Disaster Reintegration Model: A Qualitative Analysis on Developing Korean Disaster Mental Health Support Model


Abstract
:1. Introduction
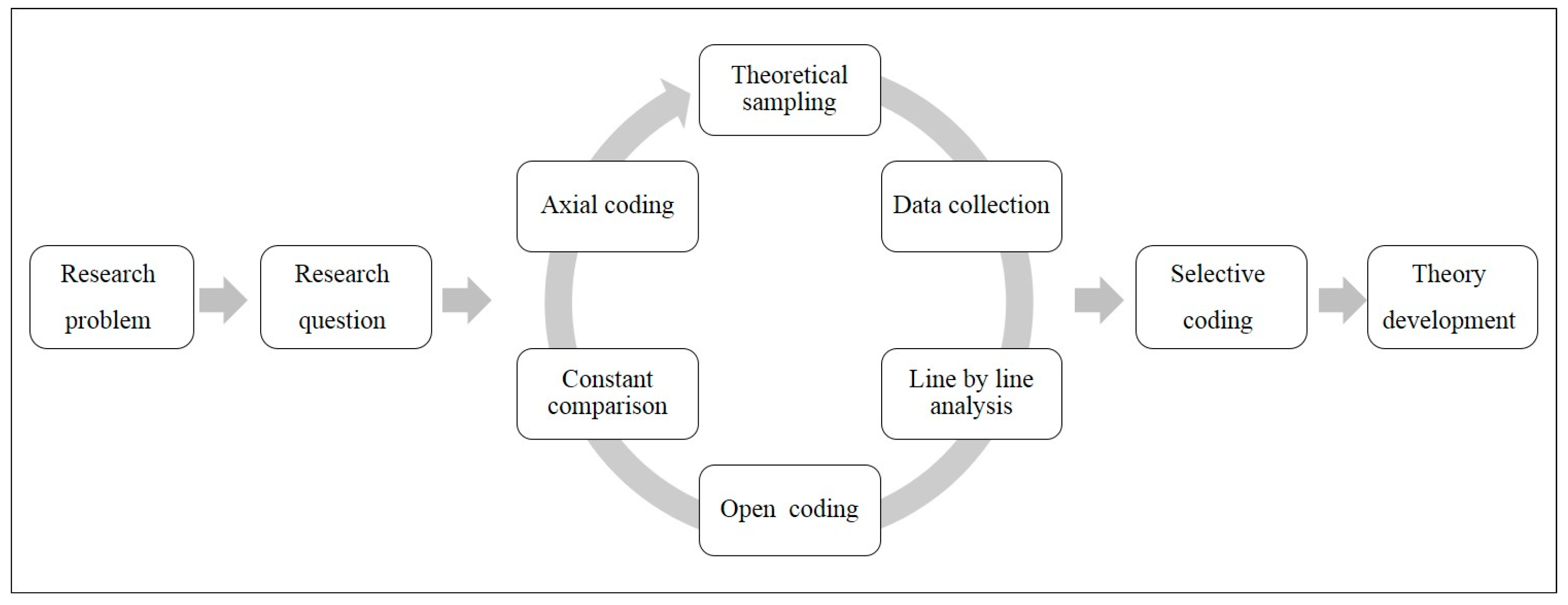
2. Materials and Methods
Ethical Approval
3. Results
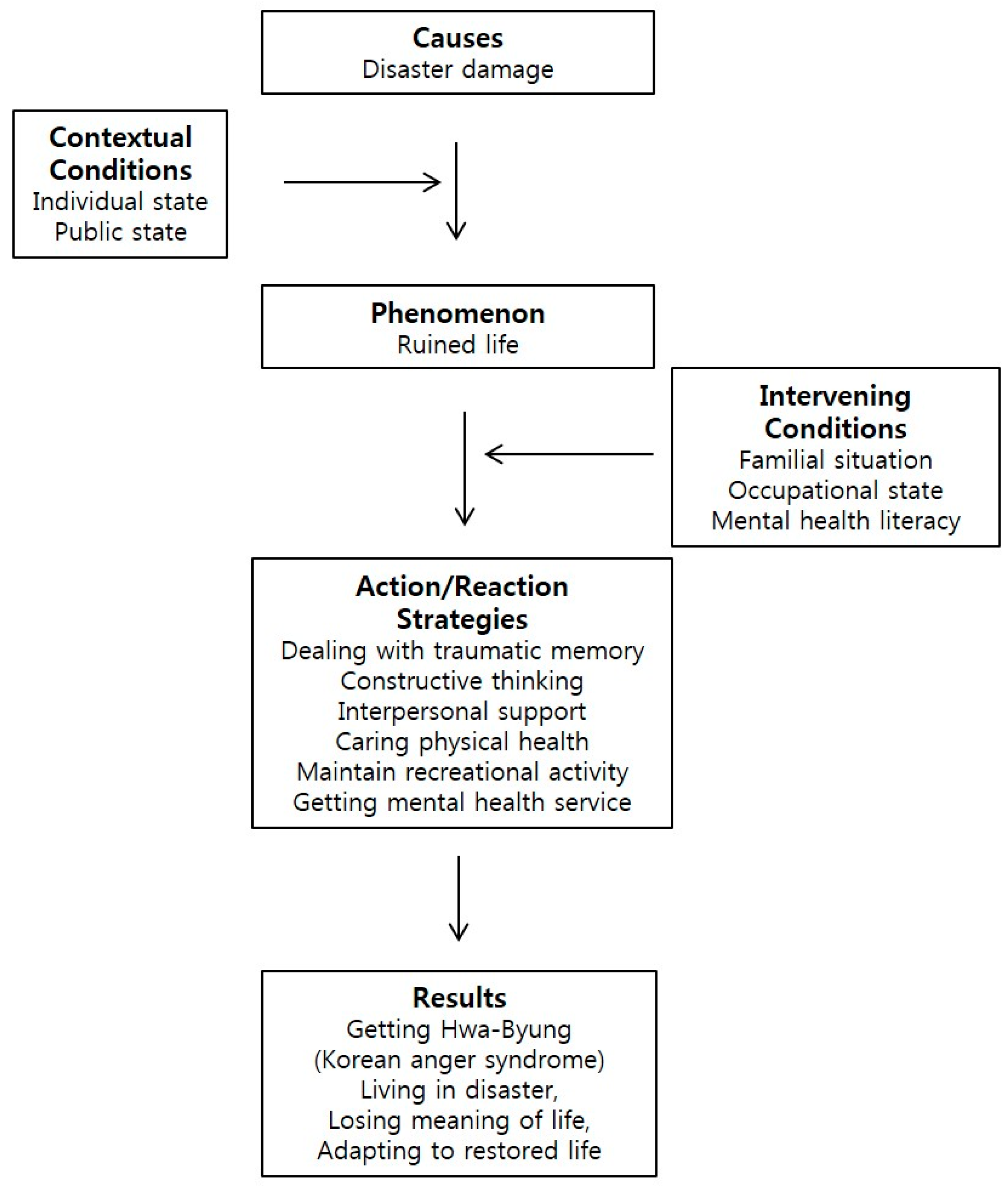
3.1. Results from Open and Axial Coding
3.1.1. Causal Conditions of the Disaster Survivors’ Mental Health Problems
“The liquidation dam had collapsed. Yeah and there’s a backflow here. At that time, two people died in B-dong and three people including Kim were dead. One was swept in the water and one died in an electric shock…”(Case 8)
“I was hit by a fire but the fire accident caused a liquefied petroleum gas explosion. Oh, that’s when the explosion happened and suddenly something happened at that time. I was so embarrassed that I did not know what to do…”(Case 2)
“The feeling that the car itself rolls like this. Because I bumped too much from the back, I was just stuck against it at a speed of 80–90 km/h. So, I was frozen still and in shock, so shaken now, all the junk in the car bounces out as it shakes…”(Case 14)
3.1.2. Contextual Conditions of the Disaster Survivors’ Mental Health Problems
“If it rained, it would be immersed in water. No matter how much it recovered, it was useless and helpless.”(Case 5)
“I was hospitalized at the hospital with burns on my arms and legs, the pain was so severe that I could not tell.”(Case 2)
“I went on a motorcycle and turned left and I ran into a car making a U-turn. I just rolled up and fell back like this. My neck was broken and my hands and feet were swollen by the shock but my feet were walking fast but my hands were so swollen that I could not touch them.”(Case 15)
“If you give me a chance by economic support to recover quickly, or if you give me a chance to recover soon, I will be better off.”(Case 13)
3.1.3. Phenomenon of the Disaster Survivors’ Mental Health Problems
“After recovery, I came back home and I was in a state of being involved with the dirt all over the house. It was so terrible. Oh, now, one by one, now my hard work was broken that I had built throughout my life and it feels like it’s collapsing; how do I do this? I feel like I have lost a lot.”(Case 4)
“No, I want to die even if I live, I just do not want to live...I just want to die. I have no idea. Yes. I do not have anyone in my ears. I cannot express the real condition that I faced…”(Case 1)
“At that time, I could not think of anything at the time. Just because I was flooded, I just cried and was blowing, so I fell asleep and cried like hell. At that time, I could not think to ask for help.”(Case 11)
3.1.4. Intervening Conditions of the Disaster Survivors’ Mental Health Problems
“I think I should save my child. Because I am a mother. The damage was huge. And should we do this again? But it was because things started out so hard but I am a mother and I have to live…”(Case 10)
“There is a limit to outsiders’ ability to help and they are busy too. So, first of all, family members gave a lot of help, primarily when things were so bad.”(Case 9)
“I stopped receiving medical treatment because I felt the gaze of my colleagues when I visited the hospital, even though I should be treated after the flooding.”(Case 6)
“I do not know where to go for psychological treatment or something like this but at home and outpatient treatment, so to speak, I would say it is a folk remedy, so I tried to do something like that.”(Case 2)
3.1.5. Action/reaction Strategies of the Disaster Survivors’ Mental Health Problems
“Now, I start driving and praying…Sometimes when the car changes next to the lane, it also jumps slightly. Every time I say to myself...I’m fine, I am much better and now I’m okay. I am safe. I always keep talking to myself like this.”(Case 14)
“I exercise a lot. Before exercising in the morning, I run for 1 hour. Exercise reduces sick days and decreases the number of times I go to the hospital. That’s why I like exercise.”(Case 3)
“Because I went on without quitting my job, I forgot about the accident. I think that the mental suffering was a little less because my colleagues and I have been working this way now…”(Case 2)
“Actually, we are helping each other and living comfortably with the neighbors. If you live with each other in a spirit of cooperation, it seems that you can overcome many problems.”(Case 7)
3.1.6. Results of the Disaster Survivors’ Mental Health Problems
“When it rains, I become anxious now. I cannot go far away. I wonder what would happen if I went there. If something goes away when you’re far away, that’s it”.(Case 10)
“Every time I see a scar, the pain of the time comes up, I hate to meet people. I just think I do not want to live like this”.(Case 2)
“I’ve got Hwa-Byung. If I get nervous, the symptoms are already building inside. I cannot just breathe. If I just get sick in the abdomen, I must run to the toilet. After the flooding, my body is bad and hardi”.(Case 9)
“The most helpful strategy was to live hard. Because I should do my job. We do not want to rely on another person. It’s just living hard that is medicine”.(Case 3)
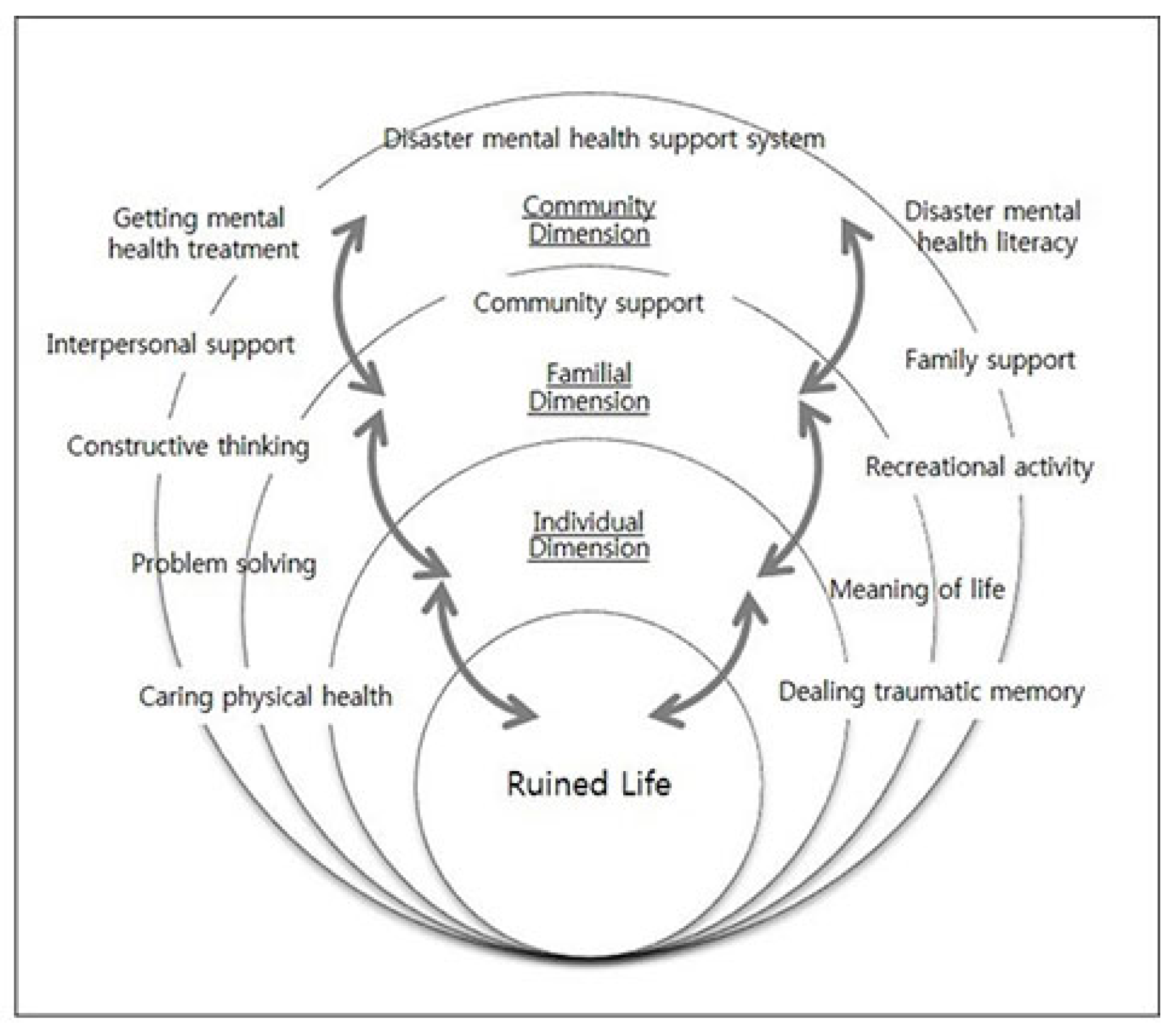
3.2. Results from Selective Coding
3.2.1. Core Category: Rebuild and Rehabilitation
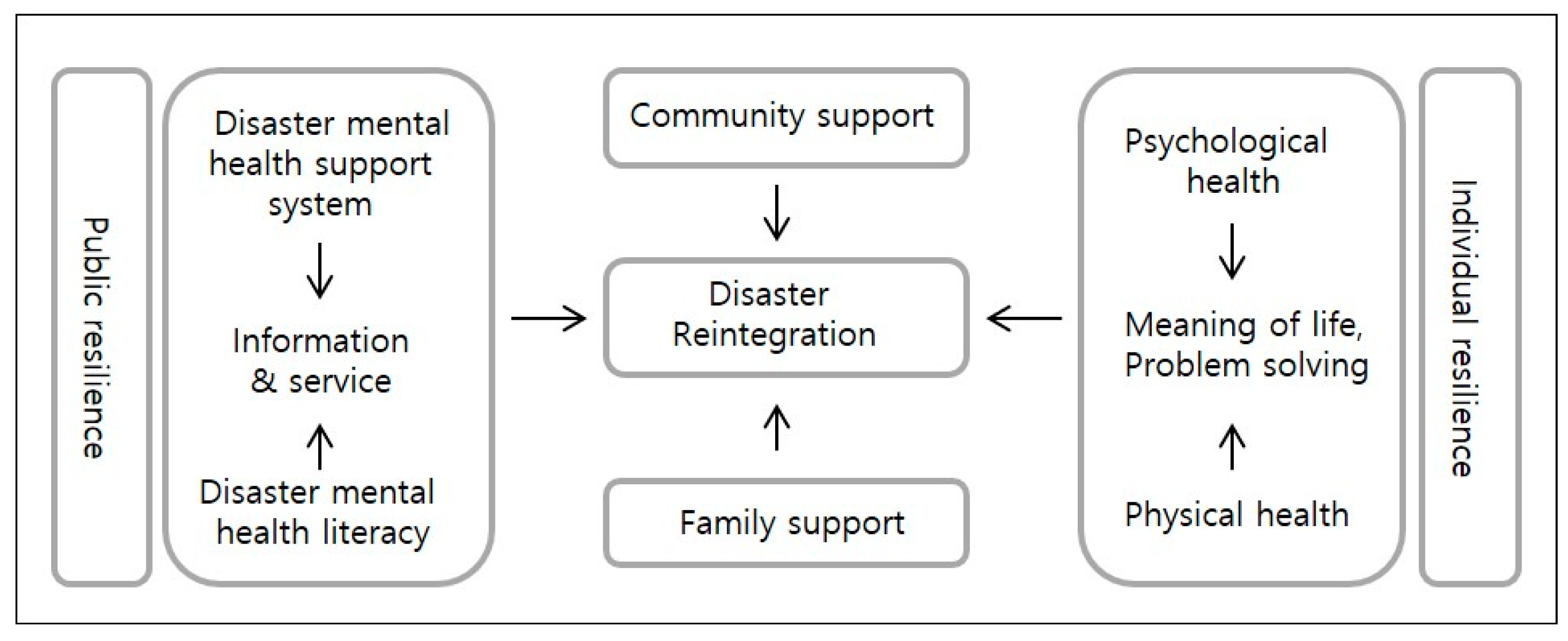
3.2.2. Conceptual Framework: Disaster Reintegration Model
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Davidson, T.M.; Price, M.; McCauley, J.L.; Ruggiero, K.J. Disaster impact across cultural groups: Comparison of Whites, African Americans, and Latinos. Am. J. Community Psychol. 2013, 52, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-S.; Ahn, J.-Y.; Kim, D.-I. Counselors’ consensus on response to national disaster -Experience of disaster counseling and needs of counselors-. Korea J. Couns. 2015, 16, 495–512. [Google Scholar]
- Lee, N.; Sim, K.; Han, S.; Lee, K.; Sim, M.; Chae, J.; Ahn, H. A qualitative content analysis of reports of mental health service providers after the Sewol Ferry Accident in Korea. Ment. Health Soc. Work 2015, 43, 116–144. [Google Scholar]
- Choi, Y.-J.; Pang, K.-Y.; Kim, S. A transcultural model of Hwa-Byung: A Grounded theory. J. Korean Acad. Psychiatr. Ment. Health Nurs. 2006, 15, 508–512. [Google Scholar]
- Choi, T.-S.; Kim, J.-H.; Lee, D.-H. A systemic approach about psycho-social interventions programs on disasters and post-traumatic stress disorder: On cultural perspective. Korean J. Cult. Arts Educ. Stud. 2014, 9, 99–118. [Google Scholar] [CrossRef]
- Lee, D.-H.; Shin, J.-Y. A study on counselors’ counseling experience participated in crisis intervention for Sewol Ferry Disaster: A phenomenological approach. Korea J. Couns. 2016, 17, 373–398. [Google Scholar]
- Wade, D.; Crompton, D.; Howard, A.; Stevens, N.; Metcalf, O.; Brymer, M.; Forbes, D. Skills for Psychological Recovery: Evaluation of a post-disaster mental health training program. Disaster Health 2015, 2, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Forbes, D.; O’Donnell, M.; Bryant, R. Psychosocial recovery following community disasters: An international collaboration. Aust. N. Z. J. Psychiatry 2016, 51, 660–662. [Google Scholar] [CrossRef] [PubMed]
- Jeong, C.-S. Disaster: Concepts and responses in Korean traditional culture from the viewpoint of analytical psychology. In Proceedings of the 2017 Conference of Korean Society for Traumatic Stress Studies, Seoul, Korea, 24 November 2017. [Google Scholar]
- Strauss, A.; Corbin, J. Basics of Qualitative Research Techniques and Procedures for Developing Grounded Theory, 2nd ed.; Sage Publications: London, UK, 1998; ISBN 13 978-0803959408. [Google Scholar]
- Choi, Y.-J. Immigrant women’s acculturation stress and coping strategies in Korea: A qualitative analysis. Int. J. Intercult. Relat. 2016, 55, 79–85. [Google Scholar] [CrossRef]
- Choi, Y.-J.; Lee, K.-J. Evidence-based nursing: Effects of a structured nursing program for the health promotion of Korean women with Hwa-Byung. Arch. Psychiatr. Nurs. 2007, 21, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Hobfoll, S.E.; Watson, P.; Bell, C.C.; Bryant, R.A.; Brymer, M.J.; Friedman, M.J.; Friedman, M.; Gersons, B.P.; de Jong, J.T.; Layne, C.M.; et al. Five essential elements of immediate and mid-term mass trauma intervention: Empirical evidence. Psychiatry 2007, 70, 283–315. [Google Scholar] [CrossRef] [PubMed]
- Dückers, M.L.A. Five essential principles of post-disaster psychosocial care: Looking back and forward with Stevan Hobfoll. Eur. J. Psychotraumatol. 2013, 4. [Google Scholar] [CrossRef] [PubMed]
- Muldoon, O.T.; Acharya, K.; Jay, S.; Adhikari, K.; Pettigrew, J.; Lowe, R.D. Community identity and collective efficacy: A social cure for traumatic stress in post-earthquake Nepal. Eur. J. Soc. Psychol. 2017, 47, 904–915. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Sex | Age (Year) | Status of Marriage | Education | No. of Disaster Experience |
|---|---|---|---|---|---|
| 1 | Female | 73 | Divorced | Middle school | 2 |
| 2 | Female | 67 | Married | High school | 1 |
| 3 | Female | 77 | Married | Middle school | 3 |
| 4 | Female | 45 | Married | University | 1 |
| 5 | Female | 76 | Bereaved | Middle school | 1 |
| 6 | Female | 81 | Bereaved | High school | 4 |
| 7 | Male | 75 | Married | Middle school | 3 |
| 8 | Female | 44 | Married | University | 2 |
| 9 | Male | 66 | Married | High school | 10 |
| 10 | Male | 57 | Married | High school | 2 |
| 11 | Female | 64 | Married | College | 5 |
| 12 | Female | 59 | Bereaved | Middle school | 1 |
| 13 | Female | 57 | Married | Middle school | 10 |
| 14 | Male | 67 | Married | High school | 10 |
| 15 | Male | 51 | Married | High school | 3 |
| 16 | Female | 37 | Single | College | 2 |
| Open Coding | Axial Coding | |
|---|---|---|
| Sub-Category | Category | |
| Flooding | Disaster damage | Causal Conditions |
| Fire | ||
| Traffic accident | ||
| Economic loss | Individual state | Contextual Conditions |
| Physical impairment | ||
| Repetitive flooding | ||
| Dissatisfied with public support | Public state | |
| Receiving public support | ||
| Physical Trauma | Ruined life | Phenomenon |
| Psychological pain | ||
| Impairment of daily living | ||
| Receiving supports from family | Familial situation | Intervening Conditions |
| Considering familial condition | ||
| Maintaining occupation | Occupational state | |
| Lost one’s job | ||
| Urgency of recovery | Mental health literacy | |
| Understanding mental health | ||
| Journaling | Dealing traumatic memory | Action/Reaction Strategies |
| Concentrating on simple activities | ||
| Rely on religion | ||
| Positive thinking | Constructive thinking | |
| Mind control | ||
| Self-empowerment | ||
| Recognizing interpersonal relationship | Interpersonal support | |
| Receiving community support | ||
| Volunteering | ||
| Combining traditional remedies | Caring physical health | |
| Managing physical health | ||
| Having physical treatment | ||
| Prescribed psychotropic medication | Getting mental
health service | |
| Receiving psychological counseling | ||
| Seeking professional information | ||
| Ventilating by hobby | Recreational activity | |
| Exercise regularly | ||
| Chronic health problems | Getting Hwa-Byung
(Korean anger syndrome) | Results |
| Chronic physical symptoms | ||
| Being powerlessness | Losing meaning of life | |
| Despaired life | ||
| No meaning of life | ||
| Accepting reconstructed environment | Adapting restored life | |
| Adjusting self to changed situation | ||
| Re-experiencing disaster | Living in disaster | |
| Avoiding disaster situation | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.-J.; Choi, H.-B.; O’Donnell, M. Disaster Reintegration Model: A Qualitative Analysis on Developing Korean Disaster Mental Health Support Model. Int. J. Environ. Res. Public Health 2018, 15, 362. https://doi.org/10.3390/ijerph15020362
Choi Y-J, Choi H-B, O’Donnell M. Disaster Reintegration Model: A Qualitative Analysis on Developing Korean Disaster Mental Health Support Model. International Journal of Environmental Research and Public Health. 2018; 15(2):362. https://doi.org/10.3390/ijerph15020362
Chicago/Turabian StyleChoi, Yun-Jung, Hwa-Bok Choi, and Meaghan O’Donnell. 2018. "Disaster Reintegration Model: A Qualitative Analysis on Developing Korean Disaster Mental Health Support Model" International Journal of Environmental Research and Public Health 15, no. 2: 362. https://doi.org/10.3390/ijerph15020362
APA StyleChoi, Y. -J., Choi, H. -B., & O’Donnell, M. (2018). Disaster Reintegration Model: A Qualitative Analysis on Developing Korean Disaster Mental Health Support Model. International Journal of Environmental Research and Public Health, 15(2), 362. https://doi.org/10.3390/ijerph15020362