stankiewicz-Rudnicki, M.; Szatko, F.; Wieczorek, A.; Gaszynski, T. Life satisfaction and work-related satisfaction among anesthesiologists in Poland. Sci. World J. 2014, 2014, 601865. [Google Scholar] [CrossRef] [PubMed]
- Heponiemi, T.; Kuusio, H.; Sinervo, T.; Elovainio, M. Job attitudes and well-being among public vs. private physicians: Organizational justice and job control as mediators. Eur. J. Public Health 2010, 21, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Janus, K.; Amelung, V.E.; Baker, L.C.; Gaitanides, M.; Schwartz, F.W.; Rundall, T.G. Job satisfaction and motivation among physicians in academic medical centers: Insights from a cross-national study. J. Health Politics Policy Law 2008, 33, 1133–1167. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, S. Psychosocial work environment and prediction of job satisfaction among Swedish registered nurses and physicians—A follow-up study. Scand. J. Caring Sci. 2012, 26, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Kinzl, J.F.; Knotzer, H.; Traweger, C.; Lederer, W.; Heidegger, T.; Benzer, A. Influence of working conditions on job satisfaction in anaesthetists. Br. J. Anaesth. 2005, 94, 211–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laubach, W.; Fischbeck, S. Job satisfaction and the work situation of physicians: A survey at a German University hospital. Int. J. Public Health 2007, 52, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Mache, S.; Vitzthum, K.; Nienhaus, A.; Klapp, B.F.; Groneberg, D.A. Physicians’ working conditions and job satisfaction: Does hospital ownership in Germany make a difference? BMC Health Serv. Res. 2009, 9, 148. [Google Scholar] [CrossRef] [PubMed]
- Mache, S.; Vitzthum, K.; Klapp, B.F.; Groneberg, D.A. Improving quality of medical treatment and care: Are surgeons’ working conditions and job satisfaction associated to patient satisfaction? Langenbeck’s Arch. Surg./Deutsche Gesellschaft fur Chirurgie 2012, 397, 973–982. [Google Scholar] [CrossRef] [PubMed]
- Mache, S.; Vitzthum, K.; Klapp, B.F.; Danzer, G. Surgeons’ work engagement: Influencing factors and relations to job and life satisfaction. Surgeon J. R. Coll. Surg. Edinb. Irel. 2014, 12, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Mascia, D.; Morandi, F.; Cicchetti, A. Hospital restructuring and physician job satisfaction: An empirical study. Health Policy 2014, 114, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Michinov, E.; Olivier-Chiron, E.; Rusch, E.; Chiron, B. Influence of transactive memory on perceived performance, job satisfaction and identification in anaesthesia teams. Br. J. Anaesth. 2008, 100, 327–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ommen, O.; Driller, E.; Köhler, T.; Kowalski, C.; Ernstmann, N.; Neumann, M.; Steffen, P.; Pfaff, H. The relationship between social capital in hospitals and physician job satisfaction. BMC Health Serv. Res. 2009, 9, 81. [Google Scholar] [CrossRef] [PubMed]
- Peña-Sánchez, J.N.; Lepnurm, R.; Morales-Asencio, J.M.; Delgado, A.; Domagała, A.; Górkiewicz, M. Factors identified with higher levels of career satisfaction of physicians in Andalusia, Spain. Health Psychol. Res. 2014, 2, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Psilopanagioti, A.; Anagnostopoulos, F.; Mourtou, E.; Niakas, D. Emotional intelligence, emotional labor, and job satisfaction among physicians in Greece. BMC Health Serv. Res. 2012, 12, 463. [Google Scholar] [CrossRef] [PubMed]
- Rosta, J.; Nylenna, M.; Aasland, O.G. Job satisfaction among hospital doctors in Norway and Germany. A comparative study on national samples. Scand. J. Public Health 2009, 37, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Schmit Jongbloed, L.J.; Schönrock-Adema, J.; Borleffs, J.C.; Stewart, R.E.; Cohen-Schotanus, J. The influence of achievement before, during and after medical school on physician job satisfaction. Adv. Health Sci. Educ. Theory Pract. 2014, 19, 581–595. [Google Scholar] [CrossRef] [PubMed]
- Stromgren, M.; Eriksson, A.; Bergman, D.; Dellve, L. Social capital among healthcare professionals: A prospective study of its importance for job satisfaction, work engagement and engagement in clinical improvements. Int. J. Nurs. Stud. 2016, 53, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Szilvia, Á.; Zsuzsa, G.; Krisztina, L. High prevalence of job dissatisfaction among female physicians: Work-family confl ict as a potential stressor. Orvosi Hetilap 2009, 150, 1451–1456. [Google Scholar]
- Tartas, M.; Walkiewicz, M.; Majkowicz, M.; Budzinski, W. Psychological factors determining success in a medical career: A 10-year longitudinal study. Med. Teach. 2011, 33, e163–e172. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.R.M.; Smets, E.M.A.; Oort, F.J.; de Haes, H.C.J. Stress, satisfaction and burnout among Dutch medical specialists. CMAJ Can. Med. Assoc. J. 2003, 168, 271–275. [Google Scholar]
- Aiken, L.H.; Sloane, D.M.; Clarke, S.; Poghosyan, L.; Cho, E.; You, L.; Finlayson, M.; Kanai-Pak, M.; Aungsuroch, Y. Importance of work environments on hospital outcomes in nine countries. Int. J. Qual. Health Care 2011, 23, 357–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassalino, L.P.; Crosson, F.J. Physician satisfaction and physician well-being: Should anyone care? Prof. Prof. 2015, 5. [Google Scholar] [CrossRef]
- Kravitz, R.L. Physician job satisfaction as a public health issue. Isr. J. Health Policy Res. 2015, 1, 51. [Google Scholar] [CrossRef] [PubMed]
- European Union. EU Level Collaboration on Forecasting Health Workforce Needs, Workforce Planning and Health Workforce Trends—A Feasibility Study; European Union: Brussels, Belgium, May 2012. [Google Scholar]
- Domagała, A.; Klich, J. Planning of Polish physician workforce—Systemic inconsistencies, challenges and possible ways forward. Health Policy 2018, 122, 102–108. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No | Study ID | Country | Period Years | Target Group/Medical Specialization | Response Rate | Number of Physicians Included in the Analysis | Tools used to Measure Physician Satisfaction |
|---|---|---|---|---|---|---|---|
| 1 | Aalto et al. (2014) [17] | Finland | 2010 | Finnish physicians | 55% | 1916 | Job Diagnostic Survey (JDS) |
| 2 | Bauer and Gronenberg (2013) [18] | Germany | 2012–2013 | Physicians in German hospitals | 18% | 7090 | Job Diagnostic Survey (JDS) |
| 3 | van Beuzekom et al. (2013) [19] | Netherlands | NR | Anaesthetists, trainee anaesthetists and nurse anaesthetists from three university hospitals | 67% 56% | 109 specialists and 46 trainees | Leiden Quality of Work Questionnaire (scale for JS) |
| 4 | French et al. (2007) [20] | United Kingdom | 2001 | Staff and associate specialists (SAS doctors) working in NHS Scotland | 50% 52% | 251 staff grades and 100 for associate specialists | Warr—Cook—Wall Job Satisfaction Scale |
| 5 | Gaszynska et al. (2014) [21] | Poland | 2013 | Senior specialist anaesthetists working within the Lodzkie Voivodship | 77% | 136 | Bovier et al. questionnaire |
| 6 | Heponiemi et al. (2008–2015) [22] | Finland | 2006 | Finnish physicians | 57% | 2652 | Job Diagnostic Survey (JDS) |
| 7 | Janus et al. (2008) [23] | Germany | 2004–2005 | Physicians at the university hospital in Hannover | 46.5% | 390 | Authors’ own questionnaire |
| 8 | Jönsson (2012) [24] | Sweden | 2002–2009 | Physicians and nurses registered in a county council in the south of Sweden (Region Skane) | 65% 45% | In 2002: 499 physicians In 2009: 359 physicians | Questionnaire based on General Nordic Questionnaire (QPS Nordic) for Psychological and Social Factors at Work |
| 9 | Kinz et al. (2005) [25] | Austria | 2003 | Anaesthetists from the University Department of Anaesthesiology and Critical Care Medicine, Innsbruck | 66% | 89 | Olson and Stewart Global Job Satisfaction Scale |
| 10 | Laubach and Fischbeck (2007) [26] | Germany | 2001–2002 | Physicians at the university hospital of Mainz | 42% | 438 | General and specific satisfaction in life developed by Fahrenberg et al. |
| 11 | Mache et al. (2009) [27] | Germany | 2008 | German hospital physicians | 67% | 203 | Copenhagen Psychological Questionnaire (COPSOQ) |
| 12 | Mache et al. (2012) [28] | Germany | 2009–2010 | Patients and surgeons (full-time employed junior doctors or residents specializing in surgery) working in surgery hospital departments in Germany | 65% | 98 | Copenhagen Psychological Questionnaire (COPSOQ) |
| 13 | Mache et al. (2014) [29] | Germany | 2009–2011 | Surgeons in hospital departments for surgery in German hospitals | 63% | 123 | Copenhagen Psychological Questionnaire (COPSOQ) |
| 14 | Mascia et al. (2014) [30] | Italy | 2006– 2009 | Physicians in 18 clinical directorates employed by ten hospitals in the I-NHS | 27% | 336 | Overall Job Satisfaction Scale |
| 15 | Michinov et al. (2008) [31] | France | 2006–2006 | Physician anaesthesiologists and nurse anaesthetists working in an anaesthesia team | 78% | 74 | Minnesota Job Satisfaction Questionnaire |
| 16 | Ommen et al. (2009) [32] | Germany | 2002 | Physicians working in 4 different German hospitals | 61% | 277 | Authors’ own questionnaire |
| 17 | Peña-Sánchez et al. (2014) [33] | Spain | 2009–2010 | Specialist physicians working in hospitals of Andalusia, Spain | 41% | 121 | 4CornerSat Questionnaire developed by Lepnurm |
| 18 | Psilopanagioti et al. (2012) [34] | Greece | 2011 | Physicians working at the University Hospital of Patras | 87% | 130 | Brayfield and Rothe General Index of Job Satisfaction |
| 19 | Rosta and Gerber (2008) [35] | Germany | 2006 | Physicians in German hospitals | 58% | 1890 | Warr—Cook—Wall Job Satisfaction Scale |
| 20 | Schmit Jongbloed et al. (2014) [36] | Netherlands | 2009–2010 | Graduates who started medical training at the University of Groningen in 1982, 1983, 1992 and 1993. | 88% | 523 | Authors’ own questionnaire |
| 21 | Strömgren et al. (2016) [37] | Sweden | 2012 | Physicians in intensive care, emergency, surgical and medical units in 5 hospitals | 53% | 224 | Copenhagen Psychological Questionnaire (COPSOQ) |
| 22 | Szilvia et al. (2009) [38] | Hungary | 2005–2007 | Female Hungarian physicians (male physicians as control group) | 76% | 440 | Authors’ own questionnaire |
| 23 | Tartas et al. (2011) [39] | Poland | Part I: 1999–2005 Part II: 2008–2009 | Medical doctors who graduated from The Medical University of Gdansk | different in subgroup: 87% and 21% | 54 | Authors’ own questionnaire |
| 24 | Visser et al. (2003) [40] | Netherlands | 1998 | Dutch medical specialists | 66% | 1435 | Consultants’ Mental Health Questionnaire |
| Personal Factors | Intrinsic Factors | Contextual Factors | ||
|---|---|---|---|---|
| Workplace Related | Job Related | Other | ||
| Age [18,20,22,28,30,31,32,34,35] Gender [17,18,20,21,22,27,28,31,32,34,35,36] Years of experience/practice [21,27,30,31,36] Marital status or having a partner [20,21] Work-family conflict [22,38] Health status [20,22,26] Life satisfaction [35] Coping strategies/psychological construct [17,25,34,39,40] Being a foreign/internationally trained doctor [33] | Specialty [17,20,22,26] Patients interactions [23,28] Work engagement [29] | Hospital type and structure [22] Management and leadership [19,22,26,27,37,40] Opportunity for professional development [23,27,28,29,40] Colleague support [17,23,24,25,26,27,28,29,31,37,40] Access to resources [19,23] | Workload and job demands [17,22,40] Work control [27,28,29,30] Work stability [22,40] Being a chief [18,30,35] Income and non-financial incentives [20,33,40] | Intention to leave [19] Prior achievement [36] |
| Factors | Statistically Significant | Statistically Non-Significant | |
|---|---|---|---|
| Personal factors | Age | Heponiemi et al. [22] Mascia et al. [30] (under 36) Rosta and Gerber [35] | Bauer and Gronenberg [18] Mache et al. [27] Mascia et al. [30] (for other age groups than under 36) Ommen et al. [32] Michniov et al. [31] Psilopanagioti et al. [34] |
| Gender | Aalto et al. [17] (female) Bauer and Gronenberg [18] (female) Michinov et al. [31] (female) Schmit Jongbloed [36] | Bauer and Gronenberg [18] (male) French et al. [20] Gaszynska et al. [21] Heponiemi et al. [22] Mache et al. [27] Mascia et al. [30] Ommen et al. [32] Psilopanagioti et al. [34] Rosta and Gerber [35] | |
| Years of experience/practice | Mache et al. [28] Mascia et al. [30] Michinov et al. [31] | Gaszynska et al. [21] Schmit Jongbloed et al. [36] | |
| Marital status or having a partner | French et al. [20] Gaszynska et al. [21] | ||
| Work-family conflict | Heponiemi et al. [22] Szilvia et al. [38] | ||
| Health status | French et al. [20] (staff) Heponiemi et al. [22] Laubachand Fischbeck [26] | French et al. [20] (associated specialists) | |
| Life satisfaction | Rosta and Gerber [35] | ||
| Coping strategies/psychological construct | Aalto et al. [17] Kinz et al. [25] Psilopanagioti et al. [34] Tartas et al. [39] Visser et al. [40] | ||
| Being a foreign doctor | Peña-Sánchez et al. [33] | ||
| Intrinsic factors | Specialty | Aalto et al. [17] French et al. [20] Heponiemi et al. [22] | |
| Patients interactions | Janus et al. [23] Mache et al. [28] | ||
| Work engagement | Mache et al. [29] | ||
| Contextual factors | Workplace Related | ||
| Hospital type and structure | Heponiemi et al. [22] | ||
| Management and leadership | van Beuzekom et al. [19] Heponiemi et al. [22] Jönsson [25] Mache et al. [27] Mascia et al. [30] (research, trust and LHA hospitals) Strömgren et al. [37] Visser et al. [40] | Mascia et al. [30] (teaching hospitals) | |
| Opportunity for professional development | Janus et al. [23] Mache et al. [27] Mache et al. [28] Mache et al. [29] Visser et al. [40] | Janus et al. [23] | |
| Colleague support | Aalto et al. [17] Janus et al. [23] Jönsson [24] Kinz et al. [25] Michinov et al. [31] Strömgren et al. [37] Mache et al. [29] Visser et al. [40] | Ommen et al. [32] | |
| Access to resources | van Beuzekom et al. [19] (anesthestists) Janus et al. [23] | van Beuzekom et al. [19] (trainee anesthetists) | |
| Job related | |||
| Workload and job demands | Aalto et al. [17] Heponiemi et al. [22] Visser et al. [40] | ||
| Work control | French et al. [20] Mache e al. [28] (subgroups) | Mache [28] (subgroups) | |
| Work stability | Heponiemi et al. [22] Visser et al. [40] | ||
| Being a chief | Bauer and Gronenber [18] Rosta and Gerber [35] | Mascia et al. [30] | |
| Income and non-financial incentives | French et al. [20] (in one range of income per year) Peña-Sánchez et al. [33] Visser et al. [40] | French et al. [20] (for other income range) | |
| Other | |||
| Intention to leave | van Beuzekom et al. [19] anesthetists | ||
| Prior achievement | Schmit Jongbloed et al. [36] | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domagała, A.; Bała, M.M.; Storman, D.; Peña-Sánchez, J.N.; Świerz, M.J.; Kaczmarczyk, M.; Storman, M. Factors Associated with Satisfaction of Hospital Physicians: A Systematic Review on European Data. Int. J. Environ. Res. Public Health 2018, 15, 2546. https://doi.org/10.3390/ijerph15112546
Domagała A, Bała MM, Storman D, Peña-Sánchez JN, Świerz MJ, Kaczmarczyk M, Storman M. Factors Associated with Satisfaction of Hospital Physicians: A Systematic Review on European Data. International Journal of Environmental Research and Public Health. 2018; 15(11):2546. https://doi.org/10.3390/ijerph15112546
Chicago/Turabian StyleDomagała, Alicja, Małgorzata M. Bała, Dawid Storman, Juan Nicolás Peña-Sánchez, Mateusz J. Świerz, Mateusz Kaczmarczyk, and Monika Storman. 2018. "Factors Associated with Satisfaction of Hospital Physicians: A Systematic Review on European Data" International Journal of Environmental Research and Public Health 15, no. 11: 2546. https://doi.org/10.3390/ijerph15112546
APA StyleDomagała, A., Bała, M. M., Storman, D., Peña-Sánchez, J. N., Świerz, M. J., Kaczmarczyk, M., & Storman, M. (2018). Factors Associated with Satisfaction of Hospital Physicians: A Systematic Review on European Data. International Journal of Environmental Research and Public Health, 15(11), 2546. https://doi.org/10.3390/ijerph15112546