Smoking, Blood Pressure, and Cardiovascular Disease Mortality in a Large Cohort of Chinese Men with 15 Years Follow-up


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Definition of Hypertension
2.3. Definition of Variables
2.4. Statistical Analysis
3. Results
3.1. General Information of the Participants
3.2. Association between Blood Pressure and Outcomes
3.3. Association between Smoking Status and Outcomes
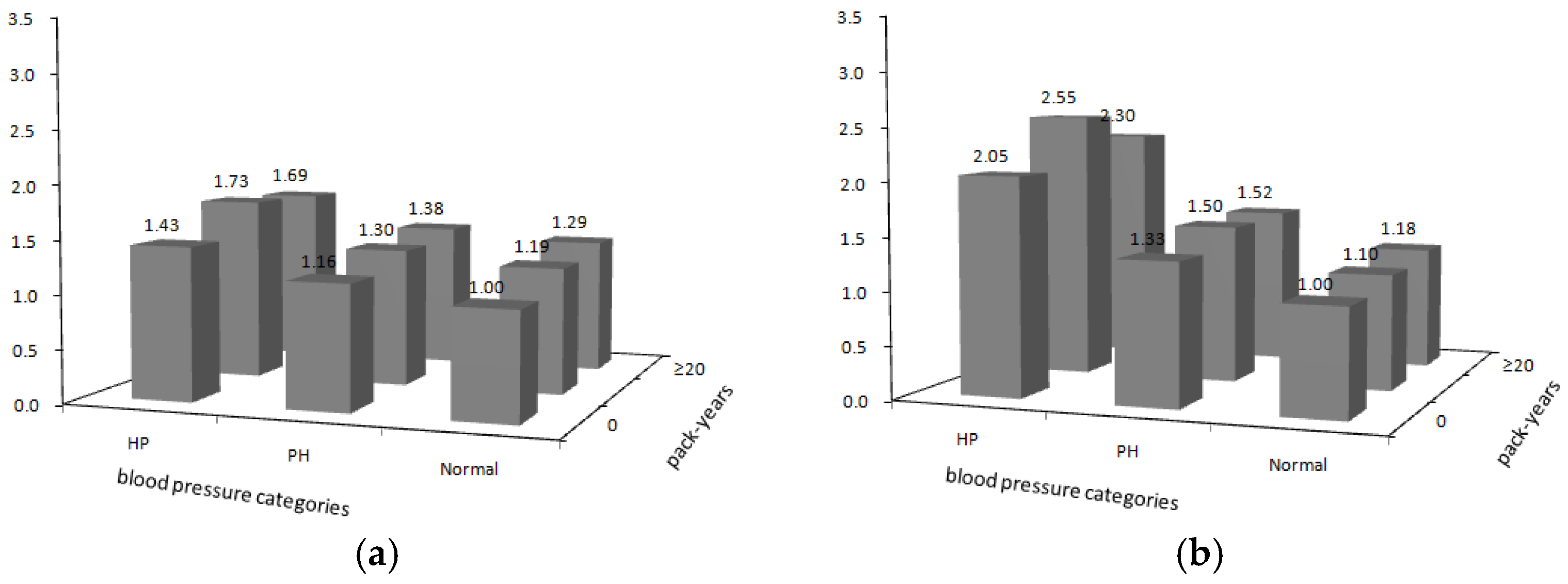
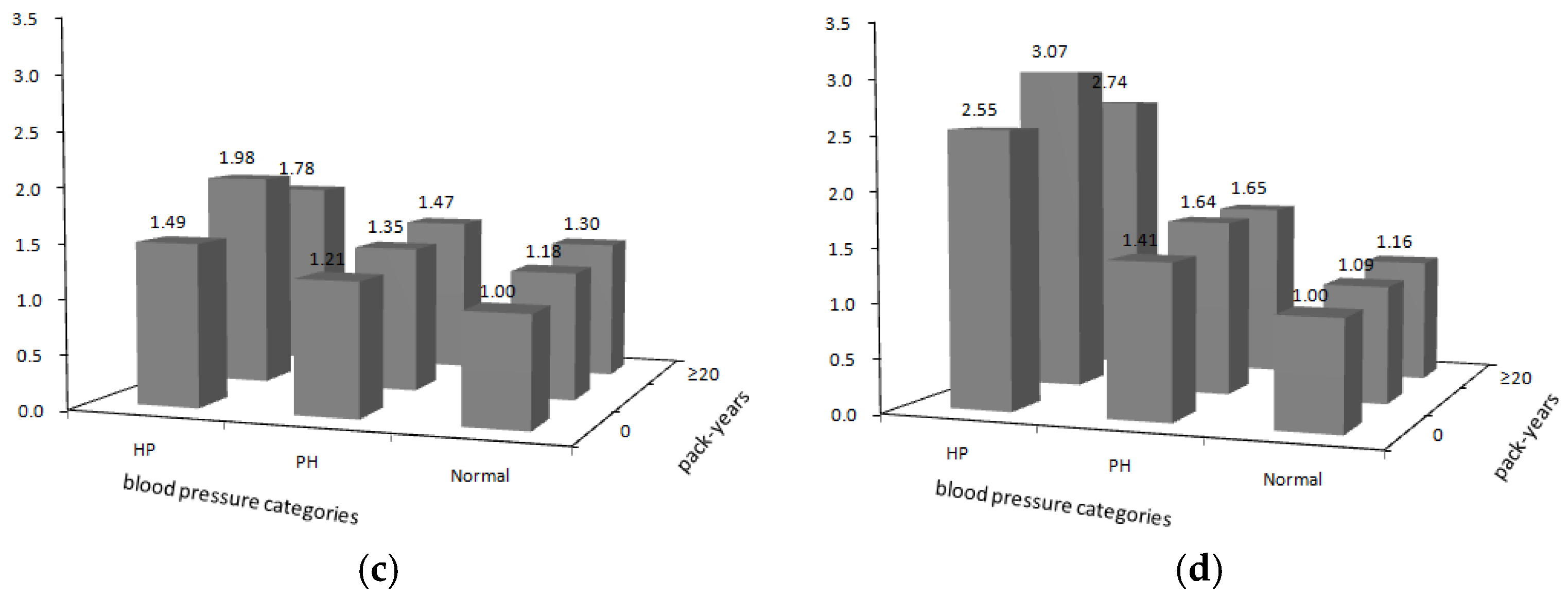
3.4. Association between the Joint Effects and Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar]
- GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar]
- Liu, S.; Zhang, M.; Yang, L.; Li, Y.; Wang, L.; Huang, Z.; Wang, L.; Chen, Z.; Zhou, M. Prevalence and patterns of tobacco smoking among Chinese adult men and women: Findings of the 2010 national smoking survey. J. Epidemiol. Community Health 2017, 71, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Ning, X.; Yang, L.; Lu, H.; Tu, J.; Jin, W.; Zhang, W.; Su, T.C. Trends of hypertension prevalence, awareness, treatment and control in rural areas of northern China during 1991–2011. J. Hum. Hypertens. 2014, 28, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Huxley, R.; Li, L.; Anna, V.; Xie, G.; Yao, C.; Woodward, M.; Li, X.; Chalmers, J.; Gao, R.; et al. Prevalence, awareness, treatment, and control of hypertension in China: Data from the China National Nutrition and Health Survey 2002. Circulation 2008, 118, 2679–2686. [Google Scholar] [CrossRef] [PubMed]
- Franklin, S.S.; Lopez, V.A.; Wong, N.D.; Mitchell, G.F.; Larson, M.G.; Vasan, R.S.; Levy, D. Single versus combined blood pressure components and risk for cardiovascular disease: The Framingham Heart Study. Circulation 2009, 119, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.; Kelly, T.N.; Wu, X.; Chen, J.; Duan, X.; Huang, J.F.; Chen, J.C.; Whelton, P.K.; He, J. Blood pressure and risk of cardiovascular disease in Chinese men and women. Am. J. Hypertens. 2008, 21, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R.; Prospective Studies, C. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [CrossRef]
- Wang, H.; Cao, J.; Li, J.; Chen, J.; Wu, X.; Duan, X.; Huang, J.; Gu, D. Blood pressure, body mass index and risk of cardiovascular disease in Chinese men and women. BMC Public Health 2010, 10, 189. [Google Scholar] [CrossRef] [PubMed]
- Honjo, K.; Iso, H.; Tsugane, S.; Tamakoshi, A.; Satoh, H.; Tajima, K.; Suzuki, T.; Sobue, T. The effects of smoking and smoking cessation on mortality from cardiovascular disease among Japanese: Pooled analysis of three large-scale cohort studies in Japan. Tob. Control 2010, 19, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, D.A.; Song, Y.M.; Sung, J.; Ebrahim, S.; Smith, G.D. The association of smoking and cardiovascular disease in a population with low cholesterol levels: A study of 648,346 men from the Korean national health system prospective cohort study. Stroke J. Cereb. Circ. 2008, 39, 760–767. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Offer, A.; Yang, G.; Smith, M.; Hui, G.; Whitlock, G.; Collins, R.; Huang, Z.; Peto, R.; Chen, Z. Body Mass Index, Blood Pressure, and Mortality From Stroke A Nationally Representative Prospective Study of 212 000 Chinese Men. Stroke 2008, 39, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Liu, L. 2010 Chinese guidelines for the management of hypertension. Zhonghua Xin Xue Guan Bing Za Zhi 2011, 39, 579–615. [Google Scholar] [PubMed]
- Sun, D.; Cao, J.; Liu, X.; Yu, L.; Yao, C.; Li, J.; Yu, D.; Chen, J.; Chen, J.; Wu, X.; et al. Combined effects of smoking and systolic blood pressure on risk of coronary heart disease: A cohort study in Chinese women. J. Womens Health (Larchmt) 2010, 19, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Ge, Z.; Hao, Y.; Cao, J.; Li, J.; Chen, J.; Huang, J.; Wu, X.; Gu, D. Does cigarette smoking exacerbate the effect of blood pressure on the risk of cardiovascular and all-cause mortality among hypertensive patients? J. Hypertens. 2012, 30, 2307–2313. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.J.; Gombojav, B.; Jee, S.H.; Nam, C.M.; Ohrr, H. Gender-specific combined effects of smoking and hypertension on cardiovascular disease mortality in elderly Koreans: The Kangwha Cohort Study. Maturitas 2012, 73, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.G.; Staessen, J.A.; Fagard, R.; Gong, L.; Liu, L. Risks of smoking in treated and untreated older Chinese patients with isolated systolic hypertension. J. Hypertens. 2001, 19, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Hozawa, A.; Ohkubo, T.; Yamaguchi, J.; Ugajin, T.; Koizumi, Y.; Nishino, Y.; Tsubono, Y.; Shibuya, D.; Tsuji, I.; Fukao, A.; et al. Cigarette smoking and mortality in Japan: The Miyagi Cohort Study. J. Epidemiol. 2004, 14 (Suppl. 1), S12–S17. [Google Scholar] [CrossRef] [PubMed]
- Kenfield, S.A.; Stampfer, M.J.; Rosner, B.A.; Colditz, G.A. Smoking and smoking cessation in relation to mortality in women. JAMA 2008, 299, 2037–2047. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Jiang, B.; Li, L.; Li, L.S.; Sun, D.L.; Wu, L.; Liu, M.; He, S.F.; Liang, B.Q.; Hu, F.B.; et al. Changes in smoking behavior and subsequent mortality risk during a 35-year follow-up of a cohort in Xi’an, China. Am. J. Epidemiol. 2014, 179, 1060–1070. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Peto, R.; Zhou, M.; Iona, A.; Smith, M.; Yang, L.; Guo, Y.; Chen, Y.; Bian, Z.; Lancaster, G.; et al. Contrasting male and female trends in tobacco-attributed mortality in China: Evidence from successive nationwide prospective cohort studies. Lancet 2015, 386, 1447–1456. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Pack Years Smoked | |||
|---|---|---|---|---|
| n (%) | 0 | 0.1–19 | 20 | |
| n (%) | 213,221 | 58,583 (27.5) | 51,891 (24.3) | 102,747 (48.2) |
| Age at enrollment (years), mean ± SD | 54.7 ± 10.6 | 55.4 ± 11.1 | 51.3 ± 9.7 | 56.1 ± 10.4 |
| Marital status | ||||
| No | 18,895 (8.9) | 6286 (10.7) | 3518 (6.8) | 9091 (8.9) |
| Yes | 194,326 (91.1) | 52,297 (89.3) | 48,373 (93.2) | 93,656 (91.1) |
| Educational level | ||||
| <6 years | 141,610 (66.4) | 36,263 (61.9) | 31,662 (61.0) | 73,685 (71.7) |
| ≥6 years | 71,611 (33.6) | 22,320 (38.1) | 20,229 (39.0) | 29,062 (28.3) |
| BMI (kg/m2), mean ± SD | 21.8 ± 2.7 | 22.1 ± 2.9 | 22.0 ± 2.7 | 21.4 ± 2.7 |
| Alcohol drinking * | ||||
| 0 | 143,894 (67.6) | 48,322 (82.6) | 34,371 (66.2) | 61,201 (59.6) |
| 0–17 | 31,795 (14.9) | 4916 (8.4) | 10,040 (19.4) | 16,839 (16.4) |
| 18–35 | 19,054 (9.0) | 2591 (4.4) | 4346 (8.4) | 12,117 (11.8) |
| >35 | 18,253 (8.5) | 2676 (4.6) | 3098 (6.0) | 12,479 (12.2) |
| Consumption of fruits and vegetables | ||||
| No | 133,093 (62.4) | 35,190 (60.1) | 30,055 (57.9) | 67,848 (66.0) |
| Yes | 80,128 (37.6) | 23,393 (39.9) | 21,836 (42.1) | 34,899 (34.0) |
| Indoor air pollution | ||||
| No | 35,605 (16.7) | 11,523 (19.7) | 9815 (18.9) | 14,267 (13.9) |
| Yes | 177,616 (83.3) | 47,060 (80.3) | 42,076 (81.1) | 88,480 (86.1) |
| Region | ||||
| South | 115,142 (54.1) | 30,840 (52.6) | 22,813 (44.0) | 61,489 (60.0) |
| North | 98,079 (45.9) | 27,743 (47.4) | 29,078 (56.0) | 41,258 (40.0) |
| Urbanicity | ||||
| Urban | 61,407 (28.9) | 19,517 (33.3) | 17,641 (34.0) | 24,249 (23.6) |
| Rural | 151,814 (71.1) | 39,066 (66.7) | 34,250 (66.0) | 78,498 (76.4) |
| Cause of Death | No. of Death | Adjusted Model (1) | Adjusted Model (2) | Adjusted Model (3) |
|---|---|---|---|---|
| 10-mmHg increase in baseline SBP and DBP | ||||
| SBP | ||||
| All-cause | 52,795 | 1.05 (1.05–1.06) | 1.07 (1.06–1.08) | 1.07 (1.06–1.07) |
| Cardiovascular | 18,833 | 1.15 (1.15–1.16) | 1.16 (1.16–1.17) | 1.16 (1.15–1.17) |
| IHD | 3744 | 1.11 (1.09–1.13) | 1.10 (1.08–1.12) | 1.08 (1.06–1.10) |
| Stroke | 11,288 | 1.19 (1.18–1.20) | 1.20 (1.19–1.21) | 1.20 (1.19–1.21) |
| DBP | ||||
| All-cause | 52,795 | 1.10 (1.10–1.11) | 1.12 (1.12–1.13) | 1.12 (1.11–1.13) |
| Cardiovascular | 18,833 | 1.27 (1.26–1.29) | 1.28 (1.26–1.30) | 1.27 (1.25–1.28) |
| IHD | 3744 | 1.17 (1.14–1.20) | 1.14 (1.11–1.18) | 1.11 (1.08–1.15) |
| Stroke | 11,288 | 1.35 (1.33–1.37) | 1.36 (1.34–1.38) | 1.35 (1.32–1.37) |
| categories of blood pressure in baseline # | ||||
| All-cause | 52,795 | |||
| Prehypertension | 26,533 | 1.09 (1.07–1.11) | 1.10 (1.07–1.13) | 1.08 (1.05–1.11) |
| Hypertension | 10,809 | 1.30 (1.26–1.33) | 1.38 (1.34–1.43) | 1.35 (1.31–1.40) |
| Cardiovascular | 18,833 | |||
| Prehypertension | 9261 | 1.39 (1.34–1.45) | 1.38 (1.32–1.45) | 1.31 (1.25–1.38) |
| Hypertension | 4942 | 2.15 (2.05–2.25) | 2.21 (2.09–2.33) | 2.07 (1.95–2.18) |
| IHD | 3744 | |||
| Prehypertension | 1933 | 1.33 (1.22–1.45) | 1.26 (1.14–1.40) | 1.14 (1.03–1.27) |
| Hypertension | 906 | 1.79 (1.62–1.99) | 1.68 (1.48–1.89) | 1.47 (1.30–1.66) |
| Stroke | 11,288 | |||
| Prehypertension | 5435 | 1.56 (1.48–1.65) | 1.56 (1.46–1.66) | 1.46 (1.37–1.55) |
| Hypertension | 3161 | 2.70 (2.54–2.87) | 2.76 (2.57–2.97) | 2.51 (2.33–2.70) |
| No. of Death | HR | No. of Death | HR | No. of Death | HR | p for Trend | |
|---|---|---|---|---|---|---|---|
| 0 | pack years 0.1–19 | pack years ≥ 20 | |||||
| All-cause | 12,295 | 1 | 9097 | 1.15 (1.12–1.18) | 27,418 | 1.21 (1.18–1.24) | <0.0001 |
| CVD | 4586 | 1 | 3324 | 1.14 (1.09–1.20) | 9370 | 1.14 (1.10–1.19) | <0.0001 |
| IHD | 963 | 1 | 720 | 1.17 (1.06–1.30) | 1825 | 1.22 (1.13–1.33) | <0.0001 |
| Stroke | 2661 | 1 | 2015 | 1.15 (1.08–1.22) | 5540 | 1.14 (1.08–1.19) | <0.0001 |
| Never | Former | Current | |||||
| All-cause | 13,059 | 1 | 4297 | 1.30 (1.25–1.34) | 35,439 | 1.18 (1.15–1.20) | - |
| CVD | 4905 | 1 | 1519 | 1.19 (1.12–1.26) | 12,409 | 1.13 (1.10–1.17) | - |
| IHD | 1005 | 1 | 376 | 1.35 (1.19–1.52) | 2363 | 1.19 (1.10–1.29) | - |
| Stroke | 2889 | 1 | 868 | 1.17 (1.08–1.26) | 7531 | 1.13 (1.08–1.18) | - |
| 0 | years ≤ 20 | years > 20 | |||||
| All-cause | 12,470 | 1 | 2427 | 1.05 (1.00–1.10) | 34,039 | 1.21 (1.18–1.23) | <0.0001 |
| CVD | 4653 | 1 | 823 | 1.10 (1.02–1.19) | 11,860 | 1.15 (1.11–1.19) | <0.0001 |
| IHD | 986 | 1 | 196 | 1.13 (0.96–1.34) | 2344 | 1.20 (1.11–1.30) | <0.0001 |
| Stroke | 2696 | 1 | 482 | 1.11 (1.00–1.23) | 7071 | 1.15 (1.10–1.20) | <0.0001 |
| 0 < pack ≤ 1 | 1 < packs ≤ 2 | packs > 2 | |||||
| All-cause | 9389 | 1 | 17,618 | 1.05 (1.02–1.07) | 9508 | 1.01 (0.98–1.04) | <0.0001 |
| CVD | 3494 | 1 | 6098 | 1.02 (0.98–1.06) | 3102 | 0.96 (0.92–1.01) | <0.0001 |
| IHD | 765 | 1 | 1245 | 1.06 (0.97–1.16) | 535 | 0.93 (0.83–1.05) | <0.0001 |
| Stroke | 2055 | 1 | 3632 | 1.03 (0.97–1.08) | 1868 | 1.00 (0.93–1.06) | <0.0001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, J.; Zhang, X.; Wang, W.; Yin, P.; Guo, X.; Zhou, M. Smoking, Blood Pressure, and Cardiovascular Disease Mortality in a Large Cohort of Chinese Men with 15 Years Follow-up. Int. J. Environ. Res. Public Health 2018, 15, 1026. https://doi.org/10.3390/ijerph15051026
Tan J, Zhang X, Wang W, Yin P, Guo X, Zhou M. Smoking, Blood Pressure, and Cardiovascular Disease Mortality in a Large Cohort of Chinese Men with 15 Years Follow-up. International Journal of Environmental Research and Public Health. 2018; 15(5):1026. https://doi.org/10.3390/ijerph15051026
Chicago/Turabian StyleTan, Jibin, Xiumin Zhang, Weihua Wang, Peng Yin, Xiaomin Guo, and Maigeng Zhou. 2018. "Smoking, Blood Pressure, and Cardiovascular Disease Mortality in a Large Cohort of Chinese Men with 15 Years Follow-up" International Journal of Environmental Research and Public Health 15, no. 5: 1026. https://doi.org/10.3390/ijerph15051026
APA StyleTan, J., Zhang, X., Wang, W., Yin, P., Guo, X., & Zhou, M. (2018). Smoking, Blood Pressure, and Cardiovascular Disease Mortality in a Large Cohort of Chinese Men with 15 Years Follow-up. International Journal of Environmental Research and Public Health, 15(5), 1026. https://doi.org/10.3390/ijerph15051026