What Works? Toward a New Classification System for Mental Health Supported Accommodation Services: The Simple Taxonomy for Supported Accommodation (STAX-SA)



Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
Domains-Based Taxonomy
2.2. Method
2.2.1. Development
2.2.2. Initial Testing and Refinement
2.2.3. Final Testing
2.2.4. Validation: Publication Date and Research Design
2.2.5. External Validity
3. Results
3.1. Initial Testing and Refinement
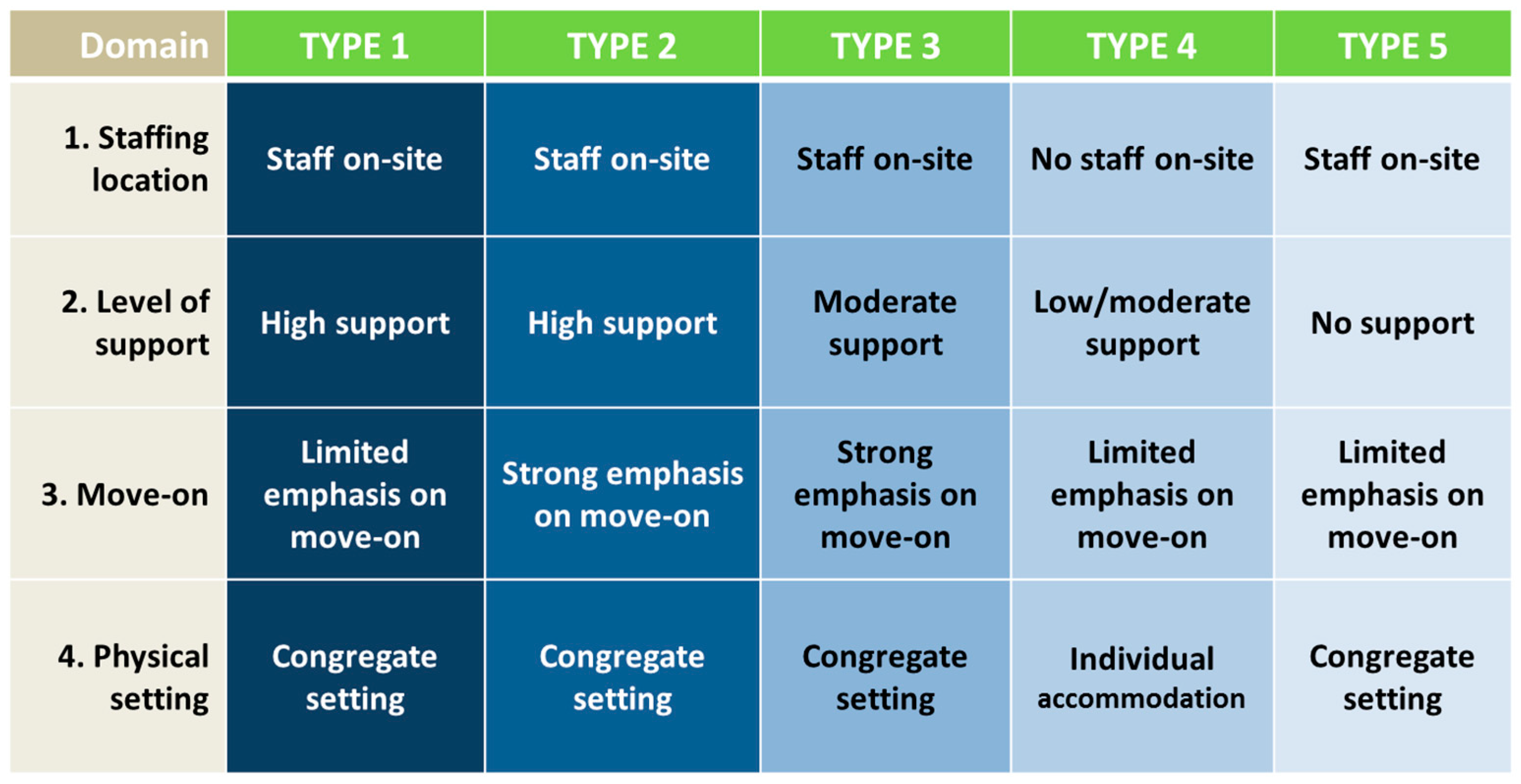
3.2. Final Testing: STAX-SA
3.3. Publication Date and Research Design
3.4. External Validity
4. Discussion
4.1. Application to the Literature
4.2. External Validity
4.3. Strengths and Limitations
4.4. Future Directions
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| STAX-SA | Simple Taxonomy for Supported Accommodation |
| DTSA | Domains-Based Taxonomy for Supported Accommodation |
| WHO-AIMS | World Health Organization Assessment Instrument for Mental Health Systems |
| ESMS | the European Service Mapping Schedule |
| DESDE-LTC | Description and Evaluation of Services and Directories in Europe-Long Term Care |
| QUEST | Quality and Effectiveness of Supported Tenancies for people with mental health problems |
| NIHR | National Institute for Health Research |
| UK | United Kingdom |
| MH | Mental Health |
| RC | Residential Care |
| SH | Supported Housing |
| FO | Floating Outreach |
| CONSORT | Consolidated Standards of Reporting Trials |
| RCT | Randomized controlled trial |
References
- Johnson, S.; Kuhlmann, R. The European Service Mapping Schedule (ESMS): Development of an instrument for the description and classification of mental health services. Acta Psychiatr. Scand. Suppl. 2000, 405, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Mental Health: Evidence and Research Team (MER). World Health Organization Assessment Instrument for Mental health Systems (WHO-AIMS); World Health Organization: Geneva, Switzerland, 2005; Volume 92. [Google Scholar]
- Salvador-Carulla, L.; Alvarez-Galvez, J.; Romero, C.; Gutiérrez-Colosía, M.R.; Weber, G.; McDaid, D.; Dimitrov, H.; Sprah, L.; Kalseth, B.; Tibaldi, G.; et al. Evaluation of an integrated system for classification, assessment and comparison of services for long-term care in Europe: The eDESDE-LTC study. BMC Health Serv. Res. 2013, 13, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabol, C.; Drebing, C.; Rosenheck, R. Studies of “supported” and “supportive” housing: A comprehensive review of model descriptions and measurement. Eval. Program Plan. 2010, 33, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Macpherson, R.; Shepherd, G.; Thyarappa, P. Supported accommodation for people with severe mental illness: An update. Adv. Psychiatr. Treat. 2012, 18, 381–391. [Google Scholar] [CrossRef]
- Gustafsson, C.; Goulding, A.; Abrams, D.; Nylander, R.-M.; Wiberg, C.; Orem, E. Boendeformer och Boendeinsatser för Personer Med Psykiska Funktionshinder. Systematisk Kartläggning av Publikationer 1980–2007; Socialstyrelsen: Stockholm, Sweden, 2009. [Google Scholar]
- McPherson, P.; Krotofil, J.; Killaspy, H. Specialist mental health supported accommodation services: A systematic review of mental health and psychosocial outcomes. BMC Psychiatry 2017, in press. [Google Scholar]
- Fakhoury, W.K.H.; Murray, A.; Shepherd, G.; Priebe, S. Research in supported housing. Soc. Psychiatry Psychiatr. Epidemiol. 2002, 37, 301–315. [Google Scholar] [CrossRef] [PubMed]
- Bradley, E.H.; Curry, L.A.; Devers, K.J. Qualitative data analysis for health services research: Developing taxonomy, themes, and theory. Health Serv. Res. 2007, 42, 1758–1772. [Google Scholar] [CrossRef] [PubMed]
- Porterfield, D.S.; Rojas-smith, L.; Lewis, M.; Mccormack, L.A.; Hoerger, T.J.; Holden, D.J. A Taxonomy of Interventions between Health Care and Public Health. RTI Int. 2015. [Google Scholar] [CrossRef]
- Gilmer, T.P.; Stefancic, A.; Sklar, M.; Tsemberis, S. Development and Validation of a Housing First Fidelity Survey. Psychiatr. Serv. 2013, 64, 911–914. [Google Scholar] [CrossRef] [PubMed]
- Gilmer, T.P.; Stefancic, A.; Katz, M.L.; Sklar, M.; Tsemberis, S.; Palinkas, L.A. Fidelity to the Housing First Model and Effectiveness of Permanent Supported Housing Programs in California. Psychiatr. Serv. 2014, 65, 1311–1317. [Google Scholar] [CrossRef] [PubMed]
- Gilmer, T.P.; Stefancic, A.; Henwood, B.F.; Ettner, S.L. Fidelity to the Housing First Model and Variation in Health Service Use within Permanent Supportive Housing. Psychiatr. Serv. 2015, 66, 1283–1289. [Google Scholar] [CrossRef] [PubMed]
- Barbato, A.; Civenti, G.; D’Avanzo, B. Community residential facilities in mental health services: A ten-year comparison in Lombardy. Health Policy 2017, 121, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Verdoux, H. The current state of adult mental health care in France. Eur. Arch. Psychiatry Clin. Neurosci. 2007, 257, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Siskind, D.; Harris, M.; Pirkis, J.; Whiteford, H. A domains-based taxonomy of supported accommodation for people with severe and persistent mental illness. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 875–894. [Google Scholar] [CrossRef] [PubMed]
- Krotofil, J.; McPherson, P.; Killaspy, H. Service user experiences of specialist mental health supported accommodation: A systematic review of qualitative studies and narrative synthesis. Health Soc. Care Community 2017, in press. [Google Scholar]
- Killaspy, H.; Priebe, S.; Bremner, S.; McCrone, P.; Dowling, S.; Harrison, I.; Krotofil, J.; McPherson, P.; Sandhu, S.; Arbuthnott, M.; et al. Quality of life, autonomy, satisfaction, and costs associated with mental health supported accommodation services in England: A national survey. Lancet Psychiatry 2016, 3, 1129–1137. [Google Scholar] [CrossRef]
- Ball, R.A.; Moore, E.; Kuipers, L. Expressed Emotion in community care staff. A comparison of patient outcome in a nine month follow-up of two hostels. Soc. Psychiatry Psychiatr. Epidemiol. 1992, 27, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Barbato, A.; D’Avanzo, B.; Rocca, G.; Amatulli, A.; Lampugnani, D. A Study of Long-Stay Patients Resettled in the Community after Closure of a Psychiatric Hospital in Italy. Psychiatr. Serv. 2004, 55, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Barr, W.; Brown, A.; Quinn, B.; Mcfarlane, J.; Mccabe, R.; Whittington, R. How effective is high-support community-based step-down housing for women in secure mental health care? A quasi-experimental pilot study. J. Psychiatr. Ment. Health Nurs. 2013, 20, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Bengtsson-Tops, A.; Ericsson, U.; Ehliasson, K. Living in supportive housing for people with serious mental illness: A paradoxical everyday life. Int. J. Ment. Health Nurs. 2014, 23, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Boydell, K.M.; Everett, B. What makes a house a home? An evaluation of a supported housing project for individuals with long-term psychiatric backgrounds. Can. J. Community Ment. Health 1992, 11, 109–123. [Google Scholar] [CrossRef]
- Boydell, K.M.; Gladstone, B.M.; Crawford, E.; Trainor, J. Making do on the outside: Everyday life in the neighborhoods of people with psychiatric disabilities. Psychiatr. Rehabil. J. 1999, 23, 11–18. [Google Scholar] [CrossRef]
- Brolin, R.; Brunt, D.; Rask, M.; Syrén, S.; Sandgren, A. Striving for meaning-life in supported housing for people with psychiatric disabilities. Int. J. Qual. Stud. Health Well-Being 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Ridgway, P.; Anthony, W.A.; Rogers, E.S. Comparison of outcomes for clients seeking and assigned to supported housing services. Hosp. Community Psychiatry 1991, 42, 1150–1153. [Google Scholar] [CrossRef] [PubMed]
- Browne, G.; Courtney, M. Housing, social support and people with schizophrenia: A grounded theory study. Issues Ment. Health Nurs. 2005, 26, 311–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caplan, B.; Schutt, R.K.; Turner, W.M.; Goldfinger, S.M.; Seidman, L.J. Change in neurocognition by housing type and substance abuse among formerly homeless seriously mentally ill persons. Schizophr. Res. 2006, 83, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Carpenter-Song, E.; Hipolito, M.M.S.; Whitley, R. “Right here is an oasis”: How “recovery communities” contribute to recovery for people with serious mental illnesses. Psychiatr. Rehabil. J. 2012, 35, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Carta, M.G.; Agaj, A.; Harapej, E.; Lecca, M.E.; Xhelili, G.; Altoé, G.; Mura, G.; Moro, M.F.; Angermeyer, M.C. Outcomes of discharged females versus those waiting for discharge from Vlore Psychiatric Hospital (Albania). Int. J. Soc. Psychiatry 2013, 59, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Casper, E.S.; Clark, D. Service Utilization, Incidents, and Hospitalizations among People with Mental Illnesses and Incarceration Histories in a Supportive Housing Program. Psychiatr. Rehabil. J. 2004, 28, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Chan, G.W.L.; Ungvari, G.S.; Shek, D.T.L.; Leung, J.P. Impact of deinstitutionalisation on the quality of life of Chinese patients with schizophrenia: A longitudinal pilot study. Hong Kong J. Psychiatry 2003, 13, 2–5. [Google Scholar]
- Chan, H.; Inoue, S.; Shimodera, S.; Fujita, H.; Fukuzawa, K.; Kii, M.; Kamimura, N.; Kato, K.; Mino, Y. Residential program for long-term hospitalized persons with mental illness in Japan: Randomized controlled trial. Psychiatry Clin. Neurosci. 2007, 61, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Charlesworth, B.; Sacks, J.; Templer, D.I.; Thackrey, M. Negative emotion as predictor of relapse in persons with schizophrenia living in board and care homes. Community Ment. Health J. 1993, 29, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Chesters, J.; Fletcher, M.; Jones, R. Mental illness recovery. AeJAMH 2005, 4, 89–97. [Google Scholar]
- Chopra, P.; Herrman, H.E. The long-term outcomes and unmet needs of a cohort of former long-stay patients in Melbourne, Australia. Community Ment. Health J. 2011, 47, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Chowdur, R.; Dharitri, R.; Kalyanasundaram, S.; Suryanarayana, R.N. Efficacy of psychosocial rehabilitation program: The RFS experience. Indian J. Psychiatry 2011, 53, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.; Rich, A.R. Outcomes of Homeless Adults with Mental Illness in a Housing Program and in Case Management only. Psychiatr. Serv. 2003, 54, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Cleary, M.; Woolford, P.; Meehan, T. Boarding house life for people with mental illness: An exploratory study. Aust. N. Z. J. Ment. Health Nurs. 1998, 7, 163–171. [Google Scholar] [PubMed]
- Cohen, B.Z.; Hatib, A. The effect of placement in a hostel on the post-hospitalization rehabilitation of psychiatrically disabled persons in Israel. Int. J. Rehabil. Res. 1999, 22, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Crosby, C.; Barry, M.; FitzGerald, M.; Fergus, C. Psychiatric rehabilitation and community care: Resettlement from a North Wales Hospital. Health Soc. Care Community 1993, 1, 355–363. [Google Scholar] [CrossRef]
- Dadich, A.; Fisher, K.R.; Muir, K. How can non-clinical case management complement clinical support for people with chronic mental illness residing in the community? Psychol. Health Med. 2013, 18, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.; Hopkins, M.; Campisi, M.; Maggs, R.G. Developing high relational support services for individuals with long term mental health needs: Scheme description and service evaluation. Ment. Health Soc. Incl. 2012, 16, 31–40. [Google Scholar] [CrossRef]
- Dayson, D.; Lee-Jones, R.; Chahal, K.K.; Leff, J. The TAPS Project 32: Social networks of two group homes ... 5 years on. Soc. Psychiatry Psychiatr. Epidemiol. 1998, 33, 438–444. [Google Scholar] [CrossRef] [PubMed]
- De Girolamo, G.; Candini, V.; Buizza, C.; Ferrari, C.; Boero, M.E.; Giobbio, G.M.; Goldschmidt, N.; Greppo, S.; Iozzino, L.; Maggi, P.; et al. Is psychiatric residential facility discharge possible and predictable? A multivariate analytical approach applied to a prospective study in Italy. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 157–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickey, B.; Gonzalez, O.; Latimer, E.; Powers, K.; Schutt, R.K.; Goldfinger, S. Use of mental health services by formerly homeless adults residing in group and independent housing. Psychiatr. Serv. 1996, 47, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Duurkoop, P.; Van Dyck, R. From a “State Mental Hospital” to New Homes in the City: Longitudinal Research into the Use of Intramural Facilities by Long-Stay Care-Dependent Psychiatric Clients in Amsterdam. Community Ment. Health J. 2003, 39, 77–92. [Google Scholar] [CrossRef] [PubMed]
- Gabrielian, S.; Burns, A.V.; Nanda, N.; Hellemann, G.; Kane, V.; Young, A.S. Factors Associated with Premature Exits From Supported Housing. Psychiatr. Serv. 2016, 67, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Gilmer, T.P.; Stefancic, A.; Ettner, S.L.; Manning, W.G.; Tsemberis, S. Effect of Full-Service Partnerships on Homelessness, Use and Costs of Mental Health Services, and Quality of Life among Adults with Serious Mental Illness. Arch. Gen. Psychiatry 2010, 67, 645. [Google Scholar] [CrossRef] [PubMed]
- Goering, P.; Sylph, J.; Foster, R.; Boyles, S.; Babiak, T. Supportive housing: A consumer evaluation study. Int. J. Soc. Psychiatry 1992, 38, 107–119. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.G.; Westhues, A. Choice and outcome in mental health supported housing. Psychiatr. Rehabil. J. 2010, 33, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Grinshpoon, A.; Naisberg, Y.; Weizman, A. A Six-Month Outcome of Long-Stay Inpatients Resettled in a Hostel. Psychiatr. Rehabil. J. 2006, 30, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Guazzelli, M.; Palagini, L.; Giuntoli, L.; Pietrini, P. Rehab rounds: Outcomes of patients with schizophrenia in a family-style, residential, community-based program in Italy. Psychiatr. Serv. 2000, 51, 1113–1115. [Google Scholar] [CrossRef] [PubMed]
- Hadley, T.R.; McGurrin, M.C.; Fye, D.M. Community residential services and community tenure. Psychosoc. Rehabil. J. 1993, 16, 41–53. [Google Scholar] [CrossRef]
- Hawthorne, W.B.; Fals-Stewart, W.; Lohr, J.B. A treatment outcome study of community-based residential care. Hosp. Community Psychiatry 1994, 45, 152–155. [Google Scholar] [CrossRef] [PubMed]
- Henwood, B.F.; Matejkowski, J.; Stefancic, A.; Lukens, J.M. Quality of life after housing first for adults with serious mental illness who have experienced chronic homelessness. Psychiatry Res. 2014, 220, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Henwood, B.F.; Derejko, K.S.; Couture, J.; Padgett, D.K. Maslow and Mental Health Recovery: A Comparative Study of Homeless Programs for Adults with Serious Mental Illness. Adm. Policy Ment. Health 2015, 42, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Higgins, A.; Webb, M.; O’Neill, G.; Brosnan, R.; Keane, J. The needs for care of the chronic mentally ill relocating from psychiatric hospital to the community: A pilot study. Irish J. Psychol. 1997, 18, 307–320. [Google Scholar] [CrossRef]
- Hodgins, S.; Cyr, M.; Gaston, L. Impact of supervised apartments on the functioning of mentally disordered adults. Community Ment. Health J. 1990, 26, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Hurlburt, M.S.; Wood, P.A.; Hough, R.L. Providing independent housing for the homeless mentally ill: A novel approach to evaluating long-term longitudinal housing patterns. J. Community Psychol. 1996, 24, 291–310. [Google Scholar] [CrossRef]
- Husted, J.; Wentler, S. Changing Self-Perception: Success in Independent Living for Individuals with Chronic Mental Illness. Psychol. Rep. 2006, 99, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Janecek, J. Cluster housing for the mentally ill. The familystyle homes experience. Minn. Med. 1996, 79, 25–28. [Google Scholar] [PubMed]
- Jervis, L.L. An imperfect refuge: Life in an ‘old folk’s home’ for younger residents with psychiatric disorders. Soc. Sci. Med. 2002, 54, 79–91. [Google Scholar] [CrossRef]
- Kallert, T.W.; Leisse, M.; Winiecki, P. Comparing the effectiveness of different types of supported housing for patients with chronic schizophrenia. J. Public Health 2006, 15, 29–42. [Google Scholar] [CrossRef]
- Kasprow, W.J.; Rosenheck, R.A.; Frisman, L.; DiLella, D. Referral and Housing Processes in a Long-Term Supported Housing Program for Homeless Veterans. Psychiatr. Serv. 2000, 51, 1017–1023. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, A.; Lavelle, E. The impact of a rehabilitation and recovery service on patient groups residing in high support community residences. Ir. J. Psychol. Med. 2008, 25, 5–10. [Google Scholar] [CrossRef]
- Kirkpatrick, H.; Byrne, C. A narrative inquiry: Moving on from homelessness for individuals with a major mental illness. J. Psychiatr. Ment. Health Nurs. 2009, 16, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, H.; Byrne, C. A Narrative Inquiry of a Program That Provides Permanent Housing with Supports to Homeless Individuals with Severe Mental Illness. Can. J. Community Ment. Heal. 2011, 30, 31–43. [Google Scholar] [CrossRef]
- Kirkpatrick, H.; Younger, J.; Links, P. Hospital-based schizophrenia program evaluates its supported housing project. Leadersh. Health Serv. 1995, 4, 27–32. [Google Scholar] [PubMed]
- Kirst, M.; Zerger, S.; Wise Harris, D.; Plenert, E.; Stergiopoulos, V. The promise of recovery: Narratives of hope among homeless individuals with mental illness participating in a Housing First randomised controlled trial in Toronto, Canada: Table 1. BMJ Open 2014, 4, e004379. [Google Scholar] [CrossRef] [PubMed]
- Kowlessar, O.A.; Corbett, K.P. The lived experience of mental health service users in a UK community rehabilitation scheme. Int. J. Ther. Rehabil. 2009, 16, 85–95. [Google Scholar] [CrossRef]
- Law, K.K.P.; Yau, S.B.; Wan, D.L.Y. Relationship between perceived quality of life, social functioning, and life skills performance of patients with chronic psychiatric conditions in a long stay care home. Hong Kong J. Psychiatry 2002, 12, 2–7. [Google Scholar]
- Lerner, Y.; Hornik-Lurie, T.; Zilber, N. The Effect of the Implementation of the Rehabilitation of the Mentally Disabled in the Community Law in Israel on the Pattern of Psychiatric Hospitalizations. Int. J. Ment. Health 2012, 41, 45–59. [Google Scholar] [CrossRef]
- Lindström, M.; Lindberg, M.; Sjöström, S. Home Bittersweet Home: The Significance of Home for Occupational Transformations. Int. J. Soc. Psychiatry 2011, 57, 284–299. [Google Scholar] [CrossRef] [PubMed]
- Mak, K.Y.; Gow, L. Clinical usefulness of an aftercare worker for psychotic patients discharged from half-way houses in Hong Kong. Br. J. Psychiatry 1996, 168, 757–761. [Google Scholar] [CrossRef] [PubMed]
- McCrea, K.T.; Spravka, L. “I’m glad you asked”: Homeless clients with severe mental illness evaluate their residential care. J. Sociol. Soc. Welf. 2008, 35, 133–159. [Google Scholar]
- McDermott, S.; Bruce, J.; Muir, K.; Ramia, I.; Fisher, K.R.; Bullen, J. Reducing hospitalisation among people living with severe mental illness. Aust. Health Rev. 2016, 40, 124–128. [Google Scholar] [CrossRef] [PubMed]
- McHugo, G.J.; Bebout, R.R.; Harris, M.; Cleghorn, S.; Herring, G.; Xie, H.; Becker, D.; Drake, R.E. A randomized controlled trial of integrated versus parallel housing services for homeless adults with severe mental illness. Schizophr. Bull. 2004, 30, 969–982. [Google Scholar] [CrossRef] [PubMed]
- Meehan, T.; Stedman, T.; Robertson, S.; Drake, S.; King, R. Does Supported Accommodation Improve the Clinical and Social Outcomes for People with Severe Psychiatric Disability? The Project 300 Experience. Aust. N. Z. J. Psychiatry 2011, 45, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Middelboe, T.; Nordentoft, M.; Knudsen, H.C.; Jessen-Petersen, B. Small group homes for the long-term mentally ill. Clinical and social characteristics of the residents. Nord. J. Psychiatry 1996, 50, 297–303. [Google Scholar] [CrossRef]
- Middelboe, T. Prospective study of clinical and social outcome of stay in small group homes for people with mental illness. Br. J. Psychiatry 1997, 171, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Muir, K.; Fisher, K.R.; Dadich, A.; Abelló, D. Challenging the exclusion of people with mental illness: The Mental Health Housing and Accommodation Support Initiative (HASI). Aust. J. Soc. Issues 2008, 43, 271–290. [Google Scholar] [CrossRef]
- Muir, K.; Fisher, K.R.; Abello, D.; Dadich, A. ‘I didn’t like just sittin’ around all day’: Facilitating Social and Community Participation Among People with Mental Illness and High Levels of Psychiatric Disability. J. Soc. Policy 2010, 39, 375–391. [Google Scholar] [CrossRef]
- Nelson, G.; Hall, G.B.; Walsh-Bowers, R. A comparative evaluation of supportive apartments, group homes, and board-and-care homes for psychiatric consumer/survivors. J. Community Psychol. 1997, 25, 167–188. [Google Scholar] [CrossRef]
- Newman, S.J.; Reschovsky, J.D.; Kaneda, K.; Hendrick, A.M. The effects of independent living on persons with chronic mental illness: An assessment of the Section 8 certificate program. Milbank Q. 1994, 72, 171–198. [Google Scholar] [CrossRef] [PubMed]
- Newton Rosen, A.; Tennant, C.; Hobbs, C.L. Moving out and moving on: Some ethnographic observations of deinstitutionalization in an Australian community. Psychiatr. Rehabil. J. 2001, 25, 152–162. [Google Scholar] [CrossRef]
- Okin, R.L.; Borus, J.F.; Baer, L.; Jones, A.L. Long-term outcome of state hospital patients discharged into structured community residential settings. Psychiatr. Serv. 1995, 46, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Okin, R.L.; Pearsall, D. Patients’ perceptions of their quality of life 11 years after discharge from a state hospital. Hosp. Community Psychiatry 1993, 44, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Patterson, M.; Moniruzzaman, A.; Palepu, A.; Zabkiewicz, D.; Frankish, C.J.; Krausz, M.; Somers, J.M. Housing First improves subjective quality of life among homeless adults with mental illness: 12-month findings from a randomized controlled trial in Vancouver, British Columbia. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 1245–1259. [Google Scholar] [CrossRef] [PubMed]
- Patterson, M.L.; Moniruzzaman, A.; Somers, J.M. Community participation and belonging among formerly homeless adults with mental illness after 12 months of housing first in Vancouver, British Columbia: A randomized controlled trial. Community Ment. Health J. 2014, 50, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Pejlert, A.; Asplund, K.; Norberg, A. Towards recovery: Living in a home-like setting after the move from a hospital ward. J. Clin. Nurs. 1999, 8, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Petersen, K.; Hounsgaard, L.; Borg, T.; Nielsen, C.V. User involvement in mental health rehabilitation: A struggle for self-determination and recognition. Scand. J. Occup. Ther. 2012, 19, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Rimmerman, A.; Schnee, J.; Klein, I. Individuals with psychiatric disabilities in adult homes: Monitoring changes over time. Int. J. Rehabil. Res. 1993, 16, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Rønning, S.B.; Bjørkly, S. Residents’ experiences of relationships with nurses in community-based supported housing—A qualitative study based on Giorgi’s method of analysis and self psychology. J. Multidiscip. Healthc. 2017, 10, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.; Bjerkeset, O.; Søndenaa, E.; Antonsen, D.Ø.; Steinsbekk, A. A qualitative study of how people with severe mental illness experience living in sheltered housing with a private fully equipped apartment. BMC Psychiatry 2016, 16, 186. [Google Scholar] [CrossRef] [PubMed]
- Saavedra, J. Schizophrenia, narrative and change: Andalusian care homes as novel sociocultural context. Cult. Med. Psychiatry 2009, 33, 163–184. [Google Scholar] [CrossRef] [PubMed]
- Sakiyama, S.; Iida, J.; Minami, Y.; Kishimoto, T. Factors of good outcome after discharge from support house (engoryou) for schizophrenia. Psychiatry Clin. Neurosci. 2002, 56, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Schutt, R.K.; Seidman, L.J.; Caplan, B.; Martsinkiv, A.; Goldfinger, S.M. The role of neurocognition and social context in predicting community functioning among formerly homeless seriously mentally ill persons. Schizophr. Bull. 2007, 33, 1388–1396. [Google Scholar] [CrossRef] [PubMed]
- Seidman, L.J.; Schutt, R.K.; Caplan, B.; Tolomiczenko, G.S.; Turner, W.M.; Goldfinger, S.M. The Effect of Housing Interventions on Neuropsychological Functioning among Homeless Persons with Mental Illness. Psychiatr. Serv. 2003, 54, 905–908. [Google Scholar] [CrossRef] [PubMed]
- Shields, D.; McGuinness, J.; MacFlynn, G. Moving long-stay patients from hospital to community: Effects on mental state and social functioning. J. Ment. Health 1995, 4, 281–287. [Google Scholar] [CrossRef]
- Shu, B.C.; Lung, F.W.; Lu, Y.C.; Chase, G.A.; Pan, P. Care of patients with chronic mental illness: Comparison of home and half-way house care. Int. J. Soc. Psychiatry 2001, 47, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Siegel, C.E.; Samuels, J.; Tang, D.-I.; Berg, I.; Jones, K.; Hopper, K. Tenant Outcomes in Supported Housing and Community Residences in New York City. Psychiatr. Serv. 2006, 57, 982–991. [Google Scholar] [CrossRef] [PubMed]
- Stefancic, A.; Tsemberis, S. Housing First for Long-Term Shelter Dwellers with Psychiatric Disabilities in a Suburban County: A Four-Year Study of Housing Access and Retention. J. Prim. Prev. 2007, 28, 265–279. [Google Scholar] [CrossRef] [PubMed]
- Stergiopoulos, V.; Gozdzik, A.; Misir, V.; Skosireva, A.; Connelly, J.; Sarang, A.; Whisler, A.; Hwang, S.W.; O’Campo, P.; McKenzie, K. Effectiveness of housing first with intensive case management in an ethnically diverse sample of homeless adults with mental illness: A randomized controlled trial. PLoS ONE 2015, 10, e0130281. [Google Scholar] [CrossRef] [PubMed]
- Stergiopoulos, V.; Gozdzik, A.; O’Campo, P.; Holtby, A.R.; Jeyaratnam, J.; Tsemberis, S. Housing First: Exploring participants’ early support needs. BMC Health Serv. Res. 2014, 14, 167. [Google Scholar] [CrossRef] [PubMed]
- Trauer, T.; Farhall, J.; Newton, R.; Cheung, P. From long-stay psychiatric hospital to Community Care Unit: Evaluation at 1 year. Soc. Psychiatry Psychiatr. Epidemiol. 2001, 36, 416–419. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.; Lapidos, A.; Rosenheck, R.A.; Harpaz-Rotem, I. Longitudinal association of therapeutic alliance and clinical outcomes. Community Ment. Health J. 2013, 49, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Tsemberis, S.; Eisenberg, R.F. Pathways to Housing: Supported Housing for Street-Dwelling Homeless Individuals with Psychiatric Disabilities. Psychiatr. Serv. 2000, 51, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Tsemberis, S.J.; Moran, L.; Shinn, M.; Asmussen, S.M.; Shern, D.L. Consumer preference programs for individuals who are homeless and have psychiatric disabilities: A drop-in center and a supported housing program. Am. J. Community Psychol. 2003, 32, 305–317. [Google Scholar] [CrossRef] [PubMed]
- Valinejad, C. The use of the Repertory Grid Technique to obtain the views of residents in a continuing care setting. Ther. Communities 1997, 18, 111–122. [Google Scholar]
- Vaslamatzis, G.; Katsouyanni, K.; Markidis, M. The efficacy of a psychiatric halfway house: A study of hospital recidivism and global outcome measure. Eur. Psychiatry 1997, 12, 94–97. [Google Scholar] [CrossRef]
- Verhaeghe, N.; De Maeseneer, J.; Maes, L.; Van Heeringen, C.; Annemans, L. Health promotion in mental health care: Perceptions from patients and mental health nurses. J. Clin. Nurs. 2013, 22, 1569–1578. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.L.I.; Poulin, S.R.; Lee, S.; Davis, M.R.; Hadley, T.R. Tracking residential outcomes of supported independent living programs for persons with serious mental illness. Eval. Program Plan. 2008, 31, 416–426. [Google Scholar] [CrossRef] [PubMed]
- Wood, P.A.; Hurlburt, M.S.; Hough, R.L.; Hofstetter, C.R. Longitudinal assessment of family support among homeless mentally ill participants in a supported housing program. J. Community Psychol. 1998, 26, 327–344. [Google Scholar] [CrossRef]
- Wright, A. Identifying pious and heretical citizens in a permanent supported housing community. Care Manag. J. 2015, 16, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.G. Social Defeat in Recovery-Oriented Supported Housing: Moral Experience, Stigma, and Ideological Resistance. Cult. Med. Psychiatry 2012, 36, 660–678. [Google Scholar] [CrossRef] [PubMed]
- Yanos, P.T.; Barrow, S.M.; Tsemberis, S. Community integration in the early phase of housing among homeless persons diagnosed with severe mental illness: Successes and challenges. Community Ment. Health J. 2004, 40, 133–150. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Ito, J.; Ogawa, M. Model Project of Home-Visit Living-Skills Coaching for Individuals with Severe Mental Illness in Japan. Int. J. Ment. Health 2011, 40, 19–27. [Google Scholar] [CrossRef]
- Killaspy, H. Supported accommodation for people with mental health problems. World Psychiatry 2016, 15, 74–75. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomized trials. Ann. Intern. Med. 2010, 152, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Fixsen, D.; Grimshaw, J.M.; Eccles, M.P. Specifying and reporting complex behaviour change interventions: The need for a scientific method. Implement. Sci. 2009, 4, 40. [Google Scholar] [CrossRef] [PubMed]
- Davidson, K.W.; Goldstein, M.; Kaplan, R.M.; Kaufmann, P.G.; Knatterud, G.L.; Orleans, C.T.; Spring, B.; Trudeau, K.J.; Whitlock, E.P. Evidence-based behavioral medicine: What is it and how do we achieve it? Ann. Behav. Med. 2003, 26, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Whitlock, E.P.; Orleans, C.T.; Pender, N.; Allan, J. Evaluating primary care behavioral counseling interventions. An evidence-based approach. Am. J. Prev. Med. 2002, 22, 267–284. [Google Scholar] [CrossRef]


{kind=link}
| Reason | n |
|---|---|
| Multiple sites, with limited service descriptions | 40 |
| Mixed method design (assessed in quantitative extraction only) | 8 |
| Non-English language | 7 |
| Database studies | 4 |
| No description of supported accommodation setting | 4 |
| Paper inaccessible | 1 |
| Total | 64 |
| Domain | Completed: n (%) | Missing: n (%) |
|---|---|---|
| Staffing location | 84 (88.4%) | 11 (11.6%) |
| Level of support | 86 (90.5%) | 9 (9.5%) |
| Recovery | 66 (69.5%) | 29 (30.5%) |
| Move-on | 79 (83.2%) | 16 (16.8%) |
| Physical setting | 87 (91.6%) | 8 (8.4%) |
| Service Type | Initial Model: n (%) | Amended Model: n (%) |
|---|---|---|
| Type 1 | 6 (6.3%) | 22 (23.2%) |
| Type 2 | 11 (11.6%) | 13 (13.7%) |
| Type 3 | 0 (0.0%) | 3 (3.2%) |
| Type 4 | 22 (23.2%) | 29 (30.5%) |
| Type 5 | 1 (1.1%) | 1 (1.1%) |
| Unable to assign type | 55 (57.9%) | 27 (28.4%) |
| Total | 95 (100.0%) | 95 (100.0%) |
| Domain | Sub-Domain | Completed (%) | Missing (%) |
|---|---|---|---|
| Duration | Duration of tenure | 80 (84.2%) | 15 (15.8%) |
| Patient characteristics | Level of need | 70 (73.7%) | 25 (26.3%) |
| Readiness to receive treatment | 33 (34.7%) | 62 (65.3%) | |
| Sobriety required? | 16 (16.8%) | 79 (83.2%) | |
| Subpopulations (i.e., women, dual-diagnosis) | 94 (98.9%) | 1 (1.1%) | |
| Housing characteristics | Structure (congregate vs. individual units) | 80 (84.2%) | 15 (15.8%) |
| Location (cluster vs. scattered site) | 83 (87.4%) | 12 (12.6%) | |
| Geographic proximity to mental health services | 13 (13.7%) | 82 (86.3%) | |
| Lease (i.e., held by patient or agency) | 20 (21.1%) | 75 (78.9%) | |
| Service characteristics | Staffing location (onsite vs. off-site) | 83 (87.4%) | 12 (12.6%) |
| Staffing duration | 58 (61.1%) | 37 (38.9%) | |
| Service linkage | 35 (36.8%) | 60 (63.2%) | |
| Staff qualifications (clinical vs. non-clinical) | 41 (43.2%) | 54 (56.8%) | |
| Intensity of support | 58 (61.1%) | 37 (38.9%) | |
| Service flexibility (i.e., variation in support) | 60 (63.2%) | 35 (36.8%) | |
| Patient choice in housing | 16 (16.8%) | 79 (83.2%) | |
| Shift in locus of control to patient | 29 (30.5%) | 66 (69.5%) |
| Domain | Guidance | Response Options |
|---|---|---|
| Staffing location | Are support staff based on-site (e.g., at the accommodation) or off-site? | 1. Staff on-site 2. No staff on-site |
| Level of support | Level of support should reflect frequency, nature and intensity of support (including staffing duration) and the level of service user need (e.g., for personal care, medication management). | 1. High support 2. Moderate support 3. Low support 4. No support |
| Move-on | How much emphasis is placed on service users moving to another physical setting after demonstrating clinical improvement, or after a set period of time (e.g., time-limited tenancies vs. open-ended tenancies/permanent housing)? | 1. Strong emphasis on move-on 2. Limited emphasis on move-on |
| Physical structure | Congregate setting = Shared with other mental health service users. Communal facilities. | 1. Congregate setting 2. Individual accommodation |
| Individual accommodation = Generic, independent community housing (not mental health specific) |
| Service Type | Final Model: n (%) |
|---|---|
| Type 1 | 31 (23.5%) |
| Type 2 | 19 (14.4%) |
| Type 3 | 4 (3.0%) |
| Type 4 | 39 (29.5%) |
| Type 5 | 1 (0.8%) |
| Unable to assign type | 38 (28.8%) |
| Total | 132 (100.0%) |
| Year: 1990–1999 | Year: 2000–2009 | Year: 2010–2017 | Total | |
|---|---|---|---|---|
| Classified | 29 | 34 | 31 | 94 |
| Not classified | 12 | 13 | 13 | 38 |
| Total | 41 | 47 | 44 | 132 |
| Service Type | Type 1 | Type 2 | Type 3 | Type 4 | Type 5 |
|---|---|---|---|---|---|
| Residential care (n = 4) | 3 (75.0%) | 1 (25.0%) | - | - | - |
| Supported housing (n = 17) | 1 (5.9%) | 7 (41.2%) | 9 (52.9%) | - | - |
| Floating outreach (n = 11) | - | - | 2 (18.2%) | 9 (81.8%) | - |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McPherson, P.; Krotofil, J.; Killaspy, H. What Works? Toward a New Classification System for Mental Health Supported Accommodation Services: The Simple Taxonomy for Supported Accommodation (STAX-SA). Int. J. Environ. Res. Public Health 2018, 15, 190. https://doi.org/10.3390/ijerph15020190
McPherson P, Krotofil J, Killaspy H. What Works? Toward a New Classification System for Mental Health Supported Accommodation Services: The Simple Taxonomy for Supported Accommodation (STAX-SA). International Journal of Environmental Research and Public Health. 2018; 15(2):190. https://doi.org/10.3390/ijerph15020190
Chicago/Turabian StyleMcPherson, Peter, Joanna Krotofil, and Helen Killaspy. 2018. "What Works? Toward a New Classification System for Mental Health Supported Accommodation Services: The Simple Taxonomy for Supported Accommodation (STAX-SA)" International Journal of Environmental Research and Public Health 15, no. 2: 190. https://doi.org/10.3390/ijerph15020190
APA StyleMcPherson, P., Krotofil, J., & Killaspy, H. (2018). What Works? Toward a New Classification System for Mental Health Supported Accommodation Services: The Simple Taxonomy for Supported Accommodation (STAX-SA). International Journal of Environmental Research and Public Health, 15(2), 190. https://doi.org/10.3390/ijerph15020190