Unfavorable Mortality-To-Incidence Ratio of Lung Cancer Is Associated with Health Care Disparity



 and
and
Abstract
:1. Introduction
2. Methods
Ethics Approval and Consent to Participate
3. Results
3.1. Crude Rates of Incidence/Mortality According to Regions
3.2. Crude rates of Incidence/Mortality and Case Numbers of Incidence/Mortality According to Countries
3.3. MIRs According to Countries
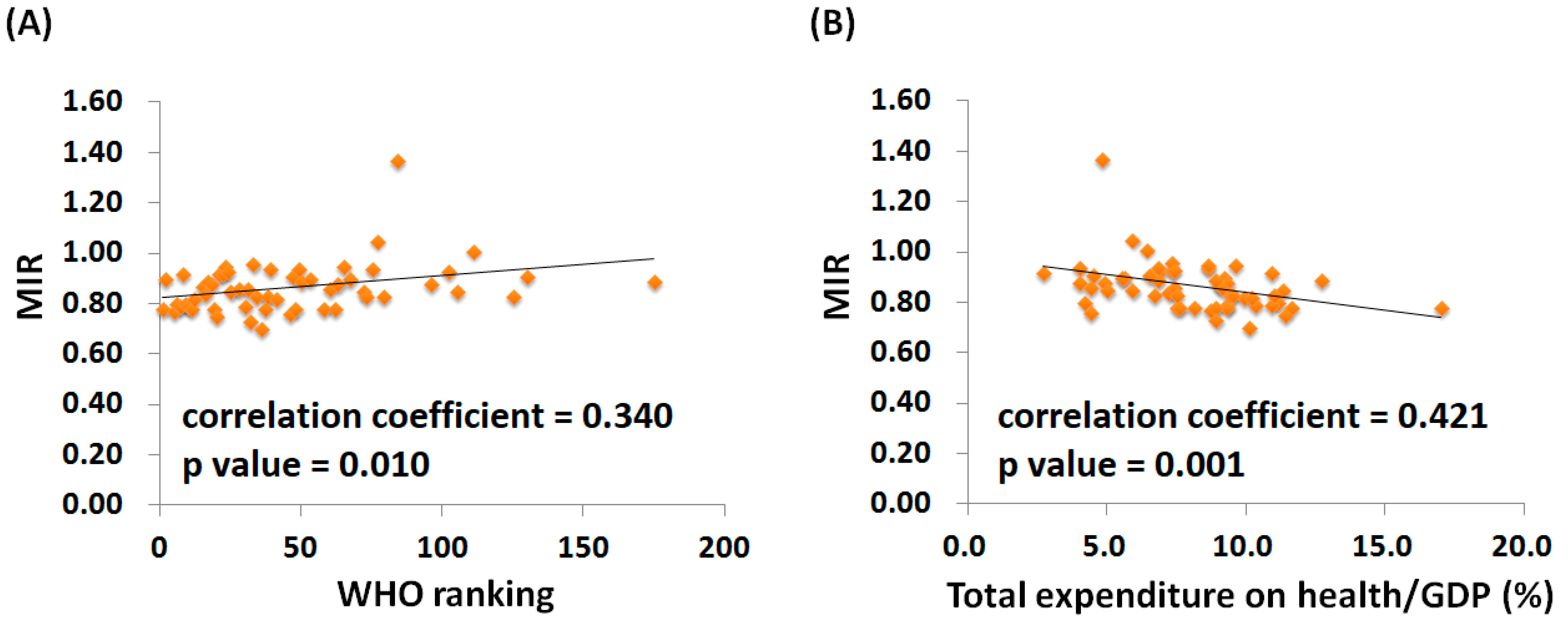
3.4. The Association between WHO Ranking, e/GDP, and MIR among Countries
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| e/GDP | Total expenditures on health/Gross Domestic Product |
| LDCT | Low Dose Computed Tomography |
| MIR | Mortality-to-Incidence Ratio |
| WHO | World Health Organization |
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eberth, J.M. Lung Cancer Screening With Low-Dose CT in the United States. J. Am. Coll. Radiol. 2015, 12, 1395–1402. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.Y.; Luo, L.; Hu, Y.H.; Chen, H.; Den, Y.K.; Tang, L.; Liu, B.; Liu, D.; Zhang, X.Y. Lung cancer screening: A systematic review of clinical practice guidelines. Int. J. Clin. Pract. 2016, 70, 20–30. [Google Scholar] [CrossRef]
- Zeng, L.; Yu, X.; Yu, T.; Xiao, J.; Huang, Y. Interventions for smoking cessation in people diagnosed with lung cancer. Cochrane Database Syst. Rev. 2015, 12, CD011751. [Google Scholar] [CrossRef]
- Fucito, L.M.; Czabafy, S.; Hendricks, P.S.; Kotsen, C.; Richardson, D.; Toll, B.A. Pairing smoking-cessation services with lung cancer screening: A clinical guideline from the Association for the Treatment of Tobacco Use and Dependence and the Society for Research on Nicotine and Tobacco. Cancer 2016, 122, 1150–1159. [Google Scholar] [CrossRef] [Green Version]
- Tse, L.A.; Lin, X.; Li, W.; Qiu, H.; Chan, C.K.; Wang, F.; Yu, I.T.; Leung, C.C. Smoking cessation sharply reduced lung cancer mortality in a historical cohort of 3185 Chinese silicotic workers from 1981 to 2014. Br. J. Cancer 2018, 119, 1557–1562. [Google Scholar] [CrossRef] [PubMed]
- Asadzadeh Vostakolaei, F.; Karim-Kos, H.E.; Janssen-Heijnen, M.L.; Visser, O.; Verbeek, A.L.; Kiemeney, L.A. The validity of the mortality to incidence ratio as a proxy for site-specific cancer survival. Eur. J. Public Health 2011, 21, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Parkin, D.M.; Bray, F. Evaluation of data quality in the cancer registry: Principles and methods Part II. Completeness. Eur. J. Cancer 2009, 45, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Sunkara, V.; Hebert, J.R. The colorectal cancer mortality-to-incidence ratio as an indicator of global cancer screening and care. Cancer 2015, 121, 1563–1569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.C.; Tsai, M.C.; Peng, C.M.; Lee, H.L.; Chen, H.Y.; Yang, T.W.; Sung, W.W.; Lin, C.C. Favorable liver cancer mortality-to-incidence ratios of countries with high health expenditure. Eur. J. Gastroenterol. Hepatol. 2017, 29, 1397–1401. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.C.; Wang, C.C.; Lee, H.L.; Peng, C.M.; Yang, T.W.; Chen, H.Y.; Sung, W.W.; Lin, C.C. Health disparities are associated with gastric cancer mortality-to-incidence ratios in 57 countries. World J. Gastroenterol. 2017, 23, 7881–7887. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.L.; Wang, S.C.; Ho, C.J.; Kao, Y.L.; Hsieh, T.Y.; Chen, W.J.; Chen, C.J.; Wu, P.R.; Ko, J.L.; Lee, H.; et al. Prostate Cancer Mortality-To-Incidence Ratios Are Associated with Cancer Care Disparities in 35 Countries. Sci. Rep. 2017, 7, 40003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanchon, T.; Brechot, J.M.; Grenier, P.A.; Ferretti, G.R.; Lemarie, E.; Milleron, B.; Chague, D.; Laurent, F.; Martinet, Y.; Beigelman-Aubry, C.; et al. Baseline results of the Depiscan study: A French randomized pilot trial of lung cancer screening comparing low dose CT scan (LDCT) and chest X-ray (CXR). Lung Cancer 2007, 58, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Aberle, D.R.; Adams, A.M.; Berg, C.D.; Black, W.C.; Clapp, J.D.; Fagerstrom, R.M.; Gareen, I.F.; Gatsonis, C.; Marcus, P.M.; Sicks, J.D. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [PubMed]
- Hensing, T.A.; Salgia, R. Molecular biomarkers for future screening of lung cancer. J. Surg. Oncol. 2013, 108, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C. Outdoor air pollution: A global perspective. J. Occup. Environ. Med. 2014, 56 (Suppl. 10), S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Dai, H.; Dong, H.; Hanaoka, T.; Masui, T. Economic Impacts from PM2.5 Pollution-Related Health Effects in China: A Provincial-Level Analysis. Environ. Sci. Technol. 2016, 50, 4836–4843. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Region | Number | Crude Rate 1 | Age-Standardized Rate 1 | Mortality-to-Incidence Ratio 2 | |||
|---|---|---|---|---|---|---|---|
| Incidence | Mortality | Incidence | Mortality | Incidence | Mortality | ||
| World | 1,824,701 | 1,589,925 | 25.9 | 22.5 | 23.1 | 19.7 | 0.87 |
| Development | |||||||
| More developed regions | 758,214 | 626,570 | 60.9 | 50.3 | 30.8 | 24.2 | 0.83 |
| Less developed regions | 1,066,487 | 963,355 | 18.4 | 16.6 | 20.0 | 18.0 | 0.90 |
| WHO region categories | |||||||
| WHO Africa region | 18,051 | 16,108 | 2.1 | 1.8 | 3.9 | 3.5 | 0.86 |
| WHO Americas region | 324,301 | 262,314 | 34.0 | 27.5 | 26.0 | 20.4 | 0.81 |
| WHO East Mediterranean region | 32,542 | 28,977 | 5.2 | 4.7 | 7.9 | 7.1 | 0.90 |
| WHO Europe region | 448,618 | 388,203 | 49.7 | 43.0 | 28.7 | 24.0 | 0.87 |
| WHO South-East Asia region | 162,003 | 146,216 | 8.7 | 7.9 | 10.5 | 9.5 | 0.91 |
| WHO Western Pacific region | 838,978 | 747,920 | 45.5 | 40.6 | 32.8 | 28.5 | 0.89 |
| Continent | |||||||
| Africa | 30,314 | 27,083 | 2.8 | 2.5 | 5.0 | 4.5 | 0.89 |
| Latin America and Caribbean | 84,520 | 74,602 | 14.0 | 12.4 | 13.7 | 12.0 | 0.89 |
| Northern America | 239,781 | 187,712 | 68.4 | 53.5 | 38.3 | 28.6 | 0.78 |
| Asia | 1,045,695 | 936,051 | 24.6 | 22.0 | 23.4 | 20.7 | 0.89 |
| Europe | 410,220 | 353,848 | 55.3 | 47.7 | 29.0 | 24.0 | 0.86 |
| Oceania | 14,171 | 10,629 | 37.6 | 28.2 | 25.3 | 18.3 | 0.75 |
| Country | Ranking | Total Expenditure on Health/GDP (%) | Life Expectancy 1 | Number | Crude Rate 2 | Age-Standardized Rate 2 | Mortality-to-Incidence Ratio 3 | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Incidence | Mortality | Incidence | Mortality | Incidence | Mortality | |||||
| France | 1 | 11.6 | 82 | 40,043 | 31,434 | 63.1 | 49.5 | 35.0 | 25.3 | 0.78 |
| Italy | 2 | 9.2 | 83 | 37,238 | 33,531 | 61.1 | 55.0 | 24.5 | 20.7 | 0.90 |
| Malta | 5 | 8.7 | 81 | 181 | 139 | 43.2 | 33.2 | 20.4 | 15.6 | 0.77 |
| Singapore | 6 | 4.2 | 83 | 1974 | 1590 | 37.6 | 30.2 | 24.9 | 19.8 | 0.80 |
| Spain | 7 | 9.3 | 83 | 26,715 | 21,118 | 57.1 | 45.2 | 30.3 | 22.8 | 0.79 |
| Oman | 8 | 2.7 | 76 | 76 | 70 | 2.6 | 2.4 | 5.1 | 4.8 | 0.92 |
| Austria | 9 | 11.1 | 81 | 4576 | 3658 | 54.3 | 43.4 | 27.5 | 20.7 | 0.80 |
| Japan | 10 | 10.3 | 84 | 94,855 | 75,119 | 75.0 | 59.4 | 24.6 | 17.4 | 0.79 |
| Norway | 11 | 9.3 | 82 | 2845 | 2219 | 57.4 | 44.7 | 30.0 | 22.2 | 0.78 |
| Portugal | 12 | 9.9 | 81 | 4192 | 3441 | 39.2 | 32.2 | 20.2 | 15.7 | 0.82 |
| Iceland | 15 | 9.0 | 82 | 162 | 141 | 49.3 | 42.9 | 29.8 | 24.5 | 0.87 |
| Luxembourg | 16 | 7.2 | 82 | 261 | 218 | 49.9 | 41.7 | 28.4 | 23.1 | 0.84 |
| Netherlands | 17 | 12.7 | 81 | 11,968 | 10,609 | 71.6 | 63.5 | 37.2 | 30.5 | 0.89 |
| United Kingdom | 18 | 9.3 | 81 | 40,382 | 35,581 | 64.3 | 56.7 | 30.0 | 25.4 | 0.88 |
| Ireland | 19 | 8.9 | 81 | 2273 | 1778 | 49.6 | 38.8 | 31.3 | 23.6 | 0.78 |
| Switzerland | 20 | 11.4 | 83 | 4237 | 3194 | 54.8 | 41.3 | 27.3 | 20.0 | 0.75 |
| Belgium | 21 | 10.9 | 80 | 7794 | 7179 | 72.2 | 66.5 | 36.8 | 30.5 | 0.92 |
| Colombia | 22 | 6.8 | 78 | 4780 | 4417 | 10.1 | 9.3 | 11.0 | 10.1 | 0.92 |
| Sweden | 23 | 9.6 | 82 | 3891 | 3695 | 41.0 | 38.9 | 19.1 | 16.4 | 0.95 |
| Cyprus | 24 | 7.3 | 82 | 276 | 258 | 24.4 | 22.8 | 16.2 | 14.7 | 0.93 |
| Germany | 25 | 11.3 | 81 | 50,813 | 43,420 | 62.0 | 53.0 | 27.5 | 22.2 | 0.85 |
| Israel | 28 | 7.4 | 82 | 2270 | 1956 | 29.5 | 25.4 | 21.2 | 17.9 | 0.86 |
| Canada | 30 | 10.9 | 82 | 25,481 | 20,108 | 73.5 | 58.0 | 37.9 | 28.4 | 0.79 |
| Finland | 31 | 9.1 | 81 | 2494 | 2138 | 46.2 | 39.6 | 20.1 | 16.7 | 0.86 |
| Australia | 32 | 8.9 | 83 | 11,331 | 8232 | 49.4 | 35.9 | 27.0 | 18.5 | 0.73 |
| Chile | 33 | 7.3 | 80 | 3127 | 2980 | 17.9 | 17.1 | 13.3 | 12.5 | 0.96 |
| Denmark | 34 | 11.0 | 80 | 4566 | 3806 | 81.6 | 68.1 | 39.2 | 31.4 | 0.83 |
| Costa Rica | 36 | 10.1 | 79 | 363 | 256 | 7.6 | 5.3 | 7.3 | 5.1 | 0.70 |
| United States of America | 37 | 17.0 | 79 | 214,226 | 167,545 | 67.8 | 53.1 | 38.4 | 28.6 | 0.78 |
| Slovenia | 38 | 9.4 | 80 | 1360 | 1131 | 66.7 | 55.4 | 33.9 | 26.8 | 0.83 |
| Cuba | 39 | 8.6 | 78 | 6143 | 5763 | 54.6 | 51.2 | 32.9 | 30.1 | 0.94 |
| New Zealand | 41 | 10.2 | 82 | 2027 | 1659 | 45.4 | 37.2 | 25.9 | 20.8 | 0.82 |
| Bahrain | 46 | 4.4 | 77 | 84 | 64 | 6.2 | 4.7 | 15.5 | 12.4 | 0.76 |
| Thailand | 47 | 4.5 | 75 | 19,505 | 17,669 | 27.9 | 25.3 | 20.9 | 19.1 | 0.91 |
| Czech Republic | 48 | 7.5 | 78 | 6683 | 5228 | 63.3 | 49.5 | 32.5 | 24.7 | 0.78 |
| Malaysia | 49 | 4.0 | 74 | 4403 | 4134 | 15.0 | 14.1 | 17.9 | 17.0 | 0.94 |
| Poland | 50 | 6.8 | 77 | 26,230 | 23,371 | 68.5 | 61.0 | 38.0 | 33.4 | 0.89 |
| Jamaica | 53 | 5.6 | 74 | 512 | 460 | 18.5 | 16.7 | 18.2 | 15.8 | 0.90 |
| Korea, Republic of | 58 | 7.6 | 82 | 22,873 | 17,848 | 47.1 | 36.7 | 28.7 | 21.3 | 0.78 |
| Philippines | 60 | 4.4 | 69 | 12,074 | 10,369 | 12.5 | 10.7 | 19.3 | 17.0 | 0.86 |
| Slovakia | 62 | 8.1 | 76 | 2531 | 1981 | 46.2 | 36.1 | 28.3 | 21.6 | 0.78 |
| Egypt | 63 | 4.9 | 71 | 5017 | 4488 | 6.0 | 5.3 | 7.2 | 6.5 | 0.88 |
| Uruguay | 65 | 8.6 | 77 | 1411 | 1336 | 41.6 | 39.4 | 27.4 | 25.1 | 0.95 |
| Trinidad and Tobago | 67 | 5.5 | 71 | 184 | 165 | 13.6 | 12.2 | 12.2 | 10.8 | 0.90 |
| Belarus | 72 | 5.0 | 72 | 4012 | 3422 | 42.1 | 35.9 | 26.2 | 22.1 | 0.85 |
| Lithuania | 73 | 6.7 | 74 | 1555 | 1292 | 47.2 | 39.2 | 26.2 | 21.2 | 0.83 |
| Argentina | 75 | 6.8 | 76 | 11,244 | 10,531 | 27.3 | 25.6 | 20.9 | 19.1 | 0.94 |
| Estonia | 77 | 5.9 | 77 | 632 | 665 | 47.2 | 49.6 | 24.4 | 23.6 | 1.05 |
| Ukraine | 79 | 7.5 | 71 | 17,251 | 14,270 | 38.4 | 31.8 | 22.2 | 18.5 | 0.83 |
| Mauritius | 84 | 4.8 | 74 | 149 | 204 | 11.3 | 15.5 | 9.9 | 13.4 | 1.37 |
| Fiji | 96 | 4.0 | 70 | 45 | 39 | 5.1 | 4.5 | 6.0 | 5.1 | 0.88 |
| Bulgaria | 102 | 7.4 | 75 | 3936 | 3659 | 53.2 | 49.5 | 28.1 | 25.9 | 0.93 |
| Latvia | 105 | 5.9 | 74 | 1183 | 1002 | 52.9 | 44.8 | 27.8 | 22.2 | 0.85 |
| Ecuador | 111 | 6.4 | 76 | 1035 | 1057 | 7.0 | 7.1 | 7.2 | 7.2 | 1.01 |
| Brazil | 125 | 9.5 | 75 | 34,280 | 28,285 | 17.3 | 14.3 | 16.3 | 13.3 | 0.83 |
| Russian Federation | 130 | 6.5 | 69 | 55,805 | 50,888 | 39.1 | 35.7 | 24.0 | 21.5 | 0.91 |
| South African Republic | 175 | 8.9 | 60 | 7242 | 6465 | 14.3 | 12.7 | 18.5 | 16.7 | 0.89 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-Y.; Au, K.-K.; Chen, S.-L.; Wang, S.-C.; Liao, C.-Y.; Hsu, H.-H.; Sung, W.-W.; Wang, Y.-C. Unfavorable Mortality-To-Incidence Ratio of Lung Cancer Is Associated with Health Care Disparity. Int. J. Environ. Res. Public Health 2018, 15, 2889. https://doi.org/10.3390/ijerph15122889
Huang C-Y, Au K-K, Chen S-L, Wang S-C, Liao C-Y, Hsu H-H, Sung W-W, Wang Y-C. Unfavorable Mortality-To-Incidence Ratio of Lung Cancer Is Associated with Health Care Disparity. International Journal of Environmental Research and Public Health. 2018; 15(12):2889. https://doi.org/10.3390/ijerph15122889
Chicago/Turabian StyleHuang, Cheng-Yu, Kwong-Kwok Au, Sung-Lang Chen, Shao-Chuan Wang, Chi-Yu Liao, Hui-Hsiang Hsu, Wen-Wei Sung, and Yao-Chen Wang. 2018. "Unfavorable Mortality-To-Incidence Ratio of Lung Cancer Is Associated with Health Care Disparity" International Journal of Environmental Research and Public Health 15, no. 12: 2889. https://doi.org/10.3390/ijerph15122889
APA StyleHuang, C. -Y., Au, K. -K., Chen, S. -L., Wang, S. -C., Liao, C. -Y., Hsu, H. -H., Sung, W. -W., & Wang, Y. -C. (2018). Unfavorable Mortality-To-Incidence Ratio of Lung Cancer Is Associated with Health Care Disparity. International Journal of Environmental Research and Public Health, 15(12), 2889. https://doi.org/10.3390/ijerph15122889