Internalized Transphobia, Resilience, and Mental Health: Applying the Psychological Mediation Framework to Italian Transgender Individuals

 ,
,  ,
, 
Abstract
:1. Introduction
1.1. Minority Stress, Health, and Resilience in the TGNC Population
1.2. The Psychological Mediation Framework within the TGNC Population
1.3. Stigma and Health in the Italian TGNC Population
1.4. The Current Study
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Measures
2.3.1. Socio-Demographic Characteristics
2.3.2. Anti-Transgender Discrimination
2.3.3. Internalized Transphobia
2.3.4. Depression
2.3.5. Anxiety
2.3.6. Resilience
2.4. Preliminary and Statistical Analyses
3. Results
3.1. Descriptive Statistics and Bivariate Correlations
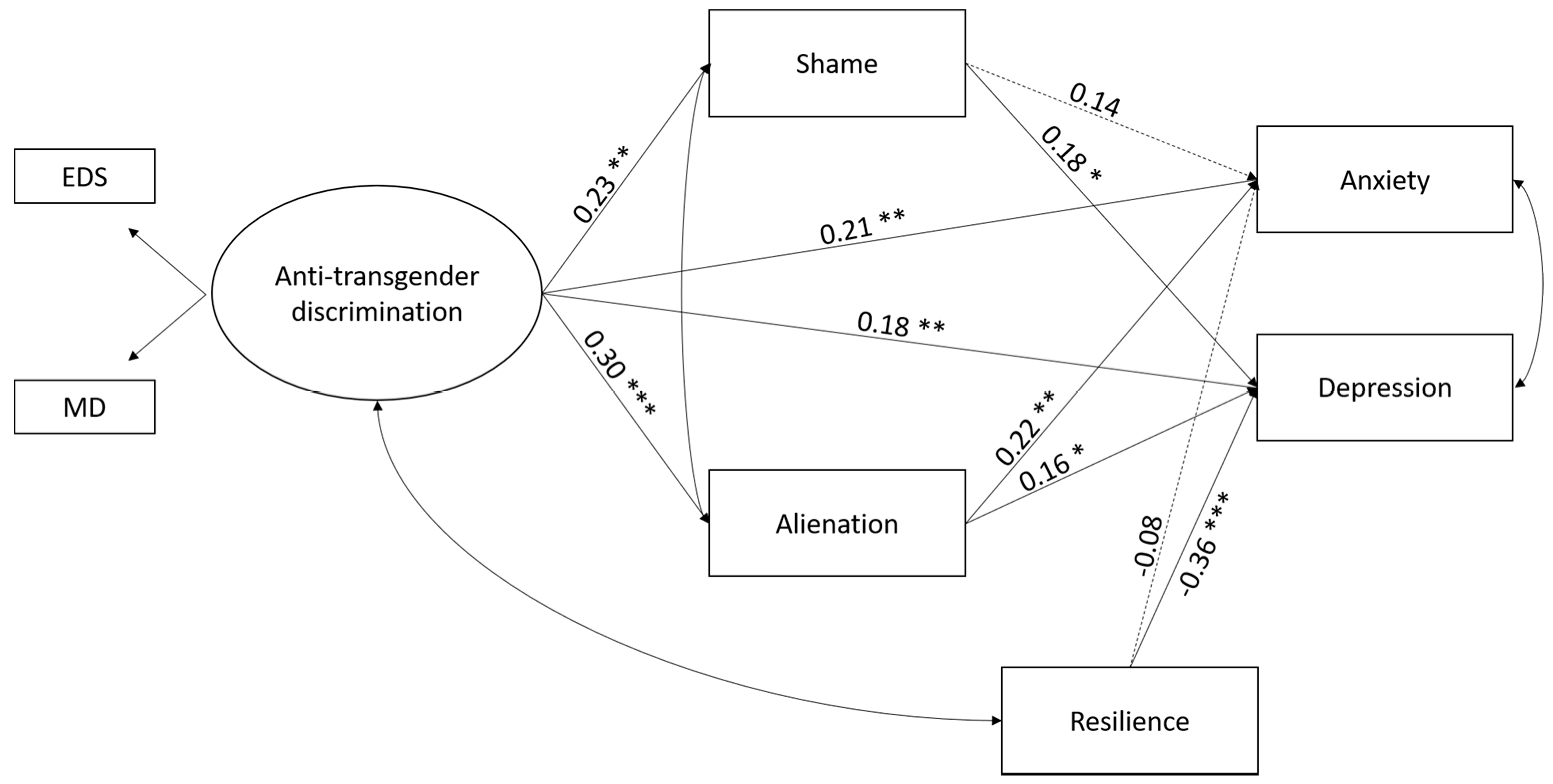
3.2. Associations between Minority Stressors, Resilience, and Mental Health
Control Variables
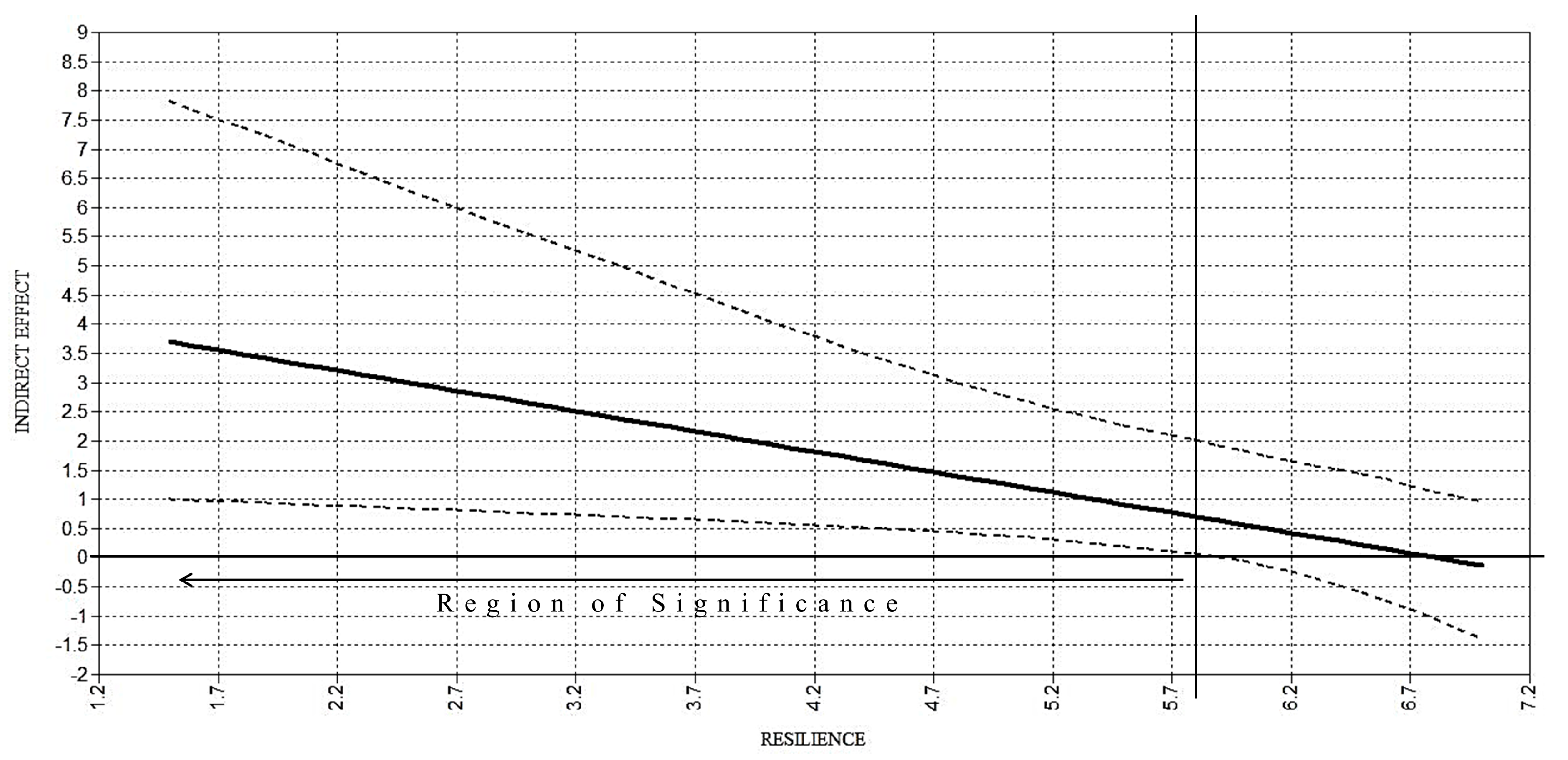
3.3. Internalized Transphobia as a Mediator and the Moderating Role of Resilience
4. Discussion
4.1. Limitations and Suggestions for Future Research
4.2. Implications for Clinical Practice
5. Conclusions
Author Contributions
Conflicts of Interest
References
- American Psychological Association. Guidelines for psychological practice with transgender and gender nonconforming people. Am. Psychol. 2015, 70, 832–864. [Google Scholar] [CrossRef]
- Bradford, J.; Reisner, S.L.; Honnold, J.A.; Xavier, J. Experiences of transgender-related discrimination and implications for health: Results from the Virginia Transgender Health Initiative Study. Am. J. Public Health 2013, 103, 1820–1829. [Google Scholar] [CrossRef] [PubMed]
- Bockting, W.O.; Miner, M.H.; Swinburne Romine, R.E.; Hamilton, A.; Coleman, E. Stigma, mental health, and resilience in an online sample of the US transgender population. Am. J. Public Health 2013, 103, 943–951. [Google Scholar] [CrossRef] [PubMed]
- Shipherd, J.C.; Maguen, S.; Skidmore, W.C.; Abramovitz, S.M. Potentially traumatic events in a transgender sample: Frequency and associated symptoms. Traumatology 2011, 17, 56–67. [Google Scholar] [CrossRef]
- Breslow, A.S.; Brewster, M.E.; Velez, B.L.; Wong, S.; Geiger, L.; Soderstrom, B. Resilience and collective action: Exploring buffers against minority stress for transgender individuals. Psychol. Sex. Orientat. Gend. Divers. 2015, 2, 253–265. [Google Scholar] [CrossRef]
- Meyer, I.H. Prejudice as stress: Conceptual and measurement problems. Am. J. Public Health 2003, 93, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Meyer, I.H. Prejudice and discrimination as social stressors. In The Health of Sexual Minorities: Public Health Perspectives on Lesbian, Gay, Bisexual and Transgender Populations; Meyer, I.H., Northridge, M.E., Eds.; Springer: New York, NY, USA, 2007; pp. 242–267. ISBN 978-0-387-31334-4. [Google Scholar]
- Scandurra, C.; Amodeo, A.L.; Valerio, P.; Bochicchio, V.; Frost, D.M. Minority stress, resilience, and mental health: A study of Italian transgender people. J. Soc. Issues 2017, 73, 563–585. [Google Scholar] [CrossRef]
- Testa, R.J.; Habarth, J.; Peta, J.; Balsam, J.; Bockting, W.O. Development of the Gender Minority Stress and Resilience Measure. Psychol. Sex. Orientat. Gend. Divers. 2015, 2, 65–77. [Google Scholar] [CrossRef]
- Hatzenbuehler, M.L. How does sexual minority stigma “get under the skin”? A psychological mediation framework. Psychol. Bull. 2009, 135, 707–730. [Google Scholar] [CrossRef] [PubMed]
- Budge, S.L.; Adelson, J.L.; Howard, K.A.S. Anxiety and depression in transgender individuals: The roles of transition status, loss, social support, and coping. J. Consult. Clin. Psychol. 2013, 81, 545–557. [Google Scholar] [CrossRef] [PubMed]
- Reisner, S.L.; Gamarel, K.E.; Nemoto, T.; Operario, D. Dyadic effects of gender minority stressors in substance use behaviors among transgender women and their non-transgender male partners. Psychol. Sex. Orientat. Gend. Divers. 2014, 1, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Austin, A.; Goodman, R. The impact of social connectedness and internalized transphobic stigma on self-esteem among transgender and gender non-conforming adults. J. Homosex. 2017, 64, 825–841. [Google Scholar] [CrossRef] [PubMed]
- Rood, B.A.; Reisner, S.L.; Puckett, J.A.; Surace, F.I.; Berman, A.K.; Pantalone, D.V. Internalized transphobia: Exploring perceptions of social messages in transgender and gender-nonconforming adults. Int. J. Transgend. 2017, 18, 411–426. [Google Scholar] [CrossRef]
- Bockting, W.O. Internalized transphobia. In The International Encyclopedia of Human Sexuality; Whelehan, P., Bolin, A., Eds.; Wiley-Blackwell: Malden, MA, USA, 2015; pp. 583–625. [Google Scholar] [CrossRef]
- Lev, A.I. Transgender Emergence: Therapeutic Guidelines for Working with Gender-Variant People and Their Families; Haworth Clinical Practice Press: Binghamton, NY, USA, 2004; ISBN 078902117X. [Google Scholar]
- Scandurra, C.; Amodeo, A.L.; Bochicchio, V.; Valerio, P.; Frost, D.M. Psychometric characteristics of the Transgender Identity Survey in an Italian sample: A measure to assess positive and negative feelings towards transgender identity. Int. J. Transgend. 2017, 18, 53–65. [Google Scholar] [CrossRef]
- Diamond, L.M.; Pardo, S.T.; Butterworth, M.R. Transgender experience and identity. In Handbook of Identity Theory and Research; Schwartz, S.J., Luyckx, K., Vignoles, V.L., Eds.; Springer: New York, NY, USA, 2011; pp. 629–647. ISBN 978-1-4419-7987-2. [Google Scholar]
- Perez-Brumer, A.; Hatzenbuehler, M.L.; Oldenburg, C.L.; Bockting, W.O. Individual- and structural-level risk factors for suicide attempts among transgender adults. Behav. Med. 2015, 41, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Pflum, S.R.; Testa, R.J.; Balsam, K.F.; Goldblum, P.B.; Bongar, B. Social support, trans community connectedness, and mental health symptoms among transgender and gender nonconforming adults. Psychol. Sex. Orientat. Gend. Divers. 2015, 2, 281–286. [Google Scholar] [CrossRef]
- Singh, A.A.; Hays, D.G.; Watson, L.S. Strength in the face of adversity: Resilience strategies of transgender individuals. J. Couns. Dev. 2011, 89, 20–27. [Google Scholar] [CrossRef]
- Singh, A.A.; Meng, S.E.; Hansen, A.W. “I am my own gender”: Resilience strategies of trans youth. J. Couns. Dev. 2014, 92, 208–218. [Google Scholar] [CrossRef]
- Testa, R.J.; Jimenez, C.L.; Rankin, S. Risk and resilience during transgender identity development: The effects of awareness and engagement with other transgender people on affect. J. Gay Lesbian Ment. Health 2014, 18, 31–46. [Google Scholar] [CrossRef]
- Meyer, I.H. Resilience in the study of minority stress and health of sexual and gender minorities. Psychol. Sex. Orientat. Gend. Divers. 2015, 2, 209–213. [Google Scholar] [CrossRef]
- Zimmerman, M.A. Resiliency theory: A strengths-based approach to research and practice for adolescent health. Health Educ. Behav. 2013, 40, 381–383. [Google Scholar] [CrossRef] [PubMed]
- Harvey, M.R. Towards an ecological understanding of resilience in trauma survivors: Implications for theory, research, and practice. J. Aggress. Maltreat. Trauma 2007, 14, 9–32. [Google Scholar] [CrossRef]
- Rainone, N.; Chiodi, A.; Lanzillo, R.; Magri, V.; Napolitano, N.; Brescia Morra, V.; Valerio, P.; Freda, M.F. Affective disorders and Health-Related Quality of Life (HRQoL) in adolescents and young adults with Multiple Sclerosis (MS): The moderating role of resilience. Qual. Life Res. 2017, 26, 727–736. [Google Scholar] [CrossRef] [PubMed]
- Luthar, S.S.; Cicchetti, D.; Becker, B. The construct of resilience: A critical evaluation and guidelines for future work. Child Dev. 2000, 71, 543–562. [Google Scholar] [CrossRef] [PubMed]
- Liao, K.Y.H.; Kashubeck-West, S.; Weng, C.Y.; Deitz, C. Testing a mediation framework for the link between perceived discrimination and psychological distress among sexual minority individuals. J. Couns. Psychol. 2015, 62, 226–241. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.R.; Stratton, N.; Hart, T.A. Minority stress and mental and sexual health: Examining the psychological mediation framework among gay and bisexual men. Psychol. Sex. Orientat. Gend. Divers. 2016, 3, 313–324. [Google Scholar] [CrossRef]
- Testa, R.J.; Michaels, M.S.; Bliss, W.; Rogers, M.L.; Balsam, K.F.; Joiner, T. Suicidal ideation in transgender people: Gender minority stress and interpersonal theory factors. J. Abnorm. Psychol. 2017, 126, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Timmins, L.; Rimes, K.A.; Rahman, Q. Minority stressors and psychological distress in transgender individuals. Psychol. Sex. Orientat. Gend. Divers. 2017, 4, 328–340. [Google Scholar] [CrossRef]
- Tucker, R.P.; Testa, R.T.; Reger, M.A.; Simpson, T.L.; Shipherd, J.C.; Lehavot, K. Current and military-specific gender minority stress factors and their relationship with suicide ideation in transgender veterans. Suicide Life Threat. Behav. 2018. [Google Scholar] [CrossRef] [PubMed]
- Luhtanen, R.; Crocker, J. A collective self-esteem scale: Self-evaluation of one’s social identity. Personal. Soc. Psychol. Bull. 1992, 18, 302–318. [Google Scholar] [CrossRef]
- Amodeo, A.L.; Vitelli, R.; Scandurra, C.; Picariello, S.; Valerio, P. Adult attachment and transgender identity in the Italian context: Clinical implications and suggestions for further research. Int. J. Transgend. 2015, 16, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Scandurra, C.; Mezza, F.; Bochicchio, V.; Valerio, P.; Amodeo, A.L. LGBT elders health from the minority stress perspective. Literature review & research recommendations. Psicol. Della Salut. 2017, 2, 70–96. [Google Scholar] [CrossRef]
- Scandurra, C.; Picariello, S.; Valerio, P.; Amodeo, A.L. Sexism, homophobia and transphobia in a sample of Italian pre-service teachers: The role of socio-demographic features. J. Educ. Teach. 2017, 43, 245–261. [Google Scholar] [CrossRef]
- Scandurra, C.; Braucci, O.; Bochicchio, V.; Valerio, P.; Amodeo, A.L. “Soccer is a matter of real men?” Sexist and homophobic attitudes in three Italian soccer teams differentiated by sexual orientation and gender identity. Int. J. Sport Exerc. Psychol. 2017, 1–17. [Google Scholar] [CrossRef]
- Scandurra, C.; Bacchini, D.; Esposito, C.; Bochicchio, V.; Valerio, P.; Amodeo, A.L. The influence of minority stress, gender, and legalization of civil unions on parenting desire and intention in lesbian women and gay men: Implications for social policy and clinical practice. J. GLBT Fam. Stud. 2018, 1–25. [Google Scholar] [CrossRef]
- Amodeo, A.L.; Picariello, S.; Valerio, P.; Scandurra, C. Empowering transgender youths: Promoting resilience through a group training program. J. Gay Lesbian Ment. Health 2018, 1, 3–19. [Google Scholar] [CrossRef]
- Hendricks, M.L.; Testa, R.J. A conceptual framework for clinical work with transgender and gender nonconforming clients: An adaptation of the minority stress model. Prof. Psychol. Res. Pract. 2012, 43, 460–467. [Google Scholar] [CrossRef]
- Bariola, E.; Lyons, A.; Leonard, W.; Pitts, M.; Badcock, P.; Couch, M. Demographic and psychosocial factors associated with psychological distress and resilience among transgender individuals. Am. J. Public Health 2015, 105, 2108–2116. [Google Scholar] [CrossRef] [PubMed]
- Snow, J. Qualtrics Survey Software: Handbook for Research Professionals; Qualtrics Labs, Incorporated: Provo, UT, USA, 2012. [Google Scholar]
- Williams, D.R.; Yu, Y.; Jackson, J.S.; Anderson, N.B. Racial differences in physical and mental health: Socio-economic status, stress and discrimination. J. Health Psychol. 1997, 2, 335–351. [Google Scholar] [CrossRef] [PubMed]
- Meyer, I.M.; Schwartz, S.; Frost, D.M. Social patterning of stress and coping: Does disadvantaged social statuses confer excess exposure and fewer coping resources? Soc. Sci. Med. 2008, 67, 368–379. [Google Scholar] [CrossRef] [PubMed]
- Bockting, W.O.; Miner, M.H.; Swinburne Romine, R.E.; Robinson, B.B.E.; Rosser, B.R.S.; Coleman, E. The Transgender Identity Survey; University of Minnesota, Program in Human Sexuality: Minneapolis, MN, USA, 2010. [Google Scholar]
- Fava, G.A. Versione Italiana del CES-D per la Valutazione Degli Stati Depressivi; Italian Version of CES-D for the Assessment of Depression; Organizzazioni Speciali: Firenze, Italy, 1981. [Google Scholar]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Clements-Nolle, K.; Marx, R.; Guzman, R.; Katz, M. HIV prevalence, risk behaviors, health care use, and mental health status of transgender persons: Implications for public health intervention. Am. J. Public Health 2001, 91, 915–921. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Sica, C.; Coradeschi, D.; Ghisi, M.; Sanavio, E. Beck Anxiety Inventory: Manuale; Manual of the Beck Anxiety Inventory; Organizzazioni Speciali: Firenze, Italy, 2006. [Google Scholar]
- Peveri, L. Resilienza e Regolazione Delle Emozioni. Un Approccio Multimodale; Resilience and Emotions Regulation. A Multimodal Approach. Ph.D. Thesis, Università degli Studi Di Milano-Bicocca, Milano, Italy, 2009. [Google Scholar]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the resilience scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar] [PubMed]
- Graham, J.W. Multiple imputation and analysis with SPSS 17-20. In Missing Data. Analysis and Design; Graham, J.W., Ed.; Springer: New York, NY, USA, 2012; pp. 111–131. ISBN 978-1-4614-4018-5. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 4th ed.; Allyn & Bacon: New York, NY, USA, 2001. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 7th ed.; Muthén & Muthén: Los Angeles, CA, USA, 1998–2012. [Google Scholar]
- Clark, L.A.; Watson, D. Tripartite model of anxiety and depression: Psychometric evidence and taxonomic implications. J. Abnorm. Psychol. 1991, 100, 316–336. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Aiken, L.S.; West, S.G. Multiple Regression: Testing and Interpreting Interactions; Sage: Newbury Park, CA, USA, 1991; ISBN 978-0761907121. [Google Scholar]
- Hayes, A.F. An index and test of linear moderated mediation. Multivar. Behav. Res. 2015, 50, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F.; Scharkow, M. The relative trustworthiness of inferential tests of the indirect effect in statistical mediation analysis: Does method really matter? Psychol. Sci. 2013, 24, 1918–1927. [Google Scholar] [CrossRef] [PubMed]
- White Hughto, J.M.; Reisner, S.L.; Pachankis, J.E. Transgender stigma and health: A critical review of stigma determinants, mechanisms, and interventions. Soc. Sci. Med. 2015, 147, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Beusekom, G.V.; Bos, H.M.W.; Kuyper, L.; Overbeek, G.; Sandfort, T.G.M. Gender nonconformity and mental health among lesbian, gay, and bisexual adults: Homophobic stigmatization and internalized homophobia as mediators. J. Health Psychol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Feinstein, B.A.; Goldfried, M.R.; Davila, J. The relationship between experiences of discrimination and mental health among lesbians and gay men: An examination of internalized homonegativity and rejection sensitivity as potential mechanisms. J. Consult. Clin. Psychol. 2012, 80, 917–927. [Google Scholar] [CrossRef] [PubMed]
- Vitelli, R.; Scandurra, C.; Pacifico, R.; Selvino, M.S.; Picariello, S.; Amodeo, A.L.; Valerio, P.; Giami, A. Trans identities and medical practice in Italy: Self-positioning towards gender affirmation surgery. Sexologies 2017, 26, 43–51. [Google Scholar] [CrossRef]
- Vitelli, R.; Scandurra, C.; Pacifico, R.; Selvino, M.S.; Picariello, S.; Amodeo, A.L.; Valerio, P.; Giami, A. Identifications de genre trans et pratiques médicales en Italie: Positionnement personnel envers les formes de chirurgie de confirmation de genre. Sexologies 2017, 26, 199–204. [Google Scholar] [CrossRef]
- Vitelli, R. Adult male-to-female transsexualism A clinical existential-phenomenological inquiry. J. Phenomenol. Psychol. 2015, 46, 33–68. [Google Scholar] [CrossRef]
- Nuccia, S.; Graifemberghi, S.; El Hamad, I.; Minelli, A.; Magri, S.; Matteelli, A. Prevalence and incidence of syphilis among South American transgender sex workers in Northern Italy. Sex. Transm. Dis. 2006, 33, 334–335. [Google Scholar] [CrossRef]
- Schrock, D.; Holden, D.; Reid, L. Creating emotional resonance: Interpersonal emotion work and motivational framing in a transgender community. Soc. Probl. 2004, 51, 61–81. [Google Scholar] [CrossRef]
- Settineri, S.; Merlo, E.M.; Bruno, A.; Mento, C. Personality assessment in Gender Dysphoria: Clinical observation in psychopathological evidence. Mediterr. J. Clin. Psychol. 2016, 4, 1–15. [Google Scholar] [CrossRef]
- Menvielle, E.; Hill, D.B. An affirmative intervention for families with gender-variant children: A process evaluation. J. Gay Lesbian Ment. Health 2010, 15, 94–123. [Google Scholar] [CrossRef]
- Amodeo, A.L.; Picariello, S.; Valerio, P.; Bochicchio, V.; Scandurra, C. Group psychodynamic counselling with final-year undergraduates in clinical psychology: A clinical methodology to reinforce academic identity and psychological well-being. Psychodyn. Pract. 2017, 23, 161–180. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (N = 149) N (%) or M ± SD | Male to Female (N = 75) N (%) or M ± SD | Female to Male (N = 74) N (%) or M ± SD | p Value |
|---|---|---|---|---|
| Age | 33.18 ± 10.96 | 37.21 ± 12.24 | 29.22 ± 7.77 | <0.001 |
| Ethnicity | 0.368 | |||
| Caucasian | 147 (98) | 74 (98.7) | 73 (98.6) | |
| African | 1 (0.7) | 1 (1.3) | – | |
| Latino | 1 (0.7) | – | 1 (1.4) | |
| Education | 0.552 | |||
| ≤High school | 106 (71.1) | 55 (73.3) | 51 (68.9) | |
| ≥College | 43 (28.9) | 20 (26.7) | 23 (31.1) | |
| Monthly income (€) | 0.492 | |||
| No income | 59 (39.6) | 30 (40) | 29 (39.2) | |
| <600 | 24 (16.1) | 12 (16) | 12 (16.2) | |
| 600–999 | 31 (20.8) | 12 (16) | 19 (25.7) | |
| 1000–1999 | 20 (13.4) | 10 (13.3) | 10 (13.5) | |
| 2000> | 15 (10.1) | 11 (14.6) | 4 (5.4) | |
| Marital status | 0.004 | |||
| Unmarried | 127 (85.2) | 56 (74.7) | 71 (95.9) | |
| Married | 9 (6) | 7 (9.3) | 2 (2.7) | |
| Widowed | 2 (1.3) | 1 (1.3) | 1 (1.4) | |
| Divorced | 3 (2) | 3 (4) | – | |
| Separated | 8 (5.4) | 8 (10.7) | – | |
| Community size | 0.768 | |||
| Urban | 111 (74.5) | 55 (73.3) | 56 (75.7) | |
| Suburban | 19 (12.8) | 9 (12) | 10 (13.5) | |
| Rural | 19 (12.8) | 11 (14.7) | 8 (10.8) | |
| Trans association | 0.788 | |||
| Yes | 58 (38.9) | 30 (40) | 28 (37.8) | |
| No | 91 (61.1) | 45 (60) | 46 (62.2) | |
| Religious education | 0.247 | |||
| Yes | 109 (73.2) | 58 (77.3) | 51 (68.9) | |
| No | 40 (26.8) | 17 (22.7) | 23 (31.1) |
| Main Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | Mean | SD |
| 1. General discrimination | 1 | 12.35 | 2.47 | ||||||||||||||
| 2. Everyday discrimination | 0.65 *** | 1 | 1.92 | 0.73 | |||||||||||||
| 3. Shame | 0.10 | 0.20 * | 1 | 3.39 | 1.57 | ||||||||||||
| 4. Alienation | 0.24 *** | 0.33 *** | 0.37 *** | 1 | 3.42 | 1.78 | |||||||||||
| 5. Anxiety | 0.12 | 0.33 *** | 0.32 *** | 0.33 *** | 1 | 16.36 | 14.89 | ||||||||||
| 6. Depression | 0.19 * | 0.40 *** | 0.43 *** | 0.38 *** | 0.69 *** | 1 | 22.90 | 14.05 | |||||||||
| 7. Resilience | −0.23 *** | −0.34 *** | −0.42 *** | −0.26 *** | −0.29 *** | −0.55 *** | 1 | 5.44 | 1.11 | ||||||||
| Control variables | |||||||||||||||||
| 8. Gender (MtF) | 0.12 | −0.20* | 0.12 | −0.16 | 0.10 | 0.03 | −0.03 | 1 | |||||||||
| 9. Age | 0.02 | 0.01 | −0.24 *** | 0.01 | −0.25 *** | −0.14 | 0.15 | −0.36 *** | 1 | ||||||||
| 10. Education (≤High school) | −0.09 | −0.09 | 0.01 | 0.11 | −0.04 | −0.01 | −0.01 | 0.06 | 0.11 | 1 | |||||||
| 11. Monthly income | −0.22 *** | −0.15 | −0.09 | −0.03 | −0.20 * | −0.21 ** | 0.11 | −03 | 0.34 *** | 0.12 | 1 | ||||||
| 12. Being in a relationship | 0.24 *** | 0.23 ** | 0.11 | −0.21 *** | −0.03 | −0.14 | 0.20 * | 0.32 *** | −0.13 | −0.02 | 0.01 | 1 | |||||
| 13. Community size | 0.06 | 0.03 | 0.04 | 0.01 | −0.01 | 0.04 | 0.05 | −0.05 | 0.01 | −0.05 | −0.09 | 0.05 | 1 | ||||
| 14. Trans association | 0.03 | −0.08 | 0.29 *** | 0.10 | 0.03 | −0.11 | 0.20 * | −0.02 | 0.02 | 0.05 | −0.01 | −0.13 | 0.05 | 1 | |||
| 15. Religious education | −0.04 | −0.07 | −0.01 | 0.03 | −0.07 | −0.09 | 0.05 | 0.10 | −0.14 | −0.04 | −0.10 | −0.04 | −0.16 * | 0.14 | 1 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scandurra, C.; Bochicchio, V.; Amodeo, A.L.; Esposito, C.; Valerio, P.; Maldonato, N.M.; Bacchini, D.; Vitelli, R. Internalized Transphobia, Resilience, and Mental Health: Applying the Psychological Mediation Framework to Italian Transgender Individuals. Int. J. Environ. Res. Public Health 2018, 15, 508. https://doi.org/10.3390/ijerph15030508
Scandurra C, Bochicchio V, Amodeo AL, Esposito C, Valerio P, Maldonato NM, Bacchini D, Vitelli R. Internalized Transphobia, Resilience, and Mental Health: Applying the Psychological Mediation Framework to Italian Transgender Individuals. International Journal of Environmental Research and Public Health. 2018; 15(3):508. https://doi.org/10.3390/ijerph15030508
Chicago/Turabian StyleScandurra, Cristiano, Vincenzo Bochicchio, Anna Lisa Amodeo, Concetta Esposito, Paolo Valerio, Nelson Mauro Maldonato, Dario Bacchini, and Roberto Vitelli. 2018. "Internalized Transphobia, Resilience, and Mental Health: Applying the Psychological Mediation Framework to Italian Transgender Individuals" International Journal of Environmental Research and Public Health 15, no. 3: 508. https://doi.org/10.3390/ijerph15030508
APA StyleScandurra, C., Bochicchio, V., Amodeo, A. L., Esposito, C., Valerio, P., Maldonato, N. M., Bacchini, D., & Vitelli, R. (2018). Internalized Transphobia, Resilience, and Mental Health: Applying the Psychological Mediation Framework to Italian Transgender Individuals. International Journal of Environmental Research and Public Health, 15(3), 508. https://doi.org/10.3390/ijerph15030508