The Comorbidity of Gambling Disorder among Macao Adult Residents and the Moderating Role of Resilience and Life Purpose


 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Respondents and Procedures
2.2. Measures Section
2.3. Data Analysis
3. Results Section
3.1. Profiles of this Sample
3.2. Comorbidity Analysis
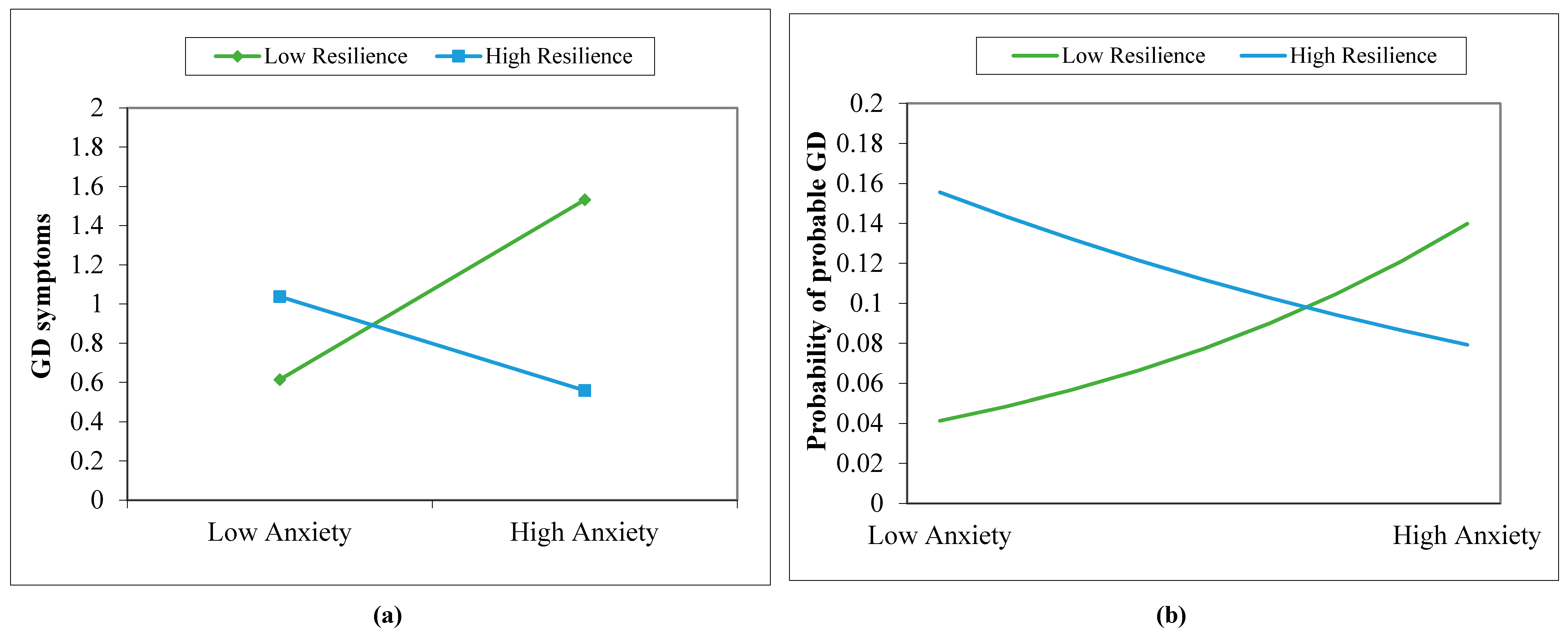
3.3. Exploring Buffering Effects of Psychological Resilience and Purpose in Life
4. Discussion Section
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chan, P.K.; Chan, P.C. Gaming Industry and its Opportunities for Development; Keng Vai: Macao, China, 2001. [Google Scholar]
- Wu AM, S.; Lau JT, F. Gambling in China: Socio-historical evolution and current challenges. Addiction 2015, 110, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Institute for the Study of Commercial Gaming (ISCG). Report on a Study of Macao People’s Participation in Gambling Activities 2007; ISCG: Taipa, Macao, China, 2008. [Google Scholar]
- Institute for the Study of Commercial Gaming (ISCG). Report on a Study of Macao People’s Participation in Gambling Activities 2010; ISCG: Taipa, Macao, China, 2010. [Google Scholar]
- Institute for the Study of Commercial Gaming (ISCG). Report on a Study of Macao People’s Participation in Gambling Activities 2013; ISCG: Taipa, Macao, China, 2014. [Google Scholar]
- Institute for the Study of Commercial Gaming (ISCG). Report on a Study of Macao People’s Participation in Gambling Activities 2016; ISCG: Taipa, Macao, China, 2016. [Google Scholar]
- Fong, D.K.-C.; Ozorio, B. Gambling participation and prevalence estimates of pathological gambling in a far-east gambling city: Macao. UNLV Gaming Res. Rev. J. 2005, 9, 15–28. [Google Scholar]
- Wu, A.M.S.; Lai, M.H.C.; Tong, K.K. Gambling disorder: Estimated prevalence rates and risk factors in Macao. Psychol. Addict. Behav. 2014, 28, 1190–1197. [Google Scholar] [CrossRef] [PubMed]
- National Council on Problem Gambling (NCPG). Report of Survey on Participation in Gambling Activities among Singapore Residents 2017; NCPG: Singapore, 2018; Available online: https://www.ncpg.org.sg/en/pdf/Report_on_NCPG_Gambling_Participation_Survey_2017_final.pdf (accessed on 5 December 2018).
- Kessler, R.C.; Hwang, I.; LaBrie, R.; Petukhova, M.; Sampson, N.A.; Winters, K.C.; Shaffer, H.J. DSM-IV pathological gambling in the National Comorbidity Survey Replication. Psychol. Med. 2008, 38, 1351–1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boughton, R.; Falenchuk, O. Vulnerability and comorbidity factors of female problem gambling. J. Gambl. Stud. 2007, 23, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Cunningham-Williams, R.M.; Cottler, L.B.; Compton WM, I.I.I.; Spitznagel, E.L. Taking chances: Problem gamblers and mental health disorders-results from the St. Louis Epidemiologic Catchment Area Study. Am. J. Public Health 1998, 88, 1093–1096. [Google Scholar] [CrossRef] [PubMed]
- El-Guebaly, N.; Patten, S.B.; Currie, S.; Williams, J.V.A.; Beck, C.A.; Maxwell, C.J.; Wang, J.L. Epidemiological associations between gambling behavior, substance use & mood and anxiety disorders. J. Gambl. Stud. 2006, 22, 275–287. [Google Scholar] [CrossRef]
- Lorains, F.K.; Cowlishaw, S.; Thomas, S.A. Prevalence of comorbid disorders in problem and pathological gambling: Systematic review and meta-analysis of population surveys. Addiction 2011, 106, 490–498. [Google Scholar] [CrossRef]
- Parhami, I.; Siani, A.; Rosenthal, R.J.; Lin, S.; Collard, M.; Fong, T.W. Sleep and gambling severity in a community sample of gamblers. J. Addict. Dis. 2012, 31, 67–79. [Google Scholar] [CrossRef]
- Pompili, M.; Innamorati, M.; Forte, A.; Longo, L.; Mazzetta, C.; Erbuto, D.; Ricci, F.; Palermo, M.; Stefani, H.; Seretti, M.E.; et al. Insomnia as a predictor of high-lethality suicide attempts. Int. J. Clin. Pract. 2013, 67, 1311–1316. [Google Scholar] [CrossRef]
- Taylor, D.J.; Lichstein, K.L.; Durrence, H.H. Insomnia as a health risk factor. Behav. Sleep Med. 2003, 1, 227–247. [Google Scholar] [CrossRef] [PubMed]
- King, D.L.; Delfabbro, P.H. Internet Gaming Disorder: Theory, Assessment, Treatment, and Prevention; Academic Press: Cambridge, MA, USA, 2018. [Google Scholar]
- Griffiths, M.D. Amusement machine playing in childhood and adolescence: A comparative analysis of video games and fruit machines. J. Adolesc. 1991, 14, 53–73. [Google Scholar] [CrossRef]
- Parker, J.D.A.; Taylor, R.N.; Eastabrook, J.M.; Schell, S.L.; Wood, L.M. Problem gambling in adolescence: Relationships with internet misuse, gaming abuse and emotional intelligence. Pers. Indiv. Differ. 2008, 45, 174–180. [Google Scholar] [CrossRef]
- Walther, B.; Morgenstern, M.; Hanewinkel, R. Co-occurrence of addictive behaviours: Personality factors related to substance use, gambling and computer gaming. Eur. Addict. Res. 2012, 18, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Murcia, S.; Fernandez-Aranda, F.; Granero, R.; Choliz, M.; La Verde, M.; Aguglia, E.; Signorelli, M.S.; Sa, G.M.; Aymami, N.; Gomez-Pena, M.; et al. Video Game Addiction in Gambling Disorder: Clinical, Psychopathological, and Personality Correlates. Biomed. Res. Int. 2014, 315062. [Google Scholar] [CrossRef] [PubMed]
- Dowling, N.A.; Brown, M. Commonalities in the psychological factors associated with problem gambling and Internet dependence. Cyberpsychol. Behav. Soc. Netw. 2010, 13, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Oei, T.P.; Goh, Z. Interactions Between Risk and Protective Factors on Problem Gambling in Asia. J. Gambl. Stud. 2015, 31, 557–572. [Google Scholar] [CrossRef]
- Lussier, I.; Derevensky, J.L.; Gupta, R.; Bergevin, T.; Ellenbogen, S. Youth gambling behaviors: An examination of the role of resilience. Psychol. Addict. Behav. 2007, 21, 165–173. [Google Scholar] [CrossRef]
- Fumaz, C.R.; Ayestaran, A.; Perez-Alvarez, N.; Munoz-Moreno, J.A.; Molto, J.; Ferrer, M.J.; Clotet, B. Resilience, ageing, and quality of life in long-term diagnosed HIV-infected patients. AIDS Care 2015, 27, 1396–1403. [Google Scholar] [CrossRef]
- Holdsworth, L.; Nuske, E.; Hing, N.A. Grounded Theory of the Influence of Significant Life Events, Psychological co-Morbidities and Related Social Factors on Gambling Involvement. Int J. Ment. Health Addiction 2015, 13, 257–273. [Google Scholar] [CrossRef]
- Wu, A.M.S.; Lei, L.L.M.; Ku, L. Psychological needs, purpose in life, and problem video game playing among Chinese young adults. Int. J. Psychol. 2013, 48, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Mei, S.; Li, L.; Chai, J.; Li, J.; Du, H. The relationship between impulsivity and internet addiction in Chinese college students: A moderated mediation analysis of meaning in life and self-esteem. PLoS ONE 2015, 10, e0131597. [Google Scholar] [CrossRef] [PubMed]
- Thege, B.K.; Bachner, Y.G.; Kushnir, T.; Kopp, M.S. Relationship between meaning in life and smoking status: Results of a national representative survey. Addict. Behav. 2009, 34, 117–120. [Google Scholar] [CrossRef] [PubMed]
- American Association for Public Opinion Research (AAPOR). Standard Definitions: Final Dispositions of Case Codes and Outcome Rates for Surveys, 9th ed.; AAPOR: Oakbrook Terrace, IL, USA, 2016; Available online: http://www.aapor.org/AAPOR_Main/media/publications/Standard-Definitions20169theditionfinal.pdf (accessed on 5 December 2018).
- Macao Statistics and Census Services. Detailed Results of 2016 Population By-Census. Macao: Macao Statistics and Census Services; DSEC: Macao, China, 2017. [Google Scholar]
- Wu AM, S.; Chen, J.H.; Tong, K.K.; Yu, S.; Lau JT, F. Prevalence and associated factors of Internet gaming disorder among community dwelling adults in Macao, China. J. Behav. Addict. 2018, 7, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.M.S.; Tang, C.S. Problem gambling of Chinese college students: Application of the theory of planned behavior. J. Gambl. Stud. 2012, 28, 315–324. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Moussa, M.T.; Lovibond, P.F.; Laube, R. Psychometric properties of a Chinese version of the short Depression Anxiety Stress Scales (DASS21). In Report for New South Wales Transcultural Mental Health Centre; Cumberland Hospital: Sydney, Australia, 2001; Available online: http://www2.psy.unsw.edu.au/dass/Chinese/Chinese%20DASS21%20Paper.pdf (accessed on 5 December 2018).
- Carter, F.A.; Bell, C.J.; Ali, A.N.; McKenzie, J.; Wilkinson, T.J. The impact of major earthquakes on the psychological functioning of medical students: A Christchurch, New Zealand study. Med. J. 2014, 127, 54–66. [Google Scholar]
- Kulsoom, B.; Afsar, N.A. Stress, anxiety, and depression among medical students in a multiethnic setting. Neuropsych. Dis. Treat. 2015, 11, 1713–1722. [Google Scholar] [CrossRef]
- Wu, L.; Tan, Y.; Liu, Y. Factor structure and psychometric evaluation of the Connor-Davidson resilience scale in a new employee population of China. BMC Psychiatry 2017, 17, 49. [Google Scholar] [CrossRef]
- Ko, C.-H.; Yen, J.-Y.; Chen, S.-H.; Wang, P.-W.; Chen, C.-S.; Yen, C.-F. Evaluation of the diagnostic criteria of Internet gaming disorder in the DSM-5 among young adults in Taiwan. J. Psychiar. Res. 2014, 53, 103–110. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Wang, L.; Shi, Z.; Zhang, Y.; Zhang, Z. Psychometric properties of the 10-item Connor–Davidson Resilience Scale in Chinese earthquake victims. Psychiatry Clin. Neurosci. 2010, 64, 499–504. [Google Scholar] [CrossRef] [PubMed]
- McKenna KY, A.; West, K.J. Give me that online-time religion: The role of the internet in spiritual life. Comput. Hum. Behav. 2007, 23, 942–954. [Google Scholar] [CrossRef]
- Crumbaugh, J.C.; Maholick, L.T. An Experimental Study in Existentialism: The Psychometric Approach to Frankl’s Concept of Noogenic Neurosis. J. Clin. Psychol. 1964, 20, 200–207. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows 25.0; IBM Corp: Armonk, NY, USA, 2017. [Google Scholar]
- Johansson, A.; Grant, J.E.; Kim, S.W.; Odlaug, B.L.; Gotestam, K.G. Risk factors for problematic gambling: A critical literature review. J. Gambl. Stud. 2009, 25, 67–92. [Google Scholar] [CrossRef] [PubMed]
- Efron, B.; Tibshirani, R. An Introduction to the Bootstrap; Chapman & Hall: New York, NY, USA, 1993. [Google Scholar]
- Aiken, L.S.; West, S.G.; Reno, R.R. Multiple Regression: Testing and Interpreting Interactions; Sage: Thousand Oaks, CA, USA, 1991. [Google Scholar]
- Cohen, J.; Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences, 3rd ed.; Lawrence Erlbaum: Mahwah, NJ, USA, 2003. [Google Scholar]
- Huang, G.-H. Responsible gambling policies and practices in Macao: A critical review. Asian J. Gambl. Issues Public Health 2011, 2, 49–60. [Google Scholar] [CrossRef]
- Institute for the Study of Commercial Gaming (ISCG). Responsible Gambling Awareness Survey 2017; ISCG: Taipa, Macao, China, 2018. [Google Scholar]
- Blaszczynski, A.; Nower, L.A. pathways model of problem and pathological gambling. Addiction 2002, 97, 487–499. [Google Scholar] [CrossRef] [PubMed]
- King, D.; Delfabbro, P.; Griffiths, M. Video Game Structural Characteristics: A New Psychological Taxonomy. Int. J. Ment. Health Ad. 2010, 8, 90–106. [Google Scholar] [CrossRef]
- Shaffer, H.J.; Hall, M.N. The natural history of gambling and drinking problems among casino employees. J. Soc. Psychol. 2002, 142, 405–424. [Google Scholar] [CrossRef]
- Steger, M.F.; Mann, J.R.; Michels, P.; Cooper, T.C. Meaning in life, anxiety, depression, and general health among smoking cessation patients. J. Psychosom. Res. 2009, 67, 353–358. [Google Scholar] [CrossRef]


{kind=link}
| Overall Sample Subgroups | Gambler Subgroups | |||
|---|---|---|---|---|
| Non-Gambler (n = 817) | Recent Gambler (n = 183) | Non-GD (n = 168) | Probable GD (n = 19) | |
| Age | U = 56297.00, z = −1.63, p = 0.10 | U = 1075.50, z = −1.10, p = 0.27 | ||
| [M (SD)] | 39.60 (15.39) | 41.51 (15.11) | 41.09 (14.87) | 45.29 (17.13) |
| Sex | χ2(1) = 42.31, p < 0.001 | χ2(1) = 3.26, p = 0.07 | ||
| [Male] | 39.2% | 65.6% | 63.4% | 84.2% |
| Educational attainment | U = 64558.00, z = −1.99, p = 0.05 | U = 884.50, z = −2.56, p = 0.01 | ||
| Primary or below | 13.1% | 20.0% | 17.7% | 41.3% |
| Junior secondary | 15.1% | 16.7% | 16.0% | 23.5% |
| Senior secondary | 28.3% | 24.4% | 25.2% | 17.6% |
| Tertiary | 43.5% | 38.9% | 41.1% | 17.6% |
| Working status | χ2(3) = 3.49, p = 0.32 | χ2(3) = 1.39, p = 0.71 | ||
| Full-time | 62.0% | 65.2% | 64.4% | 72.2% |
| Part-time | 5.7% | 7.7% | 7.4% | 11.1% |
| Student | 9.6% | 6.1% | 6.1% | 5.6% |
| Other | 22.7% | 21.0% | 22.1% | 11.1% |
| Casino Employee | χ2(1) = 0.002, p = 0.97 | χ2(1) = 1.54, p = 0.22 | ||
| [Yes%] | 11.6% | 13.1% | 13.7% | 5.3% |
| Gambling expense a | − | U = 671.50, z = −3.59, p < 0.001 | ||
| [Mdn] | − | $12.37–61.76 | $12.37–61.76 | $123.76–247.40 |
| Resilience | t (996) = −0.10, p = 0.92 | t (181) = 0.12, p = 0.91 | ||
| [M (SD)] | 2.59 (0.67) | 2.59 (0.68) | 2.59 (0.68) | 2.57 (0.70) |
| Purpose in life | t (998) = −0.90, p = 0.37 | t (181) = 0.41, p = 0.69 | ||
| [M (SD)] | 3.36 (0.64) | 3.32 (0.61) | 3.32 (0.60) | 3.26 (0.65) |
| Mental health problems | ||||
| Depression | χ2(1) = 0.48, p = 0.49 | χ2(1) = 9.49, p = 0.01 | ||
| DASS < 14 [n (%)] | 722 (88.4%) | 165 (90.2%) | 151 (92.1%) | 14 (73.7%) |
| DASS ≥ 14 [n (%)] | 95 (11.6%) | 18 (9.8%) | 13 (7.9%) | 5 (26.3%) |
| Anxiety | χ2(1) = 0.27, p = 0.61 | χ2(1) = 2.54, p = 0.11 | ||
| DASS < 10 [n (%)] | 648 (79.3%) | 142 (77.6%) | 130 (79.3%) | 12 (63.2%) |
| DASS ≥ 10 [n (%)] | 169 (20.7%) | 41 (22.4%) | 34 (20.7%) | 7 (36.8%) |
| IGD b | χ2(1) = 1.47, p = 0.23 | χ2(1) = 13.44, p < 0.001 | ||
| DSM-5 < 5 [n (%)] | 344 (96.4%) | 104 (93.7%) | 94 (96.9%) | 10 (71.4%) |
| DSM-5 ≥ 5 [n (%)] | 13 (3.6%) | 7 (6.3%) | 3 (3.1%) | 4 (28.6%) |
| Models | GD Symptoms | Probable GD | ||
|---|---|---|---|---|
| Moderating Effect Terms | b [95% CI] a | Interaction Effect | OR [95% CI] a | Interaction Effect |
| 1. Depression symptoms × purpose | 0.04 [−0.04, 0.07] | R2Change = 0.02, F (1,162) = 3.65, p = 0.06 | 1.08 [0.89, 1.17] | χ2(1) = 3.30, p = 0.07 |
| 2. Depression symptoms × resilience | −0.01 [−0.11, 0.03] | R2Change = 0.001, F (1,162) = 0.18, p = 0.68 | 0.98 [0.86, 1.06] | χ2(1) = 0.13, p = 0.72 |
| 3. Anxiety symptoms × purpose | 0.03 [−0.07, 0.07] | R2Change = 0.01, F (1,162) = 1.92, p = 0.17 | 1.06 [0.84, 1.17] | χ2(1) = 1.86, p = 0.17 |
| 4. Anxiety symptoms × resilience | −0.08 [−0.16, −0.004] | R2Change = 0.035, F (1,162) = 6.29, p = 0.01 | 0.89 [0.79, 0.94] | χ2(1) = 4.30, p = 0.04 |
| 5. IGD symptoms × purpose | −0.01 [−0.72, 0.27] | R2Change < 0.001, F (1,98) = 0.01, p = 0.92 | 1.29 [0.26, 2.27] | χ2(1) = 1.06, p = 0.30 |
| 6. IGD symptoms × resilience | −0.10 [−0.73, 0.16] | R2Change = 0.004, F (1,98) = 0.44, p = 0.51 | 1.17 [0.38, 2.44] | χ2(1) = 0.38, p = 0.54 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.H.; Tong, K.K.; Wu, A.M.S.; Lau, J.T.F.; Zhang, M.X. The Comorbidity of Gambling Disorder among Macao Adult Residents and the Moderating Role of Resilience and Life Purpose. Int. J. Environ. Res. Public Health 2018, 15, 2774. https://doi.org/10.3390/ijerph15122774
Chen JH, Tong KK, Wu AMS, Lau JTF, Zhang MX. The Comorbidity of Gambling Disorder among Macao Adult Residents and the Moderating Role of Resilience and Life Purpose. International Journal of Environmental Research and Public Health. 2018; 15(12):2774. https://doi.org/10.3390/ijerph15122774
Chicago/Turabian StyleChen, Juliet Honglei, Kwok Kit Tong, Anise M. S. Wu, Joseph T. F. Lau, and Meng Xuan Zhang. 2018. "The Comorbidity of Gambling Disorder among Macao Adult Residents and the Moderating Role of Resilience and Life Purpose" International Journal of Environmental Research and Public Health 15, no. 12: 2774. https://doi.org/10.3390/ijerph15122774
APA StyleChen, J. H., Tong, K. K., Wu, A. M. S., Lau, J. T. F., & Zhang, M. X. (2018). The Comorbidity of Gambling Disorder among Macao Adult Residents and the Moderating Role of Resilience and Life Purpose. International Journal of Environmental Research and Public Health, 15(12), 2774. https://doi.org/10.3390/ijerph15122774