Inappropriate Use of Medication by Elderly, Polymedicated, or Multipathological Patients with Chronic Diseases


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
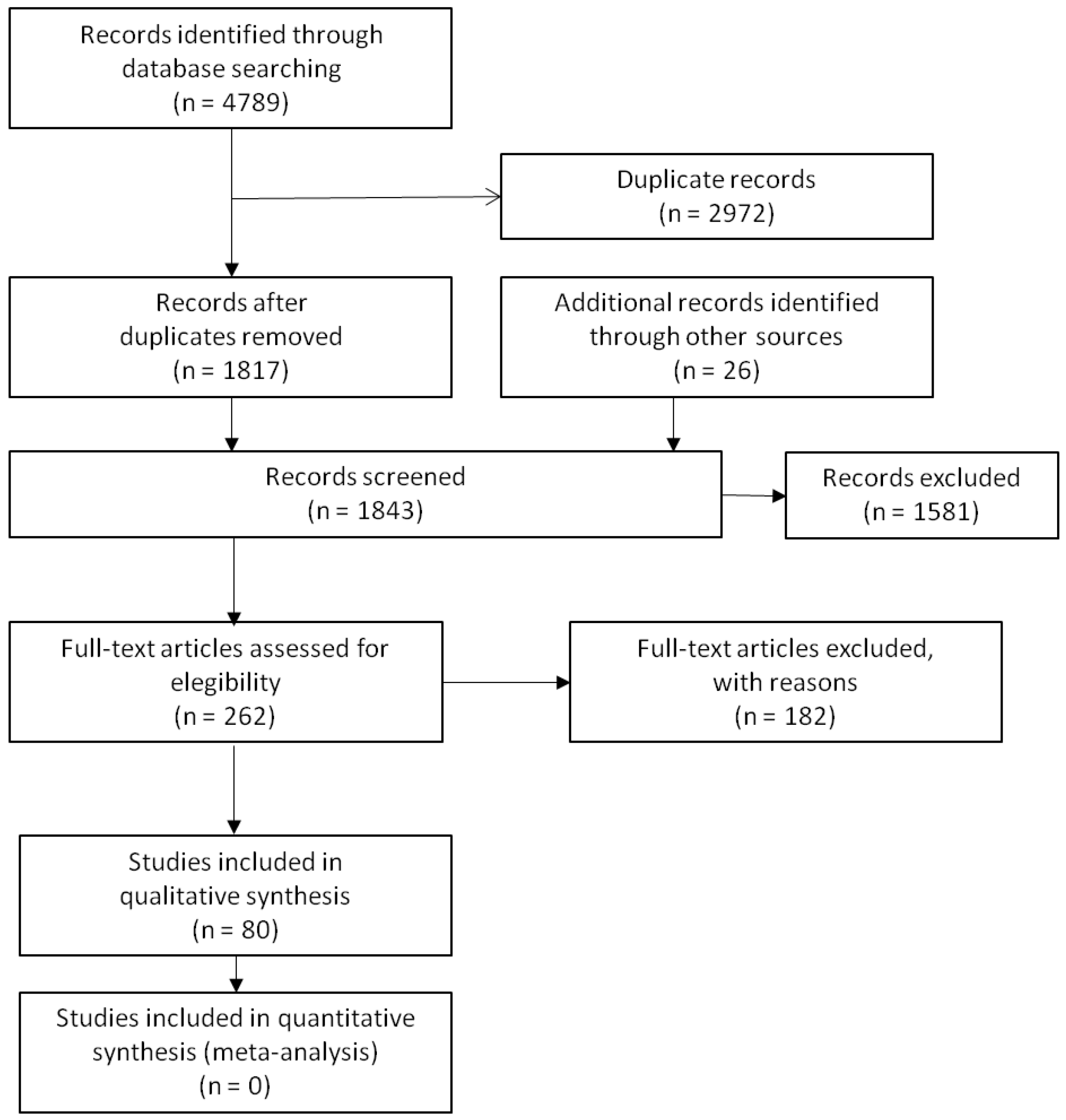
2.1. Search Strategy and Inclusion Criteria
2.2. Article Screening
2.3. Data Extraction
3. Results
3.1. Frequently Asked Questions (FAQs)
- How many elderly patients with chronic diseases take five or more medications daily?
- 2.
- What are the most common medication errors in elderly patients with chronic diseases?
- 3.
- To what extent do elderly patients taking five or more daily medications understand what they are taking and why?
- 4.
- What level of treatment adherence do elderly patients with chronic diseases have?
- 5.
- What tricks do patients use to remember to take their medication?
- 6.
- Are pill organisers useful?
- 7.
- Is it more difficult for elderly patients to understand written information, for example the information leaflets for medicines?
- 8.
- How many patients have doubts or want to ask their doctor something about their medication?
3.2. Recommendations
3.3. Possible Limitations
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Lavan, A.H.; Gallagher, P.F.; O’Mahony, D. Methods to reduce prescribing errors in elderly patients with multimorbidity. Clin. Interv. Aging 2016, 11, 857–866. [Google Scholar] [PubMed]
- Koper, D.; Kamenski, G.; Flamm, M.; Böhmdorfer, B.; Sönnichsen, A. Frequency of medication errors in primary care patients with polypharmacy. Fam. Pract. 2013, 30, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Lavon, O.; Ben-Zeev, A.; Benturi, Y. Medication Errors outside Healthcare Facilities: A National Poison Centre Perspective. Basic Clin. Pharmacol. Toxicol. 2014, 114, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Mira, J.J.; Lorenzo, S.; Guilabert, M.; Navarro, I.; Pérez-Jover, V. A systematic review of patient medication error on self-administering medication at home. Expert Opin. Drug Saf. 2015, 14, 815–838. [Google Scholar] [CrossRef] [PubMed]
- Summer Meranius, M.; Engstrom, G. Experience of self-management of medications among older people with multimorbidity. J. Clin. Nurs. 2015, 24, 2757–2764. [Google Scholar] [CrossRef] [PubMed]
- Escamilla, J.A.; Castañer, O.; Benito, S.; Ruiz, E.; Burrull, M.; Sáenz, N. Motivos de incumplimiento terapéutico en pacientes mayores polimedicados, un estudio mediante grupos focales. Aten. Primaria 2008, 40, 81–85. [Google Scholar] [CrossRef]
- Ose, D.; Mahler, C.; Vogel, I.; Ludt, S.; Szecsenyi, J.; Freund, T. Let’s talk about medication: Concordance in rating medication adherence among multimorbid patients and their general practitioners. Patient Prefer. Adherence 2012, 6, 839–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mira, J.J. Pacientes por la seguridad de los pacientes. El papel del paciente en la seguridad de los pacientes. Med. Prev. 2011, XVI, 5–11. [Google Scholar]
- Al Mahdy, H.; Seymour, D.G. How much can elderly patients tell us about their medications? Postgrad. Med. J. 1990, 66, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Metlay, J.P.; Cohen, A.; Polsky, D.; Kimmel, S.E.; Koppel, R.; Hennessy, S. Medication Safety in Older Adults: Home-Based Practice Patterns. J. Am. Geriatr. Soc. 2005, 53, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, L.; Stokes, J.A.; Purdie, D.M.; Woodward, M.; Roberts, M. Medication management at home: Medication-related risk factors associated with poor health outcomes. Age Ageing 2005, 34, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Haynes, R.B.; Montague, P.; Oliver, T.; McKibbon, K.A.; Brouwers, M.C.; Kanani, R. Interventions for helping patients to follow prescriptions for medications. Cochrane Database Syst. Rev. 2000, 2, 7–9. [Google Scholar]
- Harbour, R.; Miller, J. A new system for grading recommendations in evidence based guidelines. BJM Br. Med. J. 2001, 323, 334–336. [Google Scholar] [CrossRef]
- World Health Organization; United Nations Population Fund. Ageing in the Twenty-First Century: A Celebration and a Challenge; United Nations Population Fund: New York, NY, USA, 2012. [Google Scholar]
- Fulton, M.M.; Allen, E.R. Polypharmacy in the elderly: A literature review. J. Am. Acad. Nurse Pract. 2005, 17, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Diz-Lois, F.; Fernández, O.; Pérez, C. El paciente polimedicado. Galicia Clin. 2012, 73, S37–S41. [Google Scholar] [CrossRef] [PubMed]
- Lizano-Díez, I.; Modamio, P.; López-Calahorra, P.; Lastra, C.F.; Gilabert-Perramon, A.; Segú, J.L.; Mariño, E.L. Profile, cost and pattern of prescriptions for polymedicated patients in Catalonia, Spain. BMJ Open 2013, 3, e003963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williamson, E.M. Interactions between herbal and conventional medicines. Expert Opin. Drug Saf. 2005, 4, 355–378. [Google Scholar] [CrossRef] [PubMed]
- Meredith, S.; Feldman, P.H.; Frey, D.; Hall, K.; Arnold, K.; Brown, N.J.; Ray, W.A. Possible medication errors in home healthcare patients. J. Am. Geriatr. Soc. 2001, 49, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Gurwitz, J.H.; Field, T.S.; Harrold, L.R.; Rothschild, J.; Debellis, K.; Seger, A.; Cadoret, C.; Fish, L.S.; Garber, L.; Kelleher, M.; et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA 2003, 289, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Salvi, F.; Marchetti, A.; D’Angelo, F.; Boemi, M.; Lattanzio, F.; Cherubini, A. Adverse drug events as a cause of hospitalization in older adults. Drug Saf. 2012, 35, 29–45. [Google Scholar] [CrossRef] [PubMed]
- Fernández Lisón, L.C.; Barón Franco, B.; Vázquez Domínguez, B.; Martínez García, T.; Urendes Haro, J.J.; Pujol de la Llave, E. Errores de medicación e incumplimiento terapéutico en ancianos polimedicados. Farm. Hosp. 2006, 30, 280–283. [Google Scholar] [CrossRef]
- Otero, M.J.; Codina, C.; Tamés, M.J.; Pérez, M. Errores de medicación: Estandarización de la terminología y clasificación. Farm. Hosp. 2003, 27, 137–149. [Google Scholar]
- Pérula de Torres, L.A.; Pulido Ortega, L.; Pérula de Torres, C.; González Lama, J.; Olaya Caro, I.; Ruiz Moral, R.; Grupo corporativo Estudio ATEM-AP. Efficacy of motivational interviewing for reducing medication errors in chronic patients over 65 years with polypharmacy: Results of a cluster randomized trial. Med. Clin. 2014, 143, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Leal, M.; Abellán, J.; Casa, M.T.; Martínez, J. Paciente polimedicado: ¿conoce la posología de la medicación?, ¿afirma tomarla correctamente? Aten. Primaria 2004, 33, 451–456. [Google Scholar] [CrossRef]
- Wimmer, B.C.; Johnell, K.; Fastbom, J.; Wiese, M.D.; Bell, J.S. Factors associated with medication regimen complexity in older people: A cross-sectional population-based study. Eur. J. Clin. Pharmacol. 2015, 71, 1099–1108. [Google Scholar] [CrossRef] [PubMed]
- Molina, T.; Caraballo, M.O.; Palma, D.; López, S.; Domínguez, J.C.; Morales, J.C. Prevalencia de polimedicación y riesgo vascular en la población mayor de 65 años. Aten. Primaria 2012, 44, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Mira, J.J.; Martínez-Jimeno, L.; Orozco-Beltran, D.; Iglesias-Alonso, F.; Lorenzo, S.; Nuño, R.; Pérez, P.; Toro, N.; Pérez-Jover, V.; Gil-Guillen, V. What older complex chronic patients need know about the medication they take every day for a safe drug use. Expert Opin. Drug Saf. 2014, 13, 713–721. [Google Scholar] [PubMed]
- Akici, A.; Kalaça, S.; Uğurlu, M.U.; Toklu, H.Z.; Iskender, E.; Oktay, S. Patient knowledge about drugs prescribed at primary healthcare facilities. Pharmacoepidemiol. Drug Saf. 2004, 13, 871–876. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Adherence Long Term Therapies. 2003. Available online: http://www.paho.org/hq/index.php?option=com_docman&task=doc_view&gid=18722&Itemid=270&lang=en (accessed on 16 November 2017).
- Morales, M.T. Estudio sobre la utilidad del pastillero para mejorar el cumplimiento terapéutico. Aten. Primaria 2009, 41, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Márquez-Contreras, E.; de la Figuera-Von Wichmann, M.; Franch-Nadal, J.; Llisterri-Caro, J.L.; Gil-Guillén, V.; Martín-de Pablos, J.L.; Casado-Martínez, J.J.; Martell-Claros, N. Do Patients with High Vascular Risk Take Antihypertensive Medication Correctly? Cumple-MEMS Study. Rev. Esp. Cardiol. 2012, 65, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Gray, S.L.; Mahoney, J.E.; Blough, D.K. Medication adherence in elderly patients receiving home health services following hospital discharge. Ann. Pharmacother. 2001, 35, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Proupín, N.; Aparicio, M.; Garea, P.; Segade, X.; Arceo, A.; López, L. Polimedicación en pacientes adultos con dolencias crónicas en un centro de salud. Cad. Aten. Primaria 2008, 15, 275–279. [Google Scholar]
- Fuster, V. Un problema alarmante en prevención secundaria: Bajo cumplimiento (estilo de vida) y baja adherencia (farmacológica). Rev. Esp. Cardiol. 2012, 65, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Aronson, J.K. Medication errors resulting from the confusion of drug names. Expert Opin. Drug Saf. 2004, 3, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Van Eijken, M.; Tsang, S.; Wensing, M.; de Smet, P.A.; Grol, R.P. Interventions to improve medication compliance in older patients living in the community: A systematic review of the literature. Drugs Aging 2003, 20, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Vik, S.A.; Maxwell, C.J.; Hogan, D.B. Measurement, Correlates, and Health Outcomes of Medication Adherence among seniors. Ann. Pharmacother. 2004, 38, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Crespillo-García, E.; Rivas-Ruiz, F.; Contreras, E.; Castellano, P.; Suárez, G.; Pérez-Tobar, E. Conocimientos, percepciones y actitudes que intervienen en la adherencia al tratamiento en pacientes ancianos polimedicados desde una perspectiva cualitativa. Rev. Calid. Asist. 2013, 28, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Gellad, W.F.; Grenard, J.L.; Marcum, Z.A. A Systematic Review of Barriers to Medication Adherence in the Elderly: Looking Beyond Cost and Regimen Complexity. Am. J. Geriatr. Pharmacother. 2011, 9, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Midlöv, P.; Holmdahl, L.; Eriksson, T.; Bergkvist, A.; Ljungberg, B.; Widner, H.; Nerbrand, C.; Höglund, P. Medication report reduces number of medication errors when elderly patients are discharged from hospital. Pharm. World Sci. 2008, 30, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Haynes, R.B.; Taylor, D.W.; Sackett, D.L.; Gibson, E.S.; Bernholz, C.D.; Mukherjee, J. Can simple clinical measurements detect patient noncompliance? Hypertension 1980, 2, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Branin, J.J. The role of memory strategies in medication adherence among the elderly. Home Health Care Serv. Q. 2001, 20, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Raehl, C.L.; Bond, C.A.; Woods, T.; Patry, R.A.; Sleeper, R.B. Individualized drug use assessment in the elderly. Pharmacotherapy 2002, 22, 1239–1248. [Google Scholar] [CrossRef] [PubMed]
- Tseng, M.H.; Wu, H.C. A cloud medication safety support system using QR code and Web services for elderly outpatients. Technol. Health Care 2014, 22, 99–113. [Google Scholar] [PubMed]
- Carrillo, I.; Guilabert, M.; Pérez-Jover, V.; Mira, J.J. Valoración de dos aplicaciones para la autogestión de la medicación en pacientes mayores. Estudio cualitativo. Rev. Calid. Asist. 2015, 30, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Mira, J.J.; Guilabert, M.; Carrillo, I.; Fernández, C.; Vicente, M.A.; Orozco, D.; Gil-Guillen, V. Use of QR and EAN-13 codes by older patients taking multiple medications for a safer use of medication. Int. J. Med. Inf. 2015, 84, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Serra-Prat, M.; Bartolomé, M.; Fité, B.; Agustí, C. Eficacia de un sistema personalizado de dosificación (SPD) en la mejoría del cumplimiento terapéutico en ancianos polimedicados. Aten. Primaria 2006, 37, 524–526. [Google Scholar] [CrossRef] [PubMed]
- Llaves, E.; Segura, M.M.; García-Jiménez, E.; Baena, I. Sistemas personalizados de dosificación en el cumplimiento del tratamiento farmacológico de pacientes con hipertensión y dislipemias. Aten. Primaria 2009, 41, 472–473. [Google Scholar] [CrossRef] [PubMed]
- Mira, J.J.; Navarro, I.; Botella, F.; Borrás, F.; Nuño-Solinís, R.; Orozco, D.; Iglesias-Alonso, F.; Pérez-Pérez, P.; Lorenzo, S.; Toro, N. A Spanish pillbox app for elderly patients taking multiple medications: Randomized controlled trial. J. Med. Internet Res. 2014, 16, e99. [Google Scholar] [CrossRef] [PubMed]
- Burda, C.; Haack, M.; Duarte, A.C.; Alemi, F. Medication adherence among homeless patients: A pilot study of cell phone effectiveness. J. Am. Acad. Nurse Pract. 2012, 24, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Morak, J.; Schwarz, M.; Hayn, D.; Schreier, G. Feasibility of mHealth and Near Field Communication technology based medication adherence monitoring. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2012, 2012, 272–275. [Google Scholar] [PubMed]
- Hayakawa, M.; Uchimura, Y.; Omae, K.; Waki, K.; Fujita, H.; Ohe, K. A Smartphone-based Medication Self-management System with Realtime Medication Monitoring. Appl. Clin. Inf. 2013, 4, 37–52. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.H.; Liu, J.W.S. Intelligent Tools for Reducing Medication Dispensing and Administration Error. In Foundations of Health Information Engineering and Systems; Gibbons, J., MacCaull, W., Eds.; FHIES 2013, Lecture Notes in Computer Science; Springer: Berlin/Heidelberg, Germany, 2014; Volume 8315. [Google Scholar]
- Årsand, E.; Frøisland, D.H.; Skrøvseth, S.O.; Chomutare, T.; Tatara, N.; Hartvigsen, G.; Tufano, J.T. Mobile health applications to assist patients with diabetes: Lessons learned and design implications. J. Diabetes Sci. Technol. 2012, 6, 1197–1206. [Google Scholar] [CrossRef] [PubMed]
- Dayer, L.; Heldenbrand, S.; Anderson, P.; Gubbins, P.O.; Martin, B.C. Smartphone medication adherence apps: Potential benefits to patients and providers. J. Am. Pharm. Assoc. 2013, 53, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Feldman-Stewart, D.; Brundage, M.D.; McConell, B.A. Practical issues in assisting shared decision-making. Health Expect 2000, 3, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Mira, J.J.; Rodríguez-Marín, J. Análisis de las condiciones en las que los pacientes toman decisiones responsables. Med. Clín. 2001, 116, 104–110. [Google Scholar] [CrossRef]
- Dickinson, D.; Raynor, D.K. What information do patients need about drugs? Ask the patients: It may be more than you think. Br. Med. J. 2003, 327, 861. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Tizán, L.; Soto, J.; Peiró, S. La satisfacción con el tratamiento. Aten. Primaria 2009, 41, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Entwistle, V.A.; Watts, I.S. Disseminating information about health care effectiveness: A survey of consumer health information services. Q. Health Care 1998, 7, 124–129. [Google Scholar] [CrossRef]
- Kenny, T.; Wilson, R.G.; Purves, I.N.; Clark, J.; Newton, L.D.; Moseley, D.V. A PIL for every ill? Patient information leaflets (PILs): A review of past, present and future use. Fam. Pract. 1998, 15, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Moult, B.; Franck, L.; Brady, H. EQI: Development and preliminary validation of a new instrument to improve the quality of written health care information. Health Expect 2004, 7, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Grime, J.; Blenkinsopp, A.; Raynor, D.K.; Pollock, K.; Knapp, P. The role and value of written information for patients about individual medicines: A systematic review. Health Expect 2007, 10, 286–298. [Google Scholar] [CrossRef] [PubMed]
- Hirsh, D.; Clerehan, R.; Staples, M.; Osborne, R.; Buchbinder, R. Patient assessment of medication information leaflets and validation of the evaluative linguistic framework (ELF). Patient Educ. Couns. 2009, 77, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Raynor, D.K.; Blenkinsopp, A.; Knapp, P.; Grime, J.; Nicolson, D.J.; Pollock, K.; Dorer, G.; Gilbody, S.; Dickinson, D.; Maule, A.J.; et al. A systematic review of quantitative research on the role and effectiveness of written information available to patients about individual medicines. Health Technol. Assess. 2007, 11, 1–160. [Google Scholar] [CrossRef]
- Chubaty, A.; SadowskiCh, C.A. Typeface legibility of patient information leaflets intended for community-dwelling seniors. Age Ageing 2009, 38, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Nicolson, D.; Knapp, P.; Raynor, D.K.; Spoor, P. Written information about individual medicines for consumers. Cochrane Databases Syst. Rev. 2009, 2, CD002104. [Google Scholar] [CrossRef] [PubMed]
- Mira, J.J.; Lorenzo, S.; Pérez-Jover, V.; Navarro, I.; Martín de Rosales, A.; Lara, C. Assessment of the quality of medication information for patients in Spain. Expert Opin. Drug Saf. 2013, 12, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Mira, J.J.; Navarro, I.M.; Nuño, R. Patient Safety in Blogs and Wikis Entries by Patients and For Patients. J. Health Med. Inf. 2014, 5, 172. [Google Scholar]
- Charnock, D.; Shepperd, S.; Needham, G.; Gann, R. DISCERN: An instrument for judging the quality of written consumer health information on treatment choices. J. Epidemiol. Commun. Health 1999, 53, 105–111. [Google Scholar] [CrossRef]
- Svarstad, B.L.; Mount, J.K.; Tabak, E.R. Expert and consumer evaluation of patient medication leaflets provided in US pharmacies. J. Am. Pharm. Assoc. 2003, 45, 443–451. [Google Scholar] [CrossRef]
- Kirksey, O.; Harper, K.; Thompson, S.; Pringle, M. Assessment of selected patient educational materials of various chain pharmacies. J. Health Commun. 2004, 9, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Ballesteros-Peña, S.; Fernández-Aedo, I. Análisis de la legibilidad lingüística de los prospectos de los medicamentos mediante el índice de Flesch-Szigriszt y la escala Inflesz. An. Sist. Sanit. Navar. 2013, 36, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Basara, L.R.; Juergens, J.P. Patient package insert readability and design. Am. Pharm. 1994, 34, 48–53. [Google Scholar] [CrossRef]
- Lewis, M.A.; Newton, J.T. An evaluation of the quality of commercially produced patient information leaflets. Br. Dent. J. 2006, 201, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Barrio-Cantalejo, I.M.; Simón-Lorda, P. ¿Pueden leer los pacientes lo que pretendemos que lean? Un análisis de la legibilidad de materiales escritos de educación para la salud. Aten. Primaria 2003, 31, 409–414. [Google Scholar] [CrossRef]
- March, J.C.; Prieto, M.A.; Ruiz, A.; Simón, P.; Barrio, I.; Danet, A. Mejora de la información sanitaria contenida en prospectos de los medicamentos: Expectativas de pacientes y de profesionales sanitarios. Aten. Primaria 2010, 42, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Mira, J.J.; Carrillo, I.; Navarro, I.M.; Orozco, D.; Gil, V.; Guilabert, M. Efectos de la edad y de la formación académica en la comprensión de la información escrita que entregamos habitualmente a nuestros pacientes. Aten. Primaria 2015, 47, 126–127. [Google Scholar] [CrossRef] [PubMed]
- Mira, J.J.; Rodríguez-Marín, J.; Peset, R.; Ybarra, J.; Pérez-Jover, V.; Palazón, I.; Llorca, E. Causas de satisfacción y de insatisfacción de los pacientes en hospitales y atención primaria. Rev. Calid. Asist. 2002, 17, 273–283. [Google Scholar] [CrossRef]
- Davison, J.; Degner, L.; Morgan, T. Information and decision-making preferences of men with prostate cancer. Oncol. Nurs. Forum 1995, 22, 1401–1408. [Google Scholar] [PubMed]
- Sculper, M.J.; Dwyer, N.; Browing, J.; Horsley, S.; Cullimore, J. A survey of women’s preferences regarding alternative surgical treatments for menorrhagia. Health Expect. 1998, 1, 96–105. [Google Scholar] [CrossRef]
- Ashbury, F.; Findlay, H.; Reynolds, B.; McKerracher, K. A Canadian survey of cancer patients’ experiences: Are their needs being met? J. Pain Symptom Manag. 1998, 16, 298–306. [Google Scholar] [CrossRef]
- Mira, J.J.; Guilabert, M.; Pérez-Jover, V.; Lorenzo, S. Barriers for an effective communication around clinical decision making: An analysis of the gaps between doctors’ and patients’ point of view. Health Expect. 2014, 17, 826–839. [Google Scholar] [CrossRef] [PubMed]
- Barca, I.; Parejo, R.; Gutiérrez, P.; Fernández, F.; Alejandre, G.; López, F. La información al paciente y su participación en la toma de decisiones clínicas. Aten. Primaria 2004, 3, 361–367. [Google Scholar] [CrossRef]
- Mira, J.J.; Nebot, C.; Lorenzo, S.; Pérez-Jover, V. Patient report on information given, consultation time and safety in primary care. Q. Saf. Health Care 2010, 19, 1–4. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Main Topic (n) | Country (n) | Evidence Levels * (n) |
|---|---|---|
| Adverse Drugs Events (7) | Canada (1) | |
| Italy (1) | 2++ B (2) | |
| United Kingdom (1) | 2+ C (4) | |
| USA (2) | ||
| Spain (2) | ||
| Medication Adherence and Misuse (12) | Austria (1) | 2++ B (2) |
| Canada (1) | 2+ B (1) | |
| Germany (1) | 2+ C (6) | |
| Spain (4) | 2− C (1) | |
| The Netherlands (1) | 4 D (2) | |
| USA (4) | ||
| Medication Errors (13) | Austria (1) | 2++ B (3) |
| Ireland (1) | 2+ B (1) | |
| Israel (1) | 2+ C (6) | |
| United Kingdom (1) | 2− C (2) | |
| USA (2) | 3 D (1) | |
| Spain (6) | ||
| Sweden (1) | ||
| Medication Management (12) | Australia (2) | 1− B (1) |
| USA (3) | 2+ B (1) | |
| Spain (6) | 2+ C (6) | |
| Tokyo (1) | 2− C (2) | |
| 4 D (2) | ||
| Medication Safety Information (20) | Australia (1) | 4 D (6) |
| Canada (2) | 2++ B (2) | |
| United Kingdom (7) | 2+ B (2) | |
| USA (5) | 2+ C (5) | |
| Spain (5) | 2− C (5) | |
| Medication Safety Tools (9) | Norway (1) | 2++ B (1) |
| USA (3) | 2+ C (3) | |
| Spain (2) | 2− C (2) | |
| Taiwan (2) | 3 D (2) | |
| United Kingdom (1) | 4 D (1) | |
| Patient Medication Knowledge (7) | Hong Kong (1) | |
| Spain (2) | 2++ B (2) | |
| Turkey (1) | 2+ C (3) | |
| United Kingdom (1) | 2− C (2) | |
| USA (2) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Jover, V.; Mira, J.J.; Carratala-Munuera, C.; Gil-Guillen, V.F.; Basora, J.; López-Pineda, A.; Orozco-Beltrán, D. Inappropriate Use of Medication by Elderly, Polymedicated, or Multipathological Patients with Chronic Diseases. Int. J. Environ. Res. Public Health 2018, 15, 310. https://doi.org/10.3390/ijerph15020310
Pérez-Jover V, Mira JJ, Carratala-Munuera C, Gil-Guillen VF, Basora J, López-Pineda A, Orozco-Beltrán D. Inappropriate Use of Medication by Elderly, Polymedicated, or Multipathological Patients with Chronic Diseases. International Journal of Environmental Research and Public Health. 2018; 15(2):310. https://doi.org/10.3390/ijerph15020310
Chicago/Turabian StylePérez-Jover, Virtudes, José J. Mira, Concepción Carratala-Munuera, Vicente F. Gil-Guillen, Josep Basora, Adriana López-Pineda, and Domingo Orozco-Beltrán. 2018. "Inappropriate Use of Medication by Elderly, Polymedicated, or Multipathological Patients with Chronic Diseases" International Journal of Environmental Research and Public Health 15, no. 2: 310. https://doi.org/10.3390/ijerph15020310
APA StylePérez-Jover, V., Mira, J. J., Carratala-Munuera, C., Gil-Guillen, V. F., Basora, J., López-Pineda, A., & Orozco-Beltrán, D. (2018). Inappropriate Use of Medication by Elderly, Polymedicated, or Multipathological Patients with Chronic Diseases. International Journal of Environmental Research and Public Health, 15(2), 310. https://doi.org/10.3390/ijerph15020310