Assessment of Risk, Vulnerability and Adaptation to Climate Change by the Health Sector in Madagascar

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
- -
- Climate and health trends for 12 districts;
- -
- Climate and health projections for six districts;
- -
- Health and socio economic correlation study for six districts;
- -
- Health sector vulnerability assessment for 22 regions.
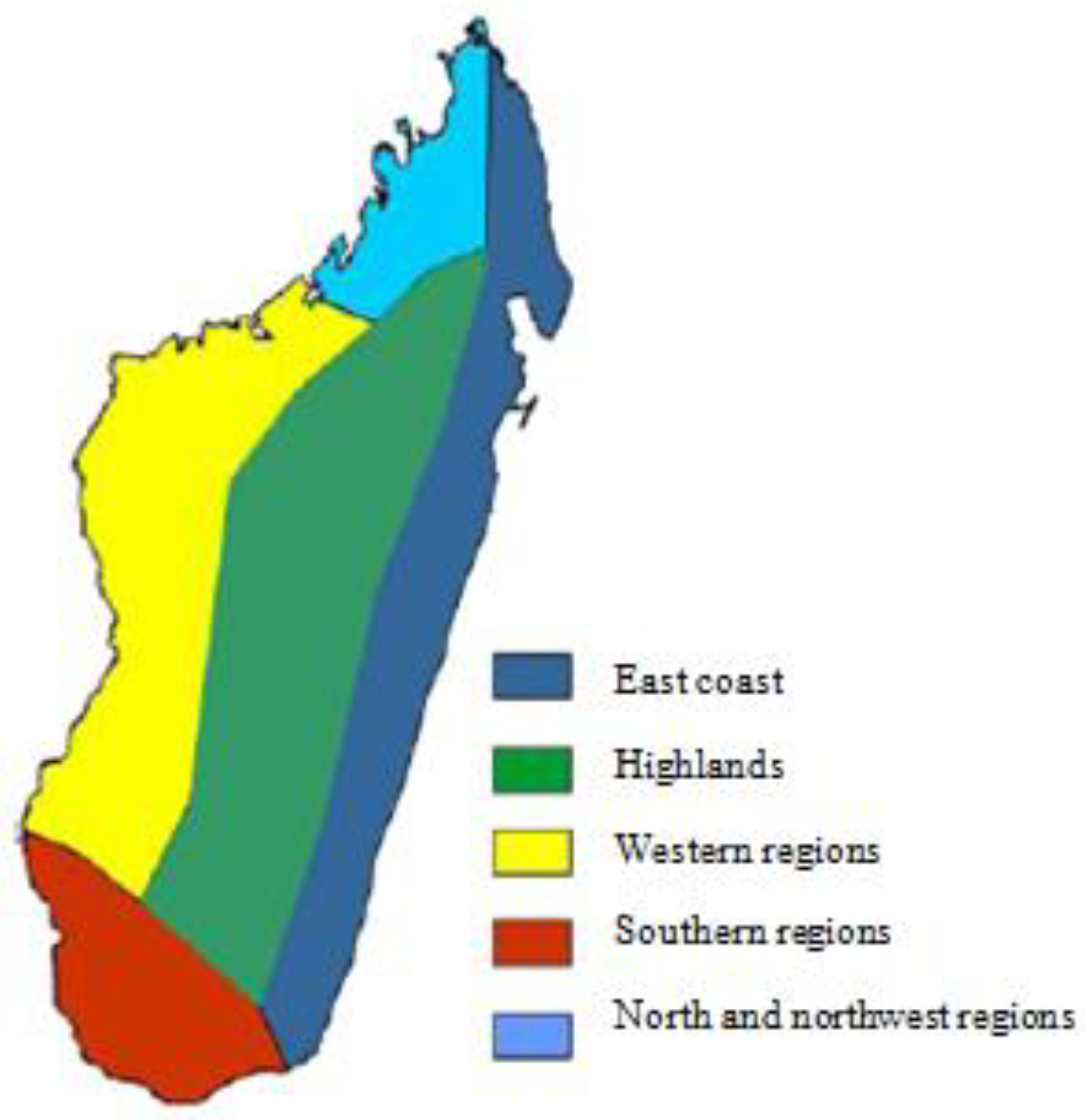
2.2. Madagascar Climate
- -
- The eastern coast has a warm and humid tropical climate;
- -
- The central highland has a high altitude tropical climate;
- -
- The western region has a warm climate and two distinct seasons, a dry winter and a hot and humid summer;
- -
- The north and northwest region has a tropical climate, with the northwest monsoon conditions driving rainfall during the summer season;
- -
- The southern region of the country has a semi-arid climate.
2.3. Climate Hazards and Health Outcomes
- -
- affecting Madagascar;
- -
- generating significant negative socio-economic impacts, particularly on health;
- -
- could be aggravated by climate change.
2.4. Target Regions and Districts
- -
- For the health sector vulnerability study: 22 regions;
- -
- For the study of climate and health trends: 12 districts (Antananarivo, Manjakandriana, Antsiranana, Nosy Be, Morondava, Belo on Tsiribihina, Mahabo, Toliara I, Morombe, Farafangana, Vangaindrano, Vohipeno) (Figure 2);
- -
- For the study of climate projections and the study of current and future climate change and health burdens: six localities (Antsiranana, Nosy Be, Antananarivo, Morondava, Farafangana, Morombe). These six localities were also used for the correlations study between climate-sensitive diseases and climate and socio-economic indicators.
2.5. Data Sources
2.5.1. Weather and Climate Data
2.5.2. Epidemiological Data
2.5.3. Socio-Economic Data
2.6. Statistical Methods
2.7. Limits of the Study
3. Results
3.1. Climate Trends and Projections in the Target Districts
3.1.1. Climate Trends in the 12 Target Districts
3.1.2. Climate Projections for the 6 Target Districts
3.2. Trends and Projections of Health Parameters
3.2.1. Observed Health Trends
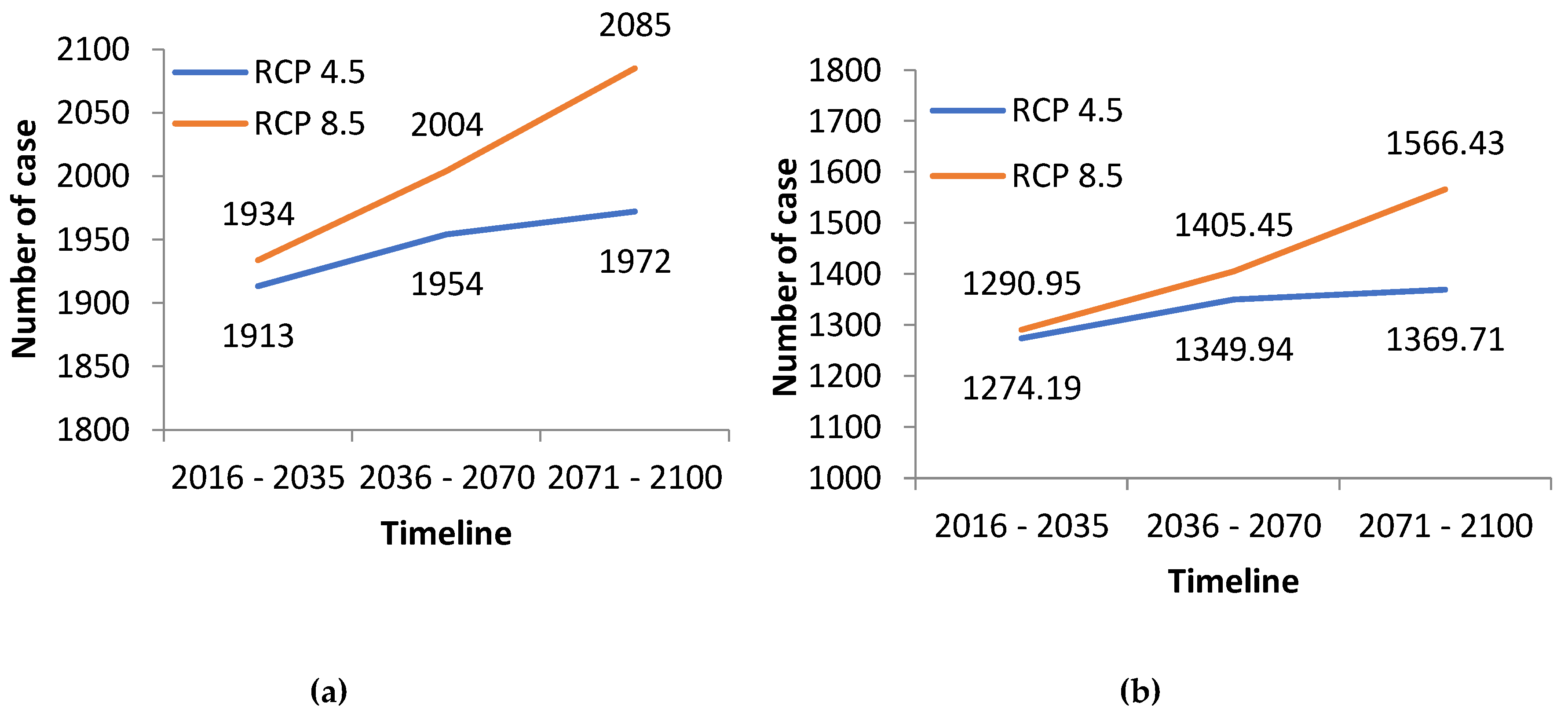
3.2.2. Health Projected Trends
3.3. Correlations between Main Socioeconomic Factors and Climate Determinants for Cases of Climate-Sensitive Pathologies
3.4. Health Sector Vulnerability Mapping
3.5. Adaptation Options for the Health Sector
- (1)
- Integrate climate risk management into health system activities, particularly in program and strategic areas of public health:
- -
- Early warning systems for climate and health and;
- -
- Building health system adaptive capacity (including disaster response capacity)
- (2)
- Strengthen community resilience:
- -
- Create a common vision on how to reduce the health risks from climate change;
- -
- Integrate adaptation measures into development plans at all levels: region, district, commune, fokontany;
- (3)
- Mobilize local actors to:
- -
- Strengthen community solidarity;
- -
- Support local development;
- -
- Improve climate change risk management sensitization;
- (4)
- Reduce the vulnerability of households by:
- -
- Improving the standard of living across the population;
- -
- Diversifying income sources;
- -
- Improving living conditions such as habitats, access to basic social services, food security, social protection and security.
4. Discussion
5. Conclusions
- -
- The population of Madagascar and the health sector are already very vulnerable to the risks of current climate variability as evidenced by observations of current health impacts;
- -
- Climate change is expected to increase risks to health and well-being in the future.
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bouley, T.; Midgley, A.; Shumake-Guillemot, J.; Golden, C.D.W.; Ebi, K.L. Madagascar Climate change and health diagnostic: Risks and opportunities for climate-smart health and nutrition investment (English). Available online: http://documents.worldbank.org/curated/en/936661516004441146/Madagascar-Climate-change-and-health-diagnostic-risks-and-opportunities-for-climate-smarthealth-and-nutrition-investment (accessed on 1 July 2018).
- World Bank. Opportunities and Challenges for Inclusive and Resilient Growth: Compendium of Policy Notes for Madagascar. Available online: http://documents.worldbank.org/curated/en/130911468086644653/Opportunites-et-defis-pour-une-croissance-inclusive-et-resiliente-recueil-de-notes-de-politique-pour-Madagascar (accessed on 1 November 2015).
- National Bureau of Catastrophic Risk Management and United Nations Development Programme (BNGRC et PNUD). Plan de relèvement et de résilience pour les districts les plus affectés par la sécheresse déclenchée par El Niño dans le Grand Sud de Madagascar. Available online: http://www.mg.undp.org/content/madagascar/fr/home/library/crisis_prevention_and_recovery/publication_1.html (accessed on 1 November 2015).
- Ratsimamanga, A.; Bettencourt, S. La Gestion des Risques Naturels à Madagascar. Personal Communication. Available online: https://slideplayer.fr/slide/5486905/ (accessed on 1 November 2015).
- McMichael, A.J.; Campbell-Lendrum, D.H.; Corvalán, C.F.; Ebi, K.L.; Githeko, A.; Scheraga, J.D.; Woodward, A. Climate Change and Human Health-Risks and Responses. Available online: https://books.google.mg/books?id=tQFYJjDEwhIC&printsec=frontcover&dq=Climate+change+and+human+health+-+risks+and+responses;&hl=fr&sa=X&ved=0ahUKEwiptaeh0OreAhVKKsAKHWu0CJYQ6AEIJzAA#v=onepage&q=Climate%20change%20and%20human%20health%20-%20risks%20and%20responses%3B&f=false (accessed on 1 November 2015).
- Government of Madagascar. Evaluation de la Vulnérabilité et de L’adaptation du Secteur Santé au Changement climatique à Madagascar. Unpublished work. 2015. [Google Scholar]
- World Health Organization. Protecting Health from Climate Change: Vulnerability and Adaptation Assessment. Available online: http://www.who.int/globalchange/publications/vulnerability-adaptation/en/ (accessed on 1 November 2015).
- Donque, G. Contribution Géographique à L’étude du Climat de Madagascar. Ph.D. Thesis, University of Antananarivo, Antananarivo, Madagascar, 1975. [Google Scholar]
- Griffiths, J.F.; Ranaivoson, R. World Survey of Climatology, Vol.10, Climates of Africa; Elsevier: Amsterdam, The Netherlands, 1972; pp. 461–500. [Google Scholar]
- Williams, J.B. Some Temporal and Regional Variations of Climate in Madagascar; Report no. 144; ODNRI, Chatham: London, UK, 1990. [Google Scholar]
- National Bureau of Catastrophic Risk Management (BNGRC). Plan de Contingence National 2010-2011: Cyclones et Inondation. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/F4075FC9B5EF07778525783A00567EBE-Rapport_complet.pdf (accessed on 1 July 2015).
- Institut National de la Statistique (INSTAT); ICF Macro. Enquête Démographique et de Santé de Madagascar 2008–2009. Available online: https://www.dhsprogram.com/pubs/pdf/FR236/FR236.pdf (accessed on 1 August 2015).
- Rakotomavo, Z.A.P.H.; Rajaonarivony, R. Les Tendances Observées et les Futurs Changements Climatiques à Madagascar. Rapport Technique Interne Direction des Recherches et Développement/Direction Générale de la Météorologie, Antananarivo, Madagascar. Unpublished work. 2015. [Google Scholar]
- Ministry of Public Helath; World Health Organization. National Health Adaptation Plan, Antananarivo, Madagascar. Unpublished work. 2014.
- World Health Organization/United Nations Framework Convention on Climate Change. Climate and Health Country Profile: Madagascar. Available online: http://apps.who.int/iris/bitstream/handle/10665/246140/WHO-FWC-PHE-EPE-15.40-eng.pdf;jsessionid=B8376C8A12D5A12D8CBB47DBA9E754A5?sequence=1 (accessed on 1 November 2015).
- Barros, V.R.; Field, C.B.; Dokken, D.J.; Mastrandrea, M.D.; Mach, K.J.; Bilir, T.E.; Chatterjee, M.; Ebi, K.L.; Estrada, Y.O.; Genova, R.C.; et al. Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part B: Regional Aspects. Contribution of Working group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014; p. 688. [Google Scholar]
- Githeko, A.K.; Lindsay, S.W.; Confalonieri, U.E.; Patz, J.A. Changement climatique et maladies à transmission vectorielle : Une analyse régionale. Bull. World Health Organ. 2000, 78, 1136–1147. (In French) [Google Scholar] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category of Vulnerability | Vulnerability Factor |
|---|---|
| Economic vulnerability | Low income Livelihood dependent on natural resources |
| Social vulnerability | High child malnutrition Area prone to communicable diseases Low accessibility to health infrastructure Limited access to water and sanitation Low literacy |
| Environmental vulnerability | Precarious housing Hazardous area Remoteness |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rakotoarison, N.; Raholijao, N.; Razafindramavo, L.M.; Rakotomavo, Z.A.P.H.; Rakotoarisoa, A.; Guillemot, J.S.; Randriamialisoa, Z.J.; Mafilaza, V.; Ramiandrisoa, V.A.M.P.; Rajaonarivony, R.; et al. Assessment of Risk, Vulnerability and Adaptation to Climate Change by the Health Sector in Madagascar. Int. J. Environ. Res. Public Health 2018, 15, 2643. https://doi.org/10.3390/ijerph15122643
Rakotoarison N, Raholijao N, Razafindramavo LM, Rakotomavo ZAPH, Rakotoarisoa A, Guillemot JS, Randriamialisoa ZJ, Mafilaza V, Ramiandrisoa VAMP, Rajaonarivony R, et al. Assessment of Risk, Vulnerability and Adaptation to Climate Change by the Health Sector in Madagascar. International Journal of Environmental Research and Public Health. 2018; 15(12):2643. https://doi.org/10.3390/ijerph15122643
Chicago/Turabian StyleRakotoarison, Norohasina, Nirivololona Raholijao, Lalao Madeleine Razafindramavo, Zo Andrianina Patrick Herintiana Rakotomavo, Alain Rakotoarisoa, Joy Shumake Guillemot, Zazaravaka Jacques Randriamialisoa, Victor Mafilaza, Voahanginirina Anne Marie Pierrette Ramiandrisoa, Rhino Rajaonarivony, and et al. 2018. "Assessment of Risk, Vulnerability and Adaptation to Climate Change by the Health Sector in Madagascar" International Journal of Environmental Research and Public Health 15, no. 12: 2643. https://doi.org/10.3390/ijerph15122643
APA StyleRakotoarison, N., Raholijao, N., Razafindramavo, L. M., Rakotomavo, Z. A. P. H., Rakotoarisoa, A., Guillemot, J. S., Randriamialisoa, Z. J., Mafilaza, V., Ramiandrisoa, V. A. M. P., Rajaonarivony, R., Andrianjafinirina, S., Tata, V., Vololoniaina, M. C., Rakotomanana, F., & Raminosoa, V. M. (2018). Assessment of Risk, Vulnerability and Adaptation to Climate Change by the Health Sector in Madagascar. International Journal of Environmental Research and Public Health, 15(12), 2643. https://doi.org/10.3390/ijerph15122643