1. Introduction
Understanding risk factors is key to preventing and controlling the development of chronic kidney disease (CKD). The known risk factors for developing CKD can be put into four categories. First, demographic conditions. People at risk are, for example, female [
1], over 75 years old [
2], non-Hispanic blacks [
3], receiving only primary education or no education [
4,
5], and having a family history of chronic renal diseases [
6]. Second, comorbidities include diabetes [
1,
7], hypertension [
1,
8], metabolic syndrome [
9], heart failure [
10], hepatitis B [
11], hepatitis C [
12], glomerulonephritis [
13], hyperuricemia [
14], hyperlipidemia [
1], anemia [
15], and systemic lupus erythematosus [
16]. Third, lifestyles, including smoking for more than five pack-years [
17], drinking alcohol heavily with 30 g/day [
18], betel nut chewing [
19], exercising lightly with <30 min of bicycling per day or an equal amount of activities [
20], and having a low water intake of <2.0 L/day [
21]. The last category is environmental and physiological conditions, including having cadmium in one’s blood and/or urine [
22], lead in the blood [
23], and organophosphorus herbicides in water [
24]. A recent study even suggested that dehydration resulted from climate change may also be a risk factor for developing CKD [
25]. Among all of these factors, diabetes and hypertension are highly recognized to associated with CKD [
8,
26].
Taiwan, infamous for the highest prevalence rate of end-stage renal disease (ESRD) in the world [
27,
28], has suffered the prevalence of CKD. CKD is also a global health problem. Approximately 13.4% of the world’s population has CKD [
29]. The CKD prevalence rate in Taiwan was approximately 11.9%, estimated by a large-scale study of 462,293 Taiwanese adults in 2006 [
27]. In other words, approximately 2.03 million Taiwanese people had CKD [
27]. CKD, which can be divided into five stages of increasing severity, is becoming an increasingly serious health problem worldwide. Until 2015, Taiwan had the highest prevalence of ESRD in the world (3317 cases per million people) [
28]. A total of 77,920 Taiwanese patients received an ESRD diagnosis in 2015 [
28]. ESRD is not only life-threatening and inconvenient for patients’ daily living, but also a burden on the society’s medical resources. Therefore, the early diagnosis and prevention of CKD are critical objectives in maintaining a healthy public.
Unprocessed raw water can affect one’s health. Not only can unprocessed water be a source of drinking water, but it can also influence agricultural soils, plants, and animals, subsequently affecting our health. In Taiwan, three categories of water resources (reservoirs, rivers, and groundwater) dominate the sources of drinking water. About three-fourths drinking water is tap water [
30]. More than half of tap water comes from reservoirs, about one third from surface water like rivers, and about ten percent from groundwater [
31]. Raw water before drinking undergoes a series of water treatment processes, which involve physical, chemical, and biological processes in order to remove contaminants such as pesticides, organic pollutants, and volatile organics. Yet, the remaining contaminants may still be delivered into human bodies.
Although water is essential for kidney function, a full-scale investigation into the environment’s exposure to water contaminants in the development of CKD/ERSD has yet to be conducted in Taiwan in order to identify any potential water-related risk factors for CKD/ESRD. This study aimed to investigate the associations between the 61 water attributes of the three water resources and the CKD/ESRD prevalence rates in Taiwan from 2005 to 2011. To our knowledge, this is the first study to assess the relationships between CKD/ESRD and a wide range of water properties in the environment.
4. Discussion
To our knowledge, this is the first ecological study with seven years of monitoring to associate the CKD and ESRD prevalence rates with a wide range of water attributes of the environment. We found that Zn, ammonia, COD, and DO of rivers were weakly correlated with the CKD prevalence rates, but none of them were linked to ESRD under the stringent Bonferroni–Holm test.
The GAM with the Zn and COD of rivers was the best model for the given data (
Table 4). Although including additional NH
3 or omitting COD in the model led to a similar AIC performance when compared to the best model, the results did not support the inclusion of one more parameter (NH
3). However, the necessity of the inclusion of COD in the model was unclear. The differences in AIC did not support the notion that the Zn only model was substantially inferior to the best model.
Zn in the environment has been linked to CKD. In fact, both our correlation and regression results supported that Zn was a relatively stronger indicator of CKD prevalence than the three other river attributes. A recent study that indicated that Zn in residential soil was a risk factor for CKD progression also supports our findings [
45]. We suspect that a Zn contaminated river, which can pollute soil, may reach CKD patients in the same way that Zn contaminated soil does. On the other hand, Zn homeostasis is important for kidney function. A Zn deficiency is present in CKD patients [
46]. Although oxidized Zn particles which interfere with Zn homeostasis in rats are toxic [
47], further investigations are needed to confirm whether exposure to environmental Zn could cause the development of CKD in humans.
To our knowledge, this is also the first report to link environmental water quality indicators to CKD in humans. Ammonia, COD, and DO all are indicative measures of water quality. They are interrelated in some way. For example, ammonia can acidify water, consume oxygen, and raise the COD. Ammonia can be a key indicator to determine whether water resources are undergoing anthropogenic pollution. Excessive anthropogenic pollutants—which mainly come from unprocessed livestock wastewater, domestic sewage, and industrial manufacturing—are enriched with ammonia. Elevated levels of ammonia in the water have been demonstrated to degenerate the kidneys of Nile tilapia [
48]. However, further studies are needed to verify its role in humans.
Like a high level of ammonia in water, a low DO may mean a poor water quality. A low DO may be caused by overfertilization, causing water plants to overgrow and dead plants to draw a lot of bacteria, which, in turn, depletes the DO level. A river with a lower DO can support less aquatic organisms, implying that the environment’s water is more toxic. A region with a lower DO may mean that its environment is more toxic, thus linking it to CKD patients. Besides, hypoxia, a condition defined by the body being deprived of oxygen, is known to accelerate CKD progression [
49]. An adequate oxygen supply is important for the functioning of the kidneys. However, it is unclear whether oxygen-deprived water would reduce the oxygen levels in the kidneys.
A high COD, which indicates more oxidizable pollutants, also suggest that the environment is more toxic in our findings. However, there is a lack of direct evidence that a high COD in water would lead to the development of CKD.
Our results linked arsenic in groundwater to higher CKD prevalence. In fact, the relationship between arsenic and CKD has been extensively studied. Previous animal research on mice and dogs confirmed that exposure to arsenic may damage kidney function [
50,
51]. A recent systematic review of studies on exposure to arsenic and kidney disease mortality in humans over the past 30 years found evidence that generally supported a positive association between the arsenic and CKD [
52]. Our study strengthens their finding through the prevalence rate of kidney disease, not the mortality rate, suggesting that exposure to arsenic in groundwater may relate to the development of CKD/ESRD in Taiwan.
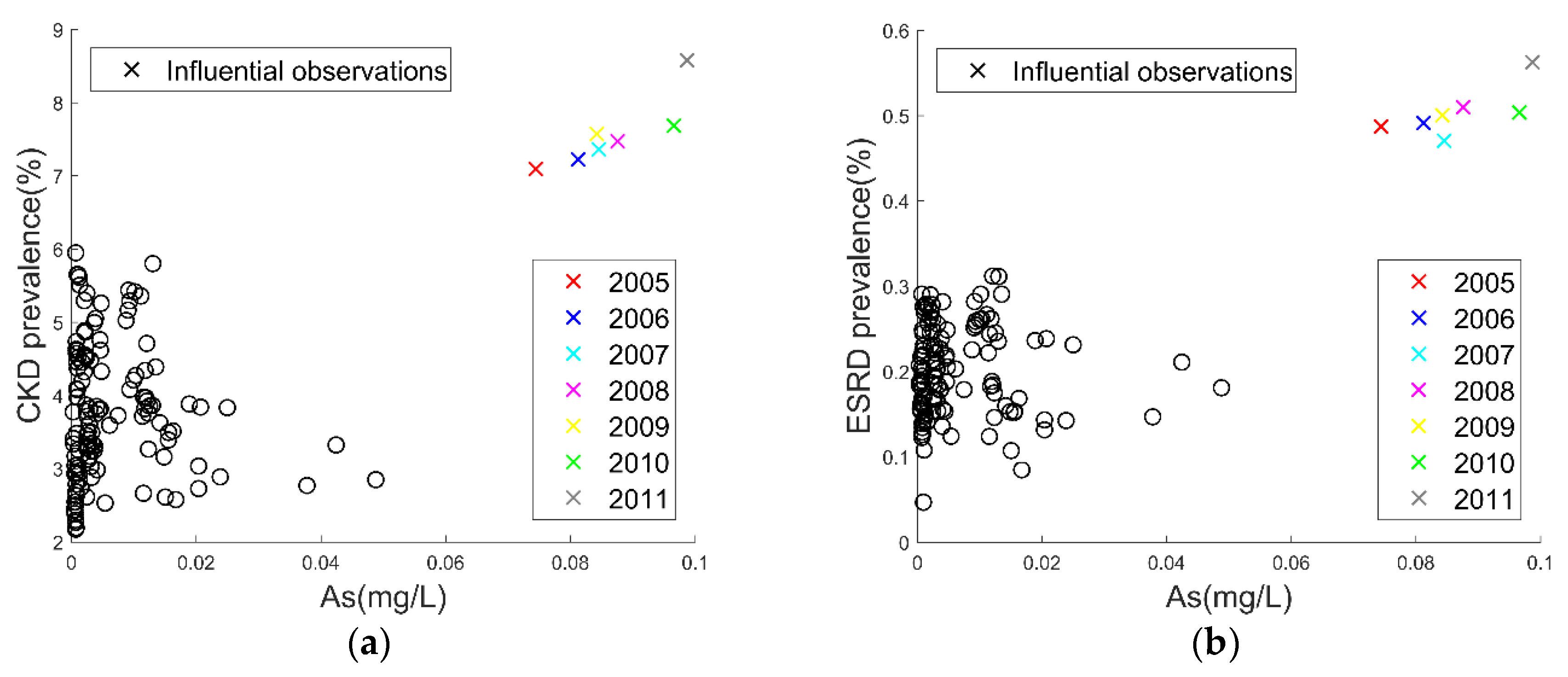
The alarmingly high arsenic concentration in groundwater concurrent with the high prevalence rate of CKD/ESRD in Chiayi city might be the best example to demonstrate a plausible link between exposure to arsenic and CKD/ESRD. Low-dose arsenic levels did not exhibit a clear correlation, suggesting that arsenic in groundwater may need to pass a certain threshold to be associated with CKD/ESRD. Because arsenic exists in the natural environment, such as in the soil, air, water, and food, it may enter human bodies through breathing, drinking, or eating. Chiayi is infamous for its 1950s Blackfoot disease endemic [
53], which resulted from the exposure to arsenic in drinking water from artesian wells, consequently impairing the blood vessels of the lower limbs of patients and causing them to develop gangrene. Based on the 1962 groundwater data, two ecological studies linked arsenic to the increased mortality of kidney disease in Chiayi [
54,
55]. They also indicated the exposure to arsenic in locals had since ceased [
54,
55]. Instead, we used contemporary water monitoring data to associate arsenic with the prevalence of kidney disease. The results led us to speculate the possible long latent effects of arsenic or the recurrent arsenic contamination in Chiayi in its drinking water, crops, or farmed seafood. A recent study reported that arsenic in drinking water in Taiwan was linked to the progression of CKD [
56]. However, further investigations are needed to verify our speculation.
Because this was a longitudinal study, patients enrolled in this ecological population-based study were aging. Some died and the population declined each year. The mean age of our patients may be older than the national estimate because only those older than 18 years were included in our analysis. Younger patients were excluded from the study to avoid possible confounding effects in renal diseases that are genetic disorders. However, the aging and shrinking populations should not affect our results as the age factor was controlled and the prevalence rates were applied in our analyses.
The reason why CKD and ESRD did not share the same correlation magnitude with water attributes may either be due to random fluctuations or may involve a complex progression of kidney disease. To determine the reason, more information is required.
Limitations and Strengths
This study has some limitations. First, this is an observational study at the city or county level so we cannot account for cases smaller than a city or county (e.g., a town or village). Second, although we already adjusted for the gender, age, and annual effects, we still cannot eliminate the possibility that the associations may result from other confounding factors that we did not adjust for. Third, we did not have direct quality measures of drinking water. We instead examined three related water resources. Thus, oral exposure may not necessarily be the same as the environmental exposure studied here. Fourth, unlike incidence cases, prevalence may not capture the full risks of abruptly developing diseases. However, to manifest a renal disease, a long-term exposure may be needed. The exact date at which the exposure started is unknown and to follow up from the first exposure is unfeasible due to the burden of the disease [
57,
58]. We thus preferred using prevalence data instead of incident cases to measure the burden of the disease during a seven-year time lapse in the Taiwanese population in this ecological study.
However, the use of nationwide health data; the extensive coverage of inorganic, physicochemical, and biological properties of water quality data; and computational analyses adjusted for important covariates, have strengthened the conjecture of this study. Although unmeasured confounders may be still present, we adjusted our data to all the possible covariates whose data were available to us. Needless to say, environmental raw water is important not only because it can be a source of drinking water but also because it is connected to our health through the food chain via agriculture and animals. Although the three water resources were only an approximate to drinking water, they—representing the majority of drinking water sources in Taiwan—were the best ones with a massive amount of information available for this study. Overall, we examined a total of 45,846 water-monitoring observations between 2005 and 2011 to address the issue of the temporality of association. Consequently, the monitored water attributes were found to correlate with the national cohort of patients since 2005 and to 2011 in the development of CKD or ESRD. The seven years of data should be reliable enough to establish meaningful associations in a clinical setting.
In fact, this study has several implications. First, the poor water quality in the environment may be linked to renal disease. Second, regulatory water monitoring of these suspicious contaminants should be strictly done from a public health perspective. Third, water with highly suspicious contaminants should be re-treated or drunk with caution. Fourth, water quality management could be imperative for current public health policymaking. Finally, further clinical trials should be warranted to assure the exact roles of the implicated environmental contaminants, such as Zn in rivers, in renal disease mechanisms.

 ,
, 


{kind=link}
{kind=link}

