Dramatic Reduction in Diarrhoeal Diseases through Implementation of Cost-Effective Household Drinking Water Treatment Systems in Makwane Village, Limpopo Province, South Africa

 ,
, 
Abstract
:1. Introduction
2. Methodology
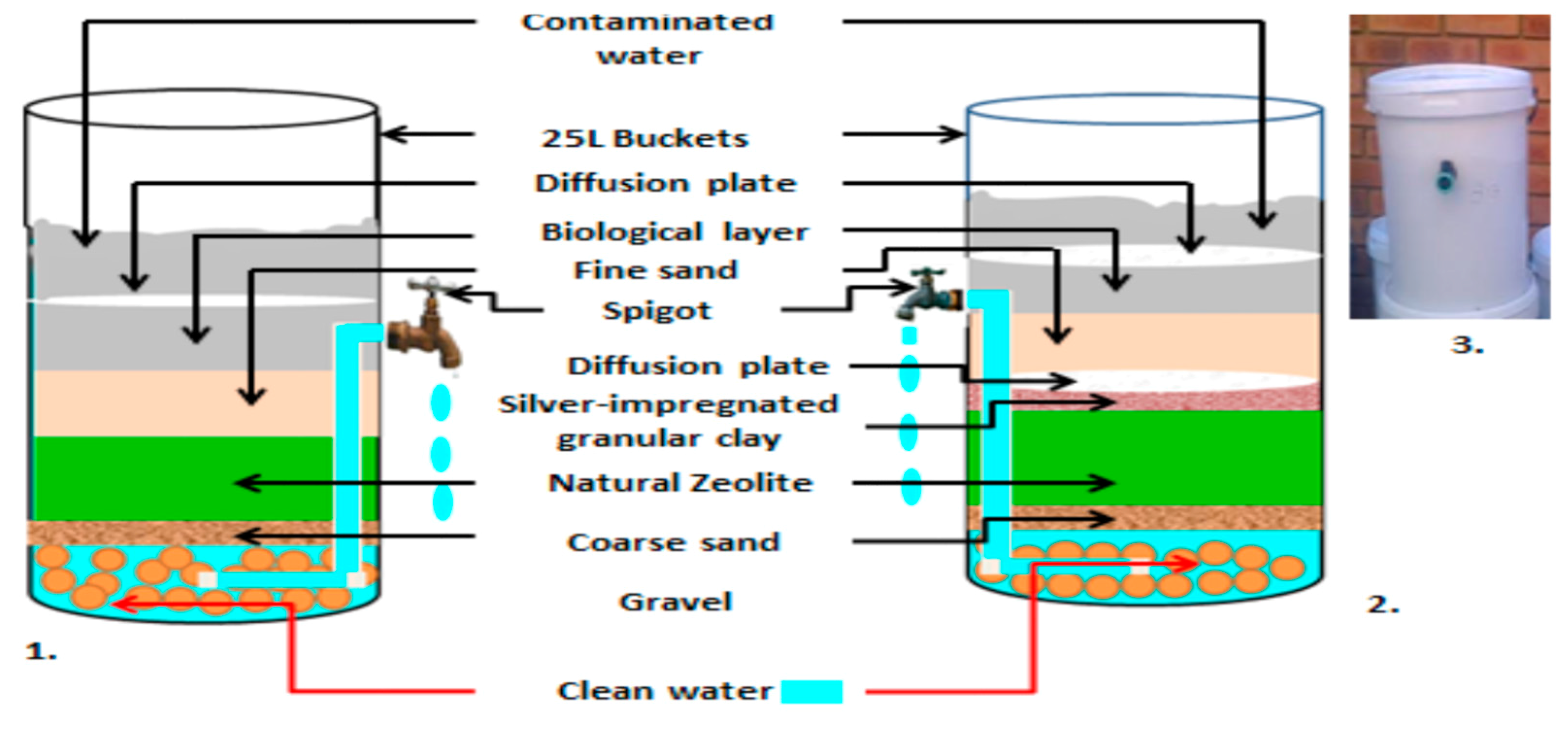
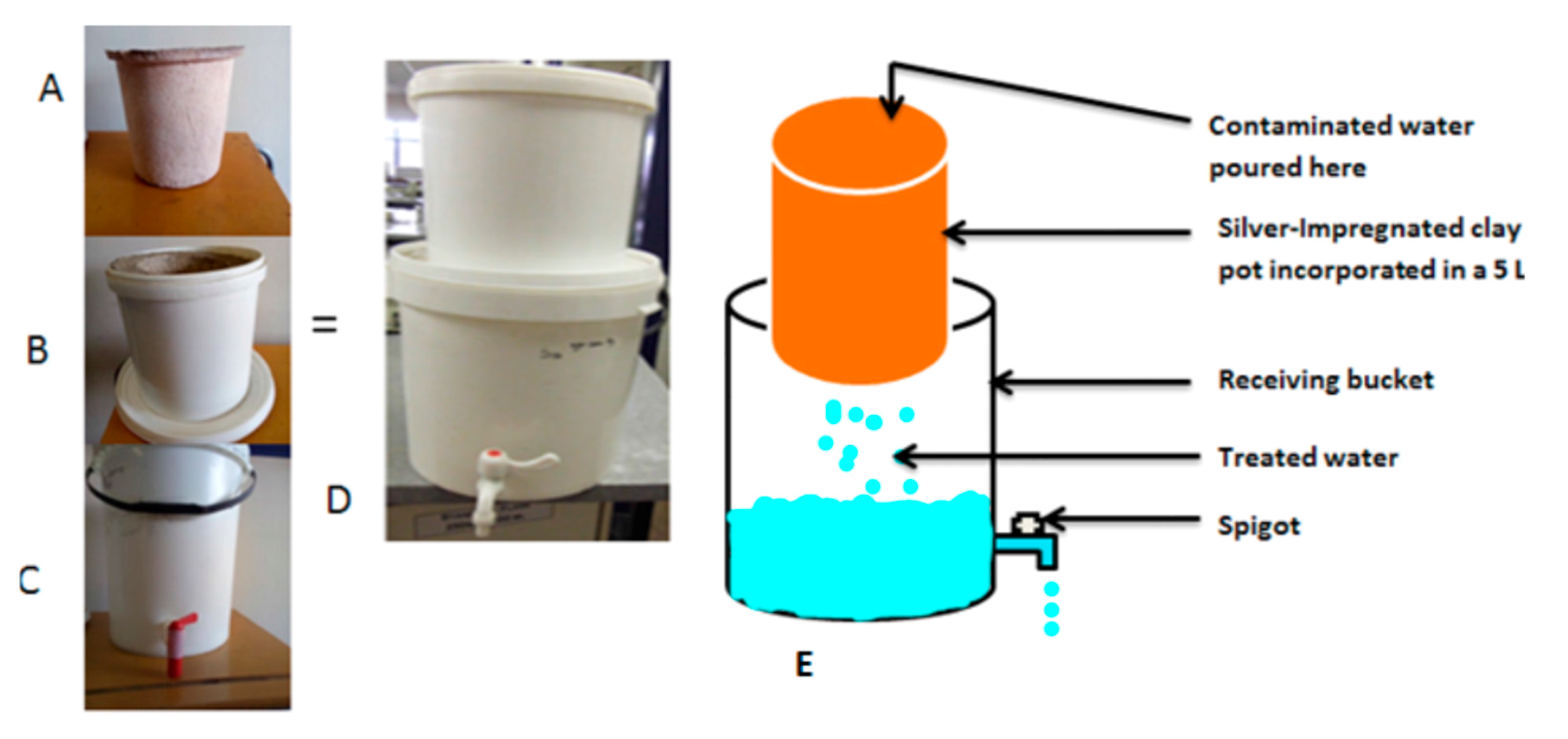
2.1. Modification of BSF-Z and SIPP Filters
2.2. Deployment of the Filters in Makwane Village
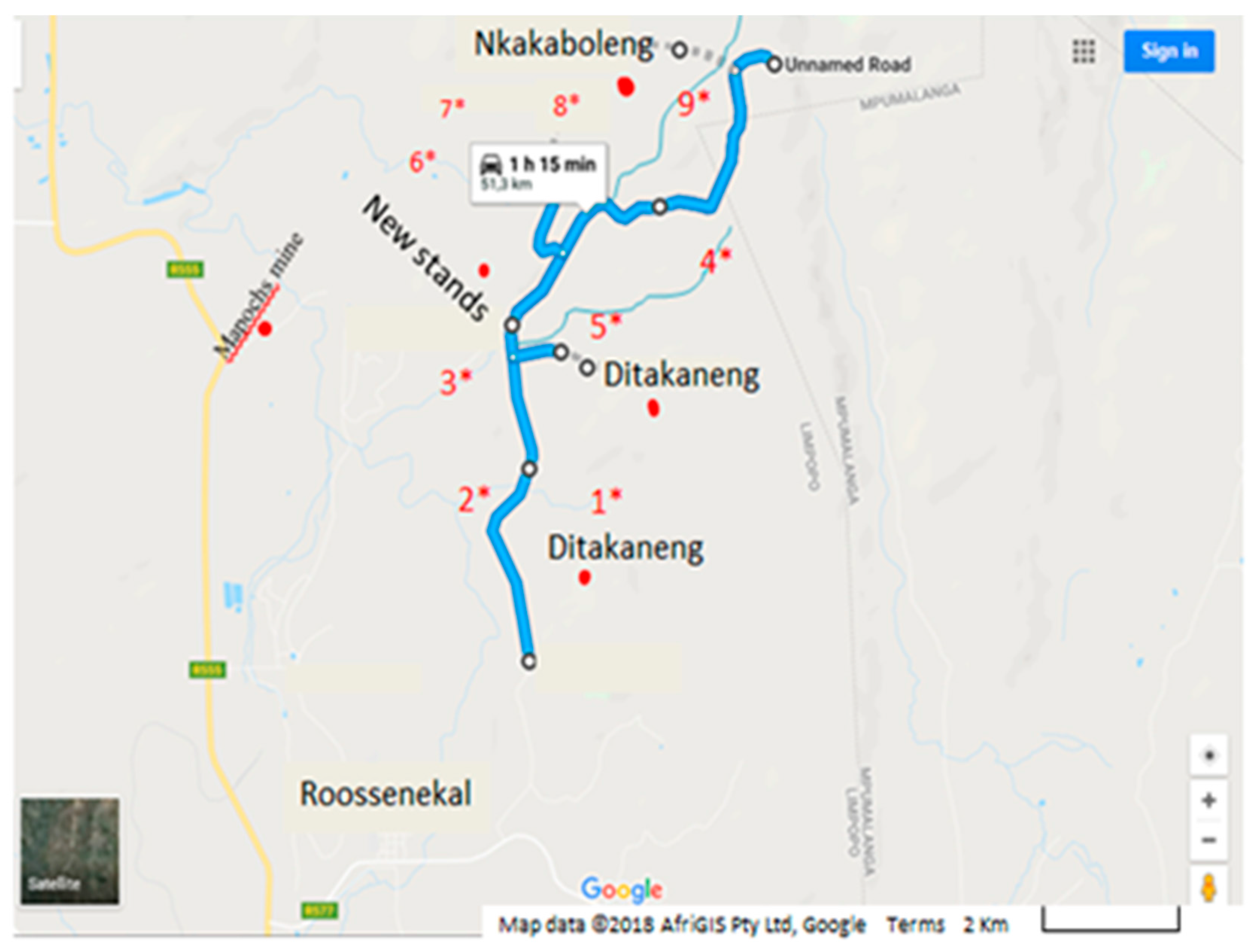
2.2.1. Description of the Study Area
2.2.2. Ethical Approval
2.2.3. Deployment of the Filters in Households of Makwane Village
2.3. Water Quality Assessment
2.3.1. Cuture-Based Methods for the Isolation of Presemptive Pathogenic E. coli
2.3.2. Molecular Identification of Pathogenic E. coli
2.4. Surveillance of Episodes of Diarrhoea before and after Implementation
2.5. Turbidity Removal Efficiency
2.6. Monitoring of Silver Leached from BSZ-SICG and SIPP Filters
2.7. Efficiency of the HWTS Devices in Removing Pathogenic E. coli Strains from Makwane Water Sources
2.8. Statistical Analysis of Data
3. Results
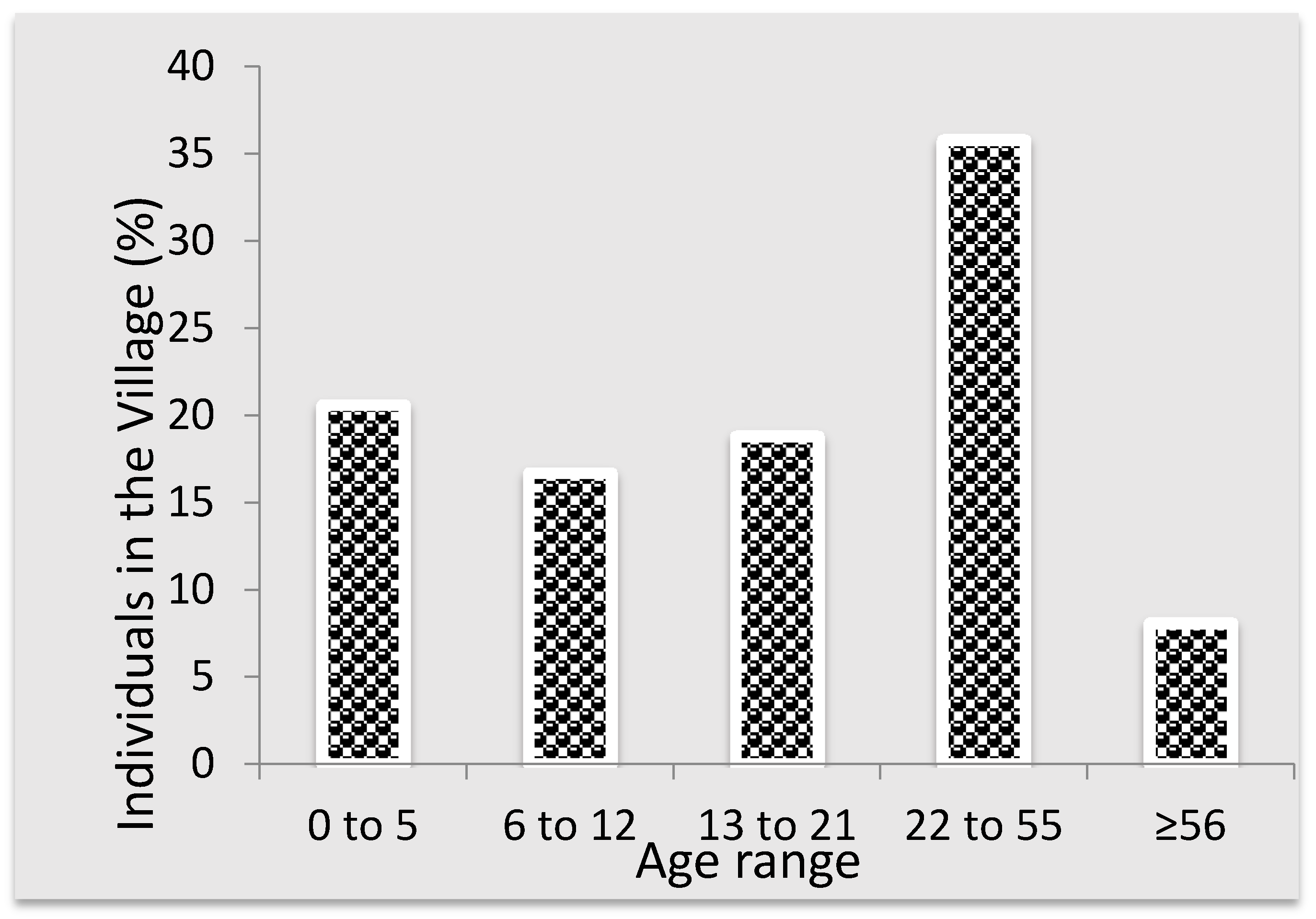
3.1. Demographic Information of the Study Area
3.2. Characteristics of Study Population Based on Episodes of Diarrhoea, and Water and Sanitation Facility Per Household
3.3. Water Quality Analysis
3.3.1. Average Mean E. coli Reduction, Turbidity Reduction, Temperature and pH of Untreated Water from Control Households and Treated Water from Intervention Households in Makwane Village
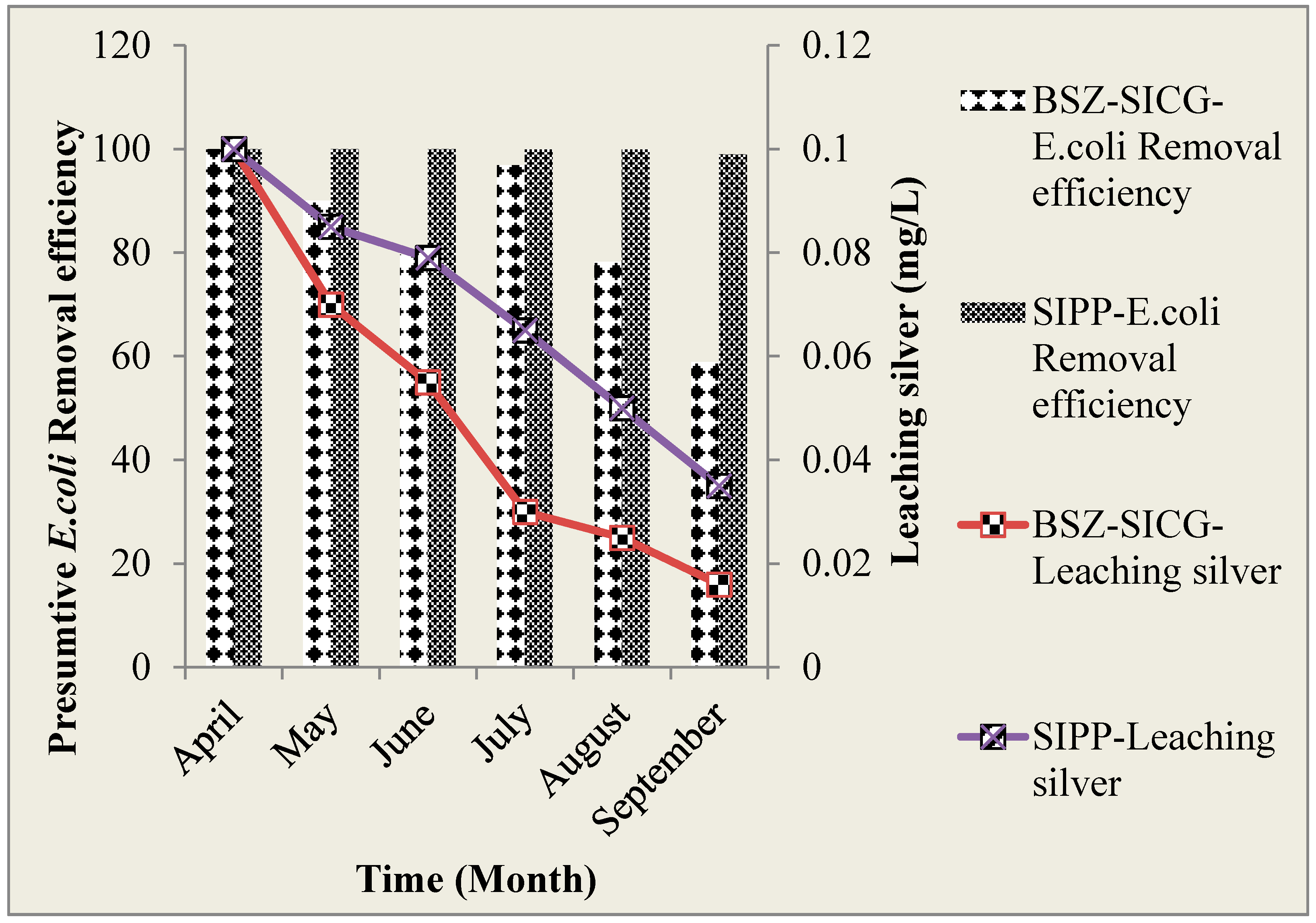
3.3.2. The Leaching of Silver Ions into Water Treated by SIPP and BSZ-SICG Filters over the Study Period (April 2015–September 2015) versus E. coli Removal Efficiency
3.3.3. Pearson’s Correlation between Presumtive E. coli Removal Efficiency and Silver Leached into Water Treated by BSZ-SIGC and SIPP Filters at POU
3.3.4. Amplification of Pathogenic E. coli Strains of by Multiplex PCR
3.4. Diarrhoeal Disease Incidence per Age Group and Stool Consistency Subsequent to HWTS Implementation in Makwane Village
4. Discussion
Water Quality
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- United Nations (UN) General Assembly. United Nations Millennium Declaration, Resolution Adopted by the General Assembly. A/RES/55/2. 18 September 2000. Available online: http://www.refworld.org/docid/3b00f4ea3.html (accessed on 21 February 2018).
- WHO/UNICEF Joint Monitoring Programme (JMP). Progress on Sanitation and Drinking Water—2014 Update; WHO Press: Geneva, Switzerland, 2014. [Google Scholar]
- Hardberger, A. Life, Liberty and the pursuit of water: Evaluating water as human right and the duties and obligations it creates. Northwest. Univ. J. Int. Hum. Rights 2005, 4, 331–362. [Google Scholar] [CrossRef]
- Fitzmaurice, M. The human rights to water. Fordham Environ. Law Rev. 2007, 18, 537–585. [Google Scholar]
- Prüss, A.; Kay, D.; Fewtrell, L.; Bartram, J. Estimating the burden of disease from water, sanitation, and hygiene at a global level. Environ. Health Perspect. 2002, 110, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Cousens, S.; Johnson, H.L.; Lawn, J.E.; Rudan, I.; Bassani, D.G.; Jha, P.; Campbell, H.; Walker, C.F.; Cibulskis, R.; et al. Child Health Epidemiology Reference Group of WHO and UNICEF. Lancet 2010, 375, 1969–1987. [Google Scholar] [CrossRef]
- Santosham, M.; Chandran, A.; Fitzwater, S.; Fischer-Walker, C.; Baqui, A.H.; Black, R. Progress and barriers for the control of diarrhoeal disease. Lancet 2010, 376, 63–67. [Google Scholar] [CrossRef]
- Liu, L.; Johnson, H.L.; Cousens, S.; Perin, J.; Scott, S.; Lawn, J.E.; Rudan, I.; Campbell, H.; Cibulskis, R.; Li, M.; et al. Global, regional, and national causes of child mortality: An updated systematic analysis for 2010 with time trends since 2000. Lancet 2012, 379, 2151–2161. [Google Scholar] [CrossRef]
- Statistics South Africa (Stats SA). Millennium Development Goals, Country Report 2013; Stats SA: Pretoria, South Africa, 2013.
- Statistics South Africa (Stats SA). Census 2011: Statistical Release; Statistics South Africa: Pretoria, South Africa, 2012; pp. 52–53.
- Chola, L.; Michalow, J.; Tugendhaft, A.; Hofman, K. Reducing diarrhoea deaths in South Africa: Costs and effects of scaling up essential interventions to prevent and treat diarrhoea in under five children. BMC Public Health 2015, 15, 394. [Google Scholar] [CrossRef] [PubMed]
- Mwabi, J.K.; Adeyemo, F.E.; Mahlangu, T.O.; Mamba, B.B.; Brouckaert, B.M.; Swartz, C.D.; Offringa, G.; Mpenyana-Monyatsi, L.; Momba, M.N.B. Household water treatment systems: A solution to the production of safe drinking water by the low-income communities of Southern Africa. J. Phys. Chem. Earth. 2011, 36, 1120–1128. [Google Scholar] [CrossRef]
- Mahlangu, T.O.; Mamba, B.B.; Momba, M.N.B. A comparative assessment of chemical contaminant removal by three household water treatment filters. Water SA. 2012, 38, 39–47. [Google Scholar] [CrossRef]
- Mwabi, J.K.; Mamba, B.B.; Momba, M.N.B. Removal of waterborne bacteria from surface water and groundwater by cost-effective household water treatment systems (HWTS): A sustainable solution for improving water quality in rural communities of Africa. Water S. Afr. 2012, 39, 445–447. [Google Scholar] [CrossRef]
- South African Bureau of Standards (SABS). SANS 241-1: 2011, South African National Standard (SANS), Drinking Water. Part 1: Microbiological, Physical, Aesthetic and Chemical Determinands; South African Bureau of Standards (SABS): Pretoria, South Africa, 2011. [Google Scholar]
- World Health Organization. The World Health Report 2006—Working Together for Health; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Map of Makwane Village Showing All the Sections and the Surrounding Streams/Rivers Where Some of the Samples Were Collected in Addition to Water Collected from Households. Available online: https://www.google.com/maps/dir/-25.1631288,29.9473028/-25.0873681,29.9861423/@-25.142823,29.9184398,12.2z/data=!4m2!4m1!3e0?hl=en (accessed on 27 February 2018).
- Nguyen, T.V.; Le Van, P.; Le Huy, C.; Gia, K.N.; Weintraub, A. Detection and characterization of diarrheagenic Escherichia coli from young children in Hanoi, Vietnam. J. Clin. Microbio. 2005, 43, 755–760. [Google Scholar] [CrossRef] [PubMed]
- Broezel, V.S.; Cloete, T.E. Effect of storage time and temperature on the aerobic plate count and on the community structure of two water samples. Water S. Afr. 1991, 17, 289–300. [Google Scholar]
- Heleba, S. Access to sufficient water in South Africa: How far have we come? Law Democr. Dev. 2012, 15, 1–35. [Google Scholar] [CrossRef]
- South African Bureau of Standards (SABS). SANS 241-1: 2015, South African National Standard (SANS), Drinking Water. Part 1: Microbiological, Physical, Aesthetic and Chemical Determinands; South African Bureau of Standards (SABS): Pretoria, South Africa, 2015. [Google Scholar]
- Environmental Protection Agency. Water Quality in Small Community Distribution Systems; EPA: Sacramento, CA, USA, 2012.
- WHO (World Health Organization). Guidelines for Drinking-Water Quality, 4th ed.; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Carnot, N.L.S. Reflections on the Motive Power of Heat, Accompanied by Kelvin W. T. “An Account of Carnot’s Theory”, 2nd ed.; Thurston, R.H., Ed.; John Willey & Sons: New York, NY, USA, 1897. [Google Scholar]
- Department of Water Affairs and Forestry. South African Water Quality Guidelines, Volume 1: Domestic Use, 2nd ed.; Department of Water Affairs and Forestry: Pretoria, South Africa, 1996; p. 1. [Google Scholar]
- Franz, A. A Performance Study of Ceramic Candle Filters in Kenya, Including Tests for Coliphage Removal. Master’s Thesis, Department of Civil and Environmental Engineering, Massachusetts Institute of Technology, Cambridge, MA, USA, 2004. [Google Scholar]
- Low, J. Appropriate Microbiological Indicator Tests for Drinking Water in Developing Countries and Assessment of Ceramic Water Filters. Master’s Thesis, Department of Civil and Environmental Engineering, Massachusetts Institute of Technology, Cambridge, MA, USA, 2002. [Google Scholar]
- Ngai, T.K.K.; Shrestha, R.R.; Dangol, B.; Maharjan, M.; Murcott, S.E. Design for sustainable development—Household drinking water filter for arsenic and pathogen treatment in Nepal. J. Environ. Sci. Health Part A 2007, 42, 1879–1888. [Google Scholar] [CrossRef] [PubMed]
- Devi, R.; Alemayehu, E.; Singh, V.; Kumar, A.; Mengistie, E. Removal of fluoride, arsenic and coliform bacteria by modified homemade filter media from drinking water. Bioresour. Technol. 2008, 99, 2269–2274. [Google Scholar] [CrossRef] [PubMed]
- Murphy, H.M.; McBean, E.A.; Farahbakhsh, K. Nitrification, denitrification and ammonification in point-of-use biosand filters in rural Cambodia. J. Water Health 2010, 8, 804–817. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.A.; Stauber, C.E.; Koksal, F.; DiGiano, F.A.; Sobsey, M. Reductions of E. coli, echovirus type 12 and bacteriophages in an intermittently operated household-scale slow sand filter. Water Res. 2008, 42, 2662–2670. [Google Scholar] [CrossRef] [PubMed]
- Nangmenyi, G.; Xao, W.; Mehrabi, S.; Mintz, E.; Economy, J. Bactericidal activity of Ag nanoparticle-impregnated fibreglass for water disinfection. J. Water Health, 2009, 7, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Michen, B.; Meder, F.; Rust, A.; Fritsch, J.; Aneziris, C.; Graule, T. Virus removal in ceramic depth filters based on diatomaceous earth. Environ. Sci. Technol. 2012, 46, 1170–1177. [Google Scholar] [CrossRef] [PubMed]
- Van Halem, D. Ceramic Silver-Impregnated Pot Filters for Household Drinking Water Treatment in Developing Countries. Master’s Thesis, Delft University of Technology, Delft, The Netherlands, 2006. [Google Scholar]
- Tiwari, S.; Schmidt, W.P.; Darby, J.; Kariuki, Z.G.; Jenkins, M.W. Intermittent slow sand filtration for preventing diarrhoea among children in households using unimproved water sources: A randomized controlled trial. Trop. Med. Int. Health 2009, 14, 1374–1382. [Google Scholar] [CrossRef] [PubMed]
- Du Preez, M.; Conroy, R.M.; Wright, J.A.; Moyo, S.; Potgieter, N.; Gundry, S.W. Use of ceramic water filtration in the prevention of diarrheal disease: A randomized controlled trial in rural South Africa and Zimbabwe. Am. J. Trop. Med. Hyg. 2008, 79, 696–701. [Google Scholar] [PubMed]
- Duke, W.F.; Nordin, R.N.; Baker, D.; Mazumder, A. The use and performance of BioSand filters in the Artibonite Valley of Haiti: A field study of 107 households. Rural Remote Health 2006, 6, 570. [Google Scholar] [PubMed]
- Clasen, T.F.; Brown, J.; Collin, S.M. Preventing diarrhoea with household ceramic water filters: Assessment of a pilot project in Bolivia. Int. J. Environ. Health Res. 2006, 16, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Michen, B.; Diatta, A.; Fritsch, J.; Aneziris, C.G.; Graule, T. Removal of colloidal particles in ceramic depth filters based on diatomaceous earth. Sep. Purif. Technol. 2011, 81, 77–87. [Google Scholar]
- Momba, M.N.B.; Offringa, G.; Nameni, G.; Brouckaert, B. Development of a Prototype Nanotechnology-Based Clay Filter Pot to Purify Water for Drinking and Cooking in Rural Homes; WRC Report No. KV 244/10; Water Research Commission: Pretoria, South Africa, 2010; pp. 27–32. [Google Scholar]
- Stauber, C.E.; Ortiz, G.M.; Loomis, D.P.; Sobsey, M.D. A randomized controlled trial of the concrete biosand filter and its impact on diarrheal disease in Bonao, Dominican Republic. Am. J. Trop. Med. Hyg. 2009, 80, 286–293. [Google Scholar] [PubMed]
- Liang, K.; Sobsey, M.; Stauber, C. Field Note: Improving Household Water Quality—Use of Biosand Filters in Cambodia; Water and Sanitation Program: Hagar, Cambodia, 2010. [Google Scholar]
- Stauber, C.E.; Printy, E.R.; McCarty, F.A.; Liang, K.R.; Sobsey, M.D. Cluster randomized trial of the plastic biosand water filter in Cambodia. Environ. Sci. Technol. 2012, 46, 722–728. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primer Name | Sequences 5’→3’ | Target Genes | Size | Reference |
|---|---|---|---|---|
| EHEC-423 | F-TGGAAAAACTCAGTGCCTCT- R-CCAGTCCGTAAATTCATTCT- | stx1 | 423 bp | [18] |
| EPEC-300 | R-GGAATCAGACGCAGACTGGTAGT- F-GGAAGTCAAATTCATGGGGGTAT- | bfpA | 300 bp | [18] |
| ETEC-187 | F-GCTAAACCAGTAGAGGTCTTCAAAA- R-CCCGGTACAGAGCAGGATTACAACA- | estA (ST) | 187 bp | [18] |
| EIEC-508 | R-CACACGGAGCTCCTCAGTC- F-CCCCCAGCCTAGCTTAGTTT- | ipaH | 508 bp | [18] |
| EAEC-215 | R-ACGACACCCCTGATAAACAA- F-ATTGTCCTCAGGCATTTCAC- | aaiC | 215 bp | [18] |
| Characteristics | Frequency (n = 88) | Percentage (%) | p-Value | |
|---|---|---|---|---|
| Episodes of diarrhoea | No | 22 | 25 | p = 0.000176115 |
| Yes | 66 | 75 | ||
| Diarrhoeal episodes based on water source | Roof water harvesting | 06 | 6.8 | |
| River/stream water | 62 | 70.5 | ||
| Open spring | 12 | 13.6 | ||
| Borehole | 8 | 9.1 | ||
| Municipal treated tap water | NA | NA | ||
| Access to proper sanitation * | With access | 52 | 59.1 | p = 0.369174254 |
| No access | 36 | 40.9 | ||
| Water Quality Parameters | Control Households | Intervention Households | ||
|---|---|---|---|---|
| Untreated Water | BSZ-SICG | SIPP | p-Value | |
| E. coli | 4.3830 Log10 * CFU/100 mL | 0.4770 Log10 CFU/100 mL | ** NG | 0.000004201 |
| % E. coli reduction | - | 89.1% | 100% | |
| Turbidity (*** NTU) | 168 | 2.34 | 0.85 | 0.000025949 |
| % Turbidity reduction | - | 98.6% | 99.5% | |
| Temperature (°C) | 25.0 | 19.8 | 22.5 | |
| pH | 8.2 | 7.8 | 7.5 | |
| Characteristics | Control Households (n = 108) | Intervention Households (n = 372) | p-Value | |||
|---|---|---|---|---|---|---|
| Age Groups | Episodes of Diarrhoea | Frequency | Percent (%) | Frequency | Percent (%) | |
| 0–5 | Yes | 17 | 85 | 4 | 5.1 | 0.0000105 |
| No | 3 | 15 | 75 | 94.9 | ||
| 6–12 | Yes | 9 | 60 | 3 | 4.6 | 0.0000959 |
| No | 6 | 40 | 62 | 95.4 | ||
| 13–21 | Yes | 7 | 36.8 | 1 | 1.4 | 0.0001004 |
| No | 12 | 63.2 | 70 | 98.6 | ||
| 22–55 | Yes | 20 | 47.6 | 3 | 2.3 | 0.0000096 |
| No | 22 | 52.4 | 127 | 97.7 | ||
| ≥56 | Yes | 9 | 75 | 3 | 11.1 | 0.0005018 |
| No | 3 | 25 | 24 | 88.9 | ||
| Stool consistency | Watery | 43/62 | 69.3 | 14/14 | 100.0 | |
| Bloody | 6/62 | 9.7 | 0/14 | 0 | ||
| Mucus | 13/62 | 21 | 0/14 | 0 | ||
| Overall episodes of diarrhoea in control households | Overall episodes of diarrhoea in intervention households | |||||
| 62/108 (57.4%) | 14/372 (3.8%) | |||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moropeng, R.C.; Budeli, P.; Mpenyana-Monyatsi, L.; Momba, M.N.B. Dramatic Reduction in Diarrhoeal Diseases through Implementation of Cost-Effective Household Drinking Water Treatment Systems in Makwane Village, Limpopo Province, South Africa. Int. J. Environ. Res. Public Health 2018, 15, 410. https://doi.org/10.3390/ijerph15030410
Moropeng RC, Budeli P, Mpenyana-Monyatsi L, Momba MNB. Dramatic Reduction in Diarrhoeal Diseases through Implementation of Cost-Effective Household Drinking Water Treatment Systems in Makwane Village, Limpopo Province, South Africa. International Journal of Environmental Research and Public Health. 2018; 15(3):410. https://doi.org/10.3390/ijerph15030410
Chicago/Turabian StyleMoropeng, Resoketswe Charlotte, Phumudzo Budeli, Lizzy Mpenyana-Monyatsi, and Maggy Ndombo Benteke Momba. 2018. "Dramatic Reduction in Diarrhoeal Diseases through Implementation of Cost-Effective Household Drinking Water Treatment Systems in Makwane Village, Limpopo Province, South Africa" International Journal of Environmental Research and Public Health 15, no. 3: 410. https://doi.org/10.3390/ijerph15030410
APA StyleMoropeng, R. C., Budeli, P., Mpenyana-Monyatsi, L., & Momba, M. N. B. (2018). Dramatic Reduction in Diarrhoeal Diseases through Implementation of Cost-Effective Household Drinking Water Treatment Systems in Makwane Village, Limpopo Province, South Africa. International Journal of Environmental Research and Public Health, 15(3), 410. https://doi.org/10.3390/ijerph15030410