Baduanjin Exercise for Stroke Rehabilitation: A Systematic Review with Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Inclusion Criteria and Study Selection
2.3. Methodological Quality Assessment of Eligible Studies
2.4. Data Extraction and Analysis
3. Results
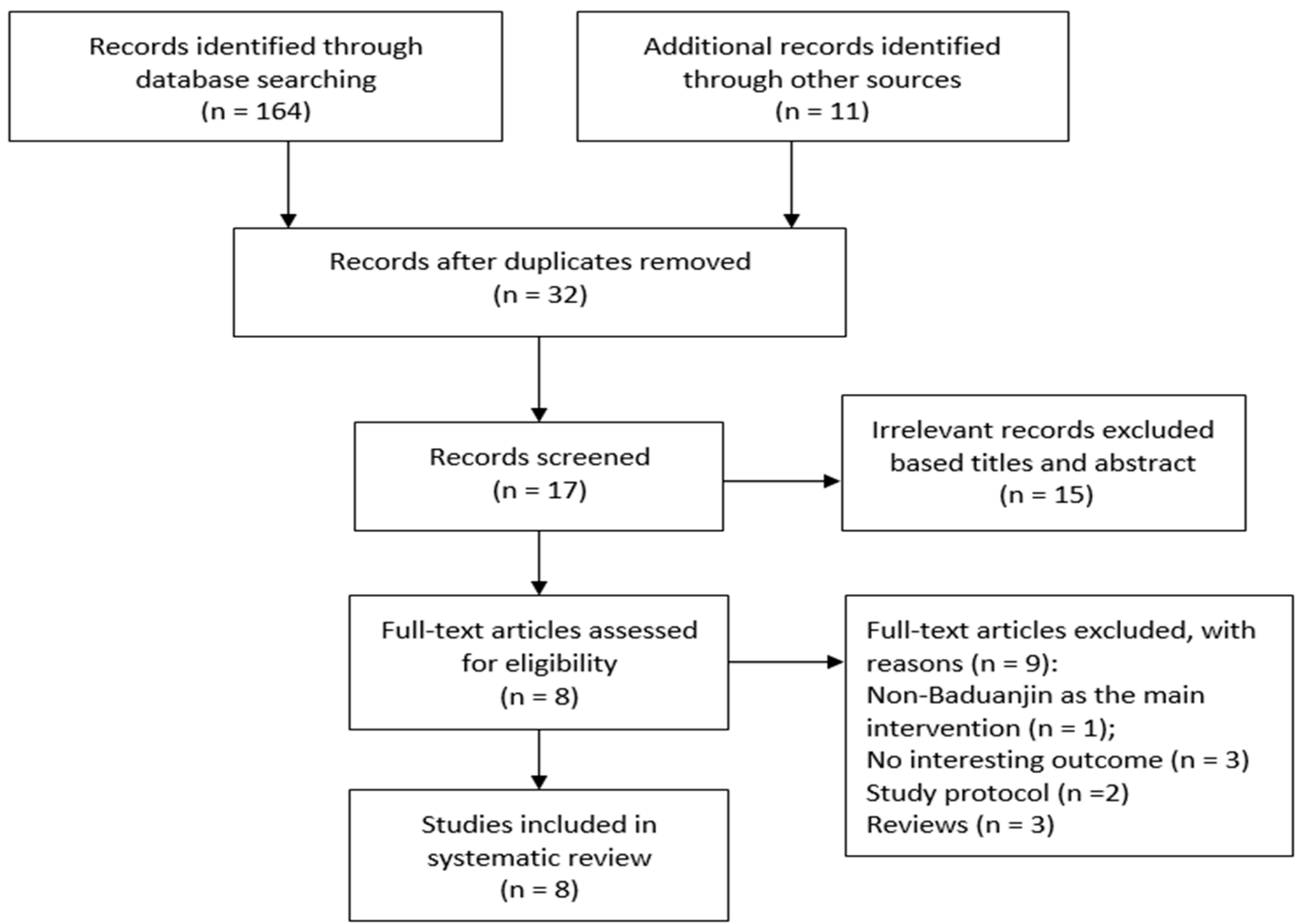
3.1. Study Selection
3.2. Study Characteristics
3.3. Study Quality
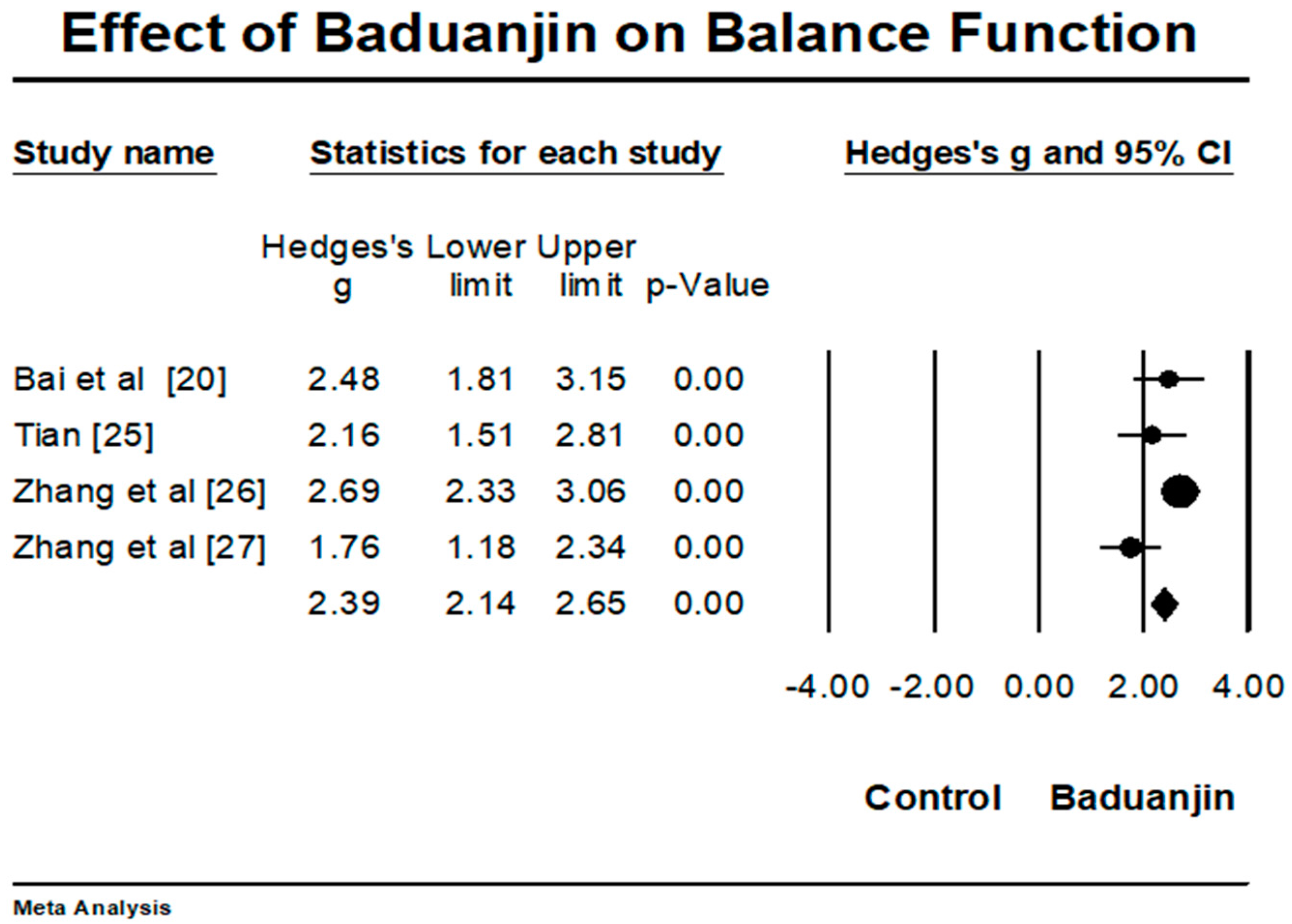
3.4. Effects of Baduanjin on Stroke-Related Outcomes
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mozaffarian, D.; Benjamin, E.; Go, A.; Arnett, D.; Blaha, M.; Cushman, M.; De Ferranti, S.; Despres, J.; Fullerton, H.; Howard, V.; et al. On behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke statistics-2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e32. [Google Scholar] [CrossRef] [PubMed]
- Sarti, C.; Rastenyte, D.; Cepaitis, Z.; Tuomilehto, J. International trends in morality from stroke, 1968–1994. Stroke 2003, 31, 1588–1601. [Google Scholar] [CrossRef]
- Sullivan, K.; Tilson, J.; Cen, S.; Rose, D.; Hershberg, R.; Correa, A.; Gallichio, J.; McLeod, M.; Moore, C.; Wu, S.; et al. Fugl-Meyer assessment of sensorimotor function after stroke: Standardized training procedure for clinical practice and clinical trials. Stroke 2011, 42, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, S. Epidemiology and treatment of post-stroke depression. Neuropsychiatr. Dis. Treat. 2008, 4, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Haghgoo, H.; Pazuki, E.; Hosseini, A.; Rassafiani, M. Depression, activities of daily living and quality of life in patients with stroke. J. Neurol. Sci. 2013, 328, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.; Heiberg, G.; Nielsen, J.; Friborg, O.; Stabel, H.; Anke, A.; Arntzen, C. Validity, reliability and Norwegian adaptation of the stroke-specific quality of life (SS-QOL) scale. SAGE Open Med. 2018, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Wu, B.; Wang, W.; Lee, L.; Zhang, S.; Kong, L. Stroke in China: Epidemiology, prevention, and management strategies. Lancet Neurol. 2007, 6, 456–464. [Google Scholar] [CrossRef]
- Chinese Expert Committee on Rehabilitation after Acute Ischemic Stroke. Expert panel consensus recommendations for the management of rehabilitation after acute ischemic stroke in China. Chin. J. Phys. Med. Rehabil. 2016, 38, 1–6. [Google Scholar]
- Roger, V.; Go, A.; Lloyd-Jones, D.; Benjamin, E.; Berry, J.; Borden, W.; Bravata, D.; Dai, S.; Ford, E.; Fox, E.; et al. Heart disease and stroke statisticsV2012 update: A report from the American Heart Association. Circulation 2012, 1, e2Y220. [Google Scholar]
- Saunders, D.; Greig, C.; Mead, G. Physical activity and exercise after stroke: Review of multiple meaningful benefits. Stroke 2014, 45, 3742–3747. [Google Scholar] [CrossRef] [PubMed]
- Laver, K.; Lange, B.; George, S.; Deutsch, J.; Saposnik, G.; Grotty, M. Virtual reality for stroke rehabilitation. Cochrane Database Syst. Rev. 2017, 11, CD008349. [Google Scholar] [CrossRef] [PubMed]
- Godwin, K.; Wasserman, J.; Ostwald, S. Cost associated with stroke: Outpatient rehabilitative services and medication. Top Stroke Rehabil. 2011, 18, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Chen, K.; Shu, Y.; Chen, X.; Luo, L.; Zhao, X. The Effect of Taichi Practice on Attenuating Bone Mineral Density Loss: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2017, 14, 1000. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M.; Li, T.; Du, G.; Liu, Y. Tai chi for health benefits in patients with multiple sclerosis: A systematic review. PLoS ONE 2017, 12, e0170212. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Pan, Z.; Yeung, A.; Talwar, S.; Wang, C.; Liu, Y.; Shu, Y.; Chen, X. Thomas, G. A review Study on the Beneficial Effects of Baduanjin. J. Altern. Complement. Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Li, T.; Lu, L. Effect of Health-Qigong on spinal mobility and disease activity in people with ankylosing spondylitis. Trav. Hum. 2017, 80, 1585–1597. [Google Scholar]
- Zou, L.; Yeung, A.; Quan, X.; Wang, H. A Systematic review and Meta-analysis of Mindfulness-based (Baduanjin) exercise for alleviating musculoskeletal pain and improving sleep quality in people with chronic diseases. Int. J. Environ. Res. Public Health 2017, 14, 1000. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Quan, X.; Hui, S.-C.; Hu, X.; Chan, J.S.M.; Wang, C.; Boyden, S.D.; Sun, L.; Wang, H. Mindfulness-Based Baduanjin Exercise for Depression and Anxiety in People with Physical or Mental Illnesses: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 321. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Sasaki, J.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M. A systematic review and meta-analysis of Baduanjin Qigong for Health Benefits: Randomized Controlled Trials. Evid. Based Complement. Altern. Med. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Mao, H.; Guo, J.; Zhang, M. Research on Baduanjin combined with function training in improving balance function of stroke patients. Chin. J. Chin. Med. 2011, 26, 1231–1232. (In Chinese) [Google Scholar]
- Cai, W. Influence of sitting Baduanjin on quality of life of cerebral apoplexy patients with sequela in community. J. Nurs. 2010, 24, 2667–2668. [Google Scholar]
- Cai, W.; Liang, C. Effects of sitting Baduanjin on the ability of activities daily living of patients with stroke sequelae in community. J. Nurs. Adm. 2011, 11, 810–811. [Google Scholar]
- Chen, Y.; Li, L.; Wang, M.; Zhang, Y.; Chen, Q. Clinical study on Post stroke depression treated with music therapy of five elements combine with Baduanjin. Shangdong J. Chin. Med. 2017, 36, 23–25. (In Chinese) [Google Scholar]
- Guo, J.; Zhang, M.; Bai, Y.; Feng, X. Effect of Baduanjin clinical outcomes in patients with stroke. Lishizhen Med. Mater. Med. Res. 2013, 24, 2941–2942. (In Chinese) [Google Scholar]
- Tian, H. Effect of Baduanjin on balance function in post-stroke patients. World Newest Med. Inf. Dig. 2017, 17, 251–252. [Google Scholar]
- Zhang, M.; Guo, J.; Bai, Y.; Feng, X. Effect of Baduanjin on balance function among survivors of stroke. Lishizhen Med. Mater. Med. Res. 2013, 24, 2938–2939. (In Chinese) [Google Scholar]
- Zhang, Y.; Li, L. Effect of a combined intervention (Baduanjin and balance training) on balance and sensorimotor function in post-stroke patients. Shangdong J. Chin. Med. 2016, 35, 716–718. (In Chinese) [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Douglas, G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.; Sherrington, C.; Herbert, R.; Moseley, A.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [PubMed]
- Durlak, J. How to select, calculate, and interpret effect size. J. Pediatr. Psychol. 2009, 34, 917–928. [Google Scholar] [CrossRef] [PubMed]
- Xiao, C.; Zhuang, Y. Effect of health Baduanjin for mild to moderate Parkinson’s disease. Geriatr. Gerontol. Int. 2015, 16, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Gao, J.; Yin, B.; Yin, B.; Yang, X.; Bai, D. Effecacy of Baduanjin in improving balance: A study in Chinese community-dwelling older adults. J. Gerontol. Nurs. 2016, 42, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Xiao, C.; Zhuang, Y.; Kang, Y. Effect of Health Qigong Baduanjin on fall prevention in individuals with Parkinson’s disease. J. Am. Geritr. Soc. 2016, 64, 227–228. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.; Li, A.; Ng, S.; Ho, R.; Xu, A.; Yao, T.; Wang, X.; So, K.; Chan, C. Adiponectin potentially contributes to the antdiepressive effects of Baduanjin Qigong exercise in women with chronic fatigue syndrome-like illness. Cell Transpl. 2017, 26, 493–501. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Reference | Location (Language) | Participant Characteristics | Intervention Program | Outcome Measured | Results | Adverse Event | Follow-Up | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Sample Size (Dropout Rate) | Mean Age or Age Range | Course of Disease | Ischemic/Hemorrhage | |||||||
| Bai et al. [20], RCT | Zhengzhou, China (Chinese) | 60 (0%) BJ:30 CG:30 | BJ:53.7 (4.5) CG:51.3 (7.5) | BJ:43.2 (6.53) day CG:38.5 (6.12) day | BJ:18/12 CG:19/11 | BJ: 7 × 40 min/wk, 42 days + balance training CG: balance training | Balance (BBS) | BJ showed significantly greater improvement on balance performance than CG (p < 0.05) | No | No |
| Cai [21], RCT | Shanghai, China (Chinese) | 60 (0%) BJ:30 CG:30 | BJ:60.3 (10.5) CG:61.3 (7.4) | NR | BJ:21/9 CG:24/6 | BJ: 4-to-5 × 30 min/wk, 3 months + educational lessons CG: educational lessons | Quality of life (WHOQOL) | Significant improvements on physical, psychological, and environment domains were only observed in BJ group (p < 0.05), but control group | No | No |
| Cai et al. [22], RCT | Shanghai, China (Chinese) | 60 (0%) BJ:30 CG: 30 | BJ:60.27 (10.48) CG:61.27 (7.42) | BJ:29.7 (7.38) wk CG:28.81 (5.37) wk | BJ:21/9 CG:24/6 | BJ: 4-to-5 × 30 min/wk, 3 months + educational lessons CG: educational lessons | Activities of daily living (Barthel Scale) | Significant improvement in the Barthel Scale was only observed in BJ (p < 0.001), but control group | No | No |
| Chen et al. [23], RCT | Jinan, China (Chinese) | 72 (0%) BJ:36 CG:36 | BJ:52.21 (5.03) CG:51.83 (4.87) | BJ:5.83 (2.09) M CG:6.35 (1.69) M | BJ:20/16 CG:22/14 | BJ1(CG):7 × 30 min/wk, 40 days + general rehabilitation BJ2: BJ + music therapy + general rehabilitation | Depression (HAMD) and quality of life (SF-36) | Both groups showed significant improvements in the two scales (p < 0.05) from baseline to post-test | No | No |
| Guo et al. [24], RCT | Zhengzhou, China, (Chinese) | 224 (1.3%) BJ:115 CG:106 | Age range from 33 to 82 | Course of disease ranged from 1 to 6 months | NR | BJ: 7 × 40 min/wk, 6 weeks + (Bobath techniques and regular drug therapy); CG: Bobath techniques and regular drug therapy | Stroke-related neurologic deficit (NIHSS) | BJ showed significantly greater improvement in the NIHSS than control group (p = 0.001) | No | No |
| Tian [25], RCT | Qingdao, China (Chinese) | 60 (5%) BJ:30 BJ:30 | BJ:54.3 (4.7) CG:53 (4.3) | NR | 60/0 | BJ: 2 × 60–80 min/wk, 12 weeks (group-based self-practice) + general rehabilitation CG: general rehabilitation | Balance (BBS), sensorimotor function (FMA-LE) | BJ showed significantly greater improvement in both BBS and FMA-LE than control group (p < 0.01) | No | No |
| Zhang et al. [26], RCT | Zhengzhou, China, (Chinese) | 224 (1.3%) BJ:115 CG:106 | Age range from 33 to 82 | Course of disease ranged from 1 to 6 months | NR | BJ: 7 × 40 min/wk, 6 weeks + (Bobath techniques and regular drug therapy); CG: Bobath techniques and regular drug therapy | Balance (BBS) | BJ showed significantly greater improvement in the BBS than control group (p < 0.01) | No | No |
| Zhang et al. [27], RCT | Jinan, China (Chinese) | 62 (0%) BJ:31 CG:31 | BJ:55.07 (4.81) CG:46.71 (3.57) | BJ: 6.22 (2.45) wk CG:7.01 (1.89) wk | BJ:21/10 CG:19/12 | BJ:5 × 40 min/wk, 8 weeks + balance training + general rehabilitation CG: balance training + general rehabilitation | Sensorimotor function (FMA-LE) and balance (BBS) | BJ showed significantly greater improvements in the BBS and FMA-LE than control group (p < 0.05) | No | No |
| Reference | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Item 10 | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bai et al. [20] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Cai [21] | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 7/10 |
| Cai et al. [22] | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 7/10 |
| Chen et al. [23] | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 7/10 |
| Guo et al. [24] | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 5/10 |
| Tian [25] | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 5/10 |
| Zhang et al. [26] | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 5/10 |
| Zhang et al. [27] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zou, L.; Wang, C.; Chen, X.; Wang, H. Baduanjin Exercise for Stroke Rehabilitation: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2018, 15, 600. https://doi.org/10.3390/ijerph15040600
Zou L, Wang C, Chen X, Wang H. Baduanjin Exercise for Stroke Rehabilitation: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2018; 15(4):600. https://doi.org/10.3390/ijerph15040600
Chicago/Turabian StyleZou, Liye, Chaoyi Wang, Xiaoan Chen, and Huiru Wang. 2018. "Baduanjin Exercise for Stroke Rehabilitation: A Systematic Review with Meta-Analysis of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 15, no. 4: 600. https://doi.org/10.3390/ijerph15040600
APA StyleZou, L., Wang, C., Chen, X., & Wang, H. (2018). Baduanjin Exercise for Stroke Rehabilitation: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health, 15(4), 600. https://doi.org/10.3390/ijerph15040600