Effects of Environmental Air Pollution on Pulmonary Function Level of Residents in Korean Industrial Complexes

 , and
, and
Abstract
:1. Introduction
2. Methods and Materials
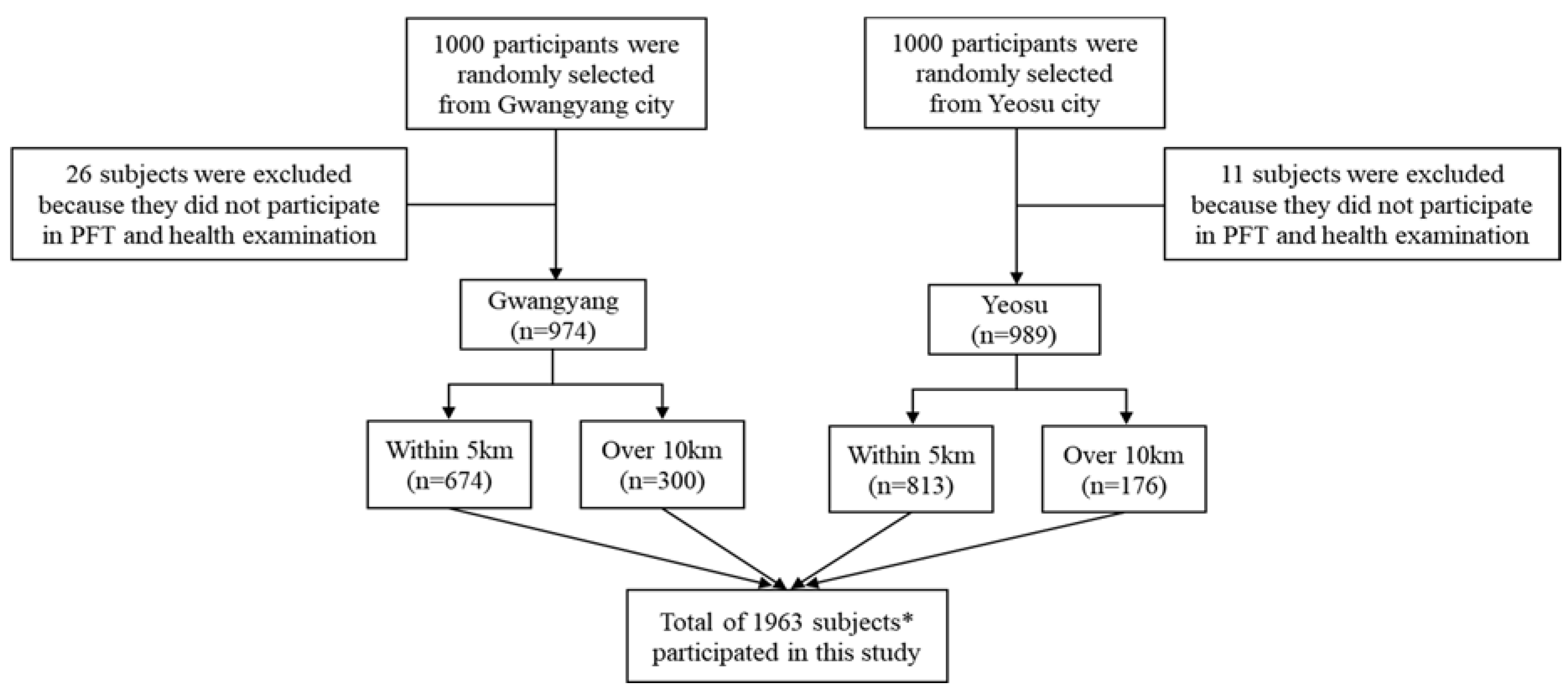
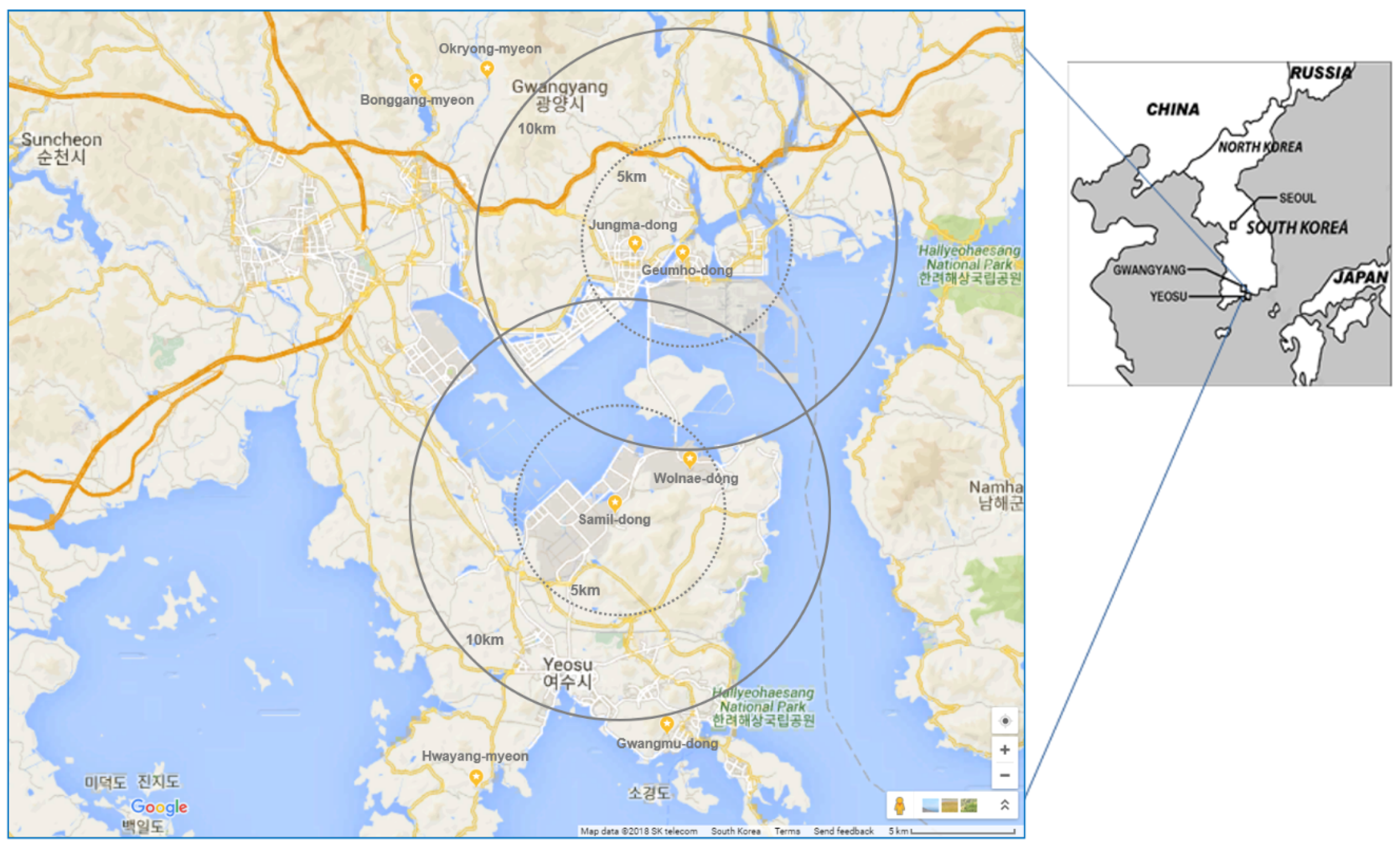
2.1. Study Subject
2.2. Questionnaire Survey
2.3. Pulmonary Function Test
2.4. Collection of Air-Monitoring Data
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Shin, J.-S.; Jeon, S.-R. A comparative study on the health status of the elementary students living in a certain industrial area and a certain residential area in Busan. J. Korean Soc. School Health 2002, 15, 263–275. [Google Scholar]
- Ahn, J. A Study on Relationship between Ambient Air Pollutants and Pulmonary Function in the Seoul Area; Graduate School of Hanyang University: Seoul, Korea, 2002. [Google Scholar]
- Lee, J.-T.; Cho, Y.-S.; Son, J.-Y.; Lee, J.-W.; Lee, S.-J.; Chung, Y.-H.; Kim, D.-S.; Yu, S.-D.; Ahn, S.-C. A study of monitoring method on exposure level and biomarkers of environmental pollutants-focused on Ulsan industrial complex area. Korean J. Environ. Health Sci. 2008, 34, 188–198. [Google Scholar] [CrossRef]
- Han, S.-H.; Park, J.-S.; Seo, S.-H.; Yoon, J.-E.; Jee, S.-H. Factors affecting the morbidity related to respiratory dieseases in urban Korea. Korea J. Popul. Stud. 2005, 28, 205–217. [Google Scholar]
- Yu, S.-D.; Cha, J.-H.; Kim, D.-S.; Lee, J.-T. Effects of fine particles on pulmonary function of elementary school children in Ulsan. Korean J. Environ. Health Sci. 2007, 33, 365–371. [Google Scholar] [CrossRef]
- Choi, J.K.; Kang, S.H.; Park, Y.H.; Bae, Y.J.; Kim, T.B.; Lee, T.H.; Park, C.S.; Moon, H.B.; Cho, S.H.; Park, H.W. Pulmonary function and clinical characteristics influenced by cigarette smoking among adult asthmatics. Korean J. Asthma Allergy Clin. Immunol. 2008, 28, 263–270. [Google Scholar]
- Jung, J.-H.; Choi, B.-W.; Kim, M.-H.; Baek, S.-O.; Lee, G.-W.; Shon, B.-H. The characteristics of the appearance and health risks of volatile organic compounds in industrial (Pohang, Ulsan) and non-industrial (Gyeongju) areas. Environ. Health Toxicol. 2012, 27, e2012012. [Google Scholar] [CrossRef] [PubMed]
- Joo, Y.; Roh, S. Exposure assessment of heavy metals using exposure biomarkers among residents living near a chungcheongnam-do province industrial complex area. Korean J. Environ. Health Sci. 2016, 42, 213–223. [Google Scholar] [CrossRef]
- Ahn, S.-C.; Kim, D.-S.; Yu, H.-Y.; Kwon, Y.-M.; Zoo, D.-H. A study on the allergen skin test prevalence in the residents of a non-industrial area. Korean J. Environ. Health Sci. 2012, 38, 398–406. [Google Scholar] [CrossRef]
- Seo, J.; Youn, D.; Kim, J.; Lee, H. Extensive spatiotemporal analyses of surface ozone and related meteorological variables in South Korea for the period 1999–2010. Atmos. Chem. Phys. 2014, 14, 6395–6415. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.-H.; Lee, G.-W.; Yang, J.-Y.; Jeon, J.-M.; Lee, W.-S.; Lim, J.-Y.; Lee, H.-S.; Gwak, Y.-K.; Shin, D.-C.; Lim, Y.-W. Indoor exposure and health risk of polycyclic aromatic hydrocarbons (pahs) via public facilities pm 2.5, Korea (II). Asian J. Atmos. Environ. 2014, 8, 35–47. [Google Scholar] [CrossRef]
- 1Park, H.; Lee, K.; Moon, C.-S.; Woo, K.; Kang, T.-S.; Chung, E.-K.; Son, B.-S. Simultaneous exposure to heavy metals among residents in the industrial complex: Korean national cohort study. Int. J. Environ. Res. Public Health 2015, 12, 5905–5917. [Google Scholar]
- Kang, B.-W.; Lee, H.-S.; Kim, J.-H.; Hong, J.-H.; Kim, R.-H.; Seo, Y.-K.; Han, J.-S.; Baek, K.-M.; Kim, M.-J.; Baek, S.-O. Distribution of airborne hexavalent chromium concentrations in large industrial complexes in Korea. Asian J. Atmos. Environ. 2016, 10, 208–216. [Google Scholar] [CrossRef]
- Jung, S.-W.; Lee, K.; Cho, Y.-S.; Choi, J.-H.; Yang, W.; Kang, T.-S.; Park, C.; Kim, G.-B.; Yu, S.-D.; Son, B.-S. Association by spatial interpolation between ozone levels and lung function of residents at an industrial complex in South Korea. Int. J. Environ. Res. Public Health 2016, 13, 728. [Google Scholar] [CrossRef] [PubMed]
- Seo, W.; Chang, S.; Kwon, H. Concentration of air pollutants and asthma in Taejon city. Korean J. Environ. Health 2000, 26, 80–90. [Google Scholar]
- Choi, J.-H.; Xu, Q.-S.; Park, S.-Y.; Kim, J.-H.; Hwang, S.-S.; Lee, K.-H.; Lee, H.-J.; Hong, Y.-C. Seasonal variation of effect of air pollution on blood pressure. J. Epidemiol. Community Health 2007, 61, 314–318. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.S.; Kim, Y.S.; Kim, J.H.; Son, B.S.; Kim, D.S.; Yang, W. Respiratory health effects among schoolchildren and their relationship to air pollutants in Korea. Int. J. Environ. Health Res. 2009, 19, 31–48. [Google Scholar] [CrossRef] [PubMed]
- Song, H.I. Effect of air pollution on childhood asthma living in Seoul. J. Asthma Allergy Clin. Immunol. 2001, 21, 28–39. [Google Scholar]
- Lee, J.-T.; Son, J.-Y.; Cho, Y.-S. The adverse effects of fine particle air pollution on respiratory function in the elderly. Sci. Total Environ. 2007, 385, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.-J.; Hong, S.-J. Ambient air pollution and allergic diseases in children. Korean J. Pediatr. 2012, 55, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-H.; Jahan, S.A.; Kabir, E. A review on human health perspective of air pollution with respect to allergies and asthma. Environ. Int. 2013, 59, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Bae, K.W.; Kim, Y.S.; Park, J.S.; Lee, K.Y.; Kwon, H.J.; Lee, S.R.; Jee, Y.K. Changes of lung function and symptoms of asthmatics according to the concentration of on-site measured NO2. Korean J. Asthma Allergy Clin. Immunol. 2004, 24, 324–330. [Google Scholar]
- Bae, H.-J.; Kim, M.-H.; Lee, A.-K.; Park, J.-I. Acute effects of PM10 on asthma hospitalization among children and benefit analysis at four major cities in Korea. Korean J. Environ. Health Sci. 2009, 35, 1–10. [Google Scholar] [CrossRef]
- Na, W.T.; Park, J.H.; Lee, G.E.; Kwon, S.J.; Son, J.W.; Na, M.J.; Choi, E.G. Comparison of spirometry with cardiopulmonary exercise test of chronic obstructive pulmonary disease. Korean J. Med. 2009, 76, 571–577. [Google Scholar]
- Choi, J.K.; Paek, D.; Lee, J.O. Normal predictive values of spirometry in Korean population. Tuberc. Respir. Dis. 2005, 58, 230–242. [Google Scholar] [CrossRef]
- Kim, D.S.; Kim, Y.S.; Jung, K.-S.; Chang, J.H.; Lim, C.-M.; Lee, J.H.; Uh, S.-T.; Shim, J.J.; Lew, W.J. Prevalence of chronic obstructive pulmonary disease in Korea: A population-based spirometry survey. Am. J. Respir. Crit. Care Med. 2005, 172, 842–847. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Lim, Y.H.; Kyung, S.Y.; An, C.H.; Lee, S.P.; Jeong, S.H.; Ju, Y.S. Effects of ambient particulate matter on peak expiratory flow rates and respiratory symptoms of asthmatics during asian dust periods in Korea. Respirology 2005, 10, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Kwon, S.Y.; Yoon, J.W.; Kim, S.Y.; Choi, S.H.; Park, Y.J.; Yoon, H.I.; Chang, Y.S.; Lee, J.H.; Lee, C.T.; et al. Association between body composition and pulmonary function in elderly people: The Korean longitudinal study on health and aging. Obesity 2011, 19, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Cooper, B. Spirometry standards and FEV1/FVC repeatability. Prim. Care Respir. J. 2010, 19, 292. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-T.; Shin, D.; Chung, Y. Air pollution and daily mortality in Seoul and Ulsan, Korea. Environ. Health Perspect. 1999, 107, 149. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.-J.; Cho, S.-H.; Chun, Y.; Lagarde, F.; Pershagen, G. Effects of the asian dust events on daily mortality in Seoul, Korea. Environ. Res. 2002, 90, 1–5. [Google Scholar] [CrossRef] [PubMed]
- 3Son, J.-Y.; Bell, M.L.; Lee, J.-T. Individual exposure to air pollution and lung function in Korea: Spatial analysis using multiple exposure approaches. Environ. Res. 2010, 110, 739–749. [Google Scholar]
- Kim, S.H.; Kim, J.W.; Kim, J.E.; Son, B.C.; Kim, J.H.; Lee, C.H.; Jang, S.H.; Lee, C.K. Pulmonary function and respiratory symptoms of municipal fire officers in Busan. Korean J. Occup. Environ. Med. 2006, 18, 103–111. [Google Scholar]
- Smargiassi, A.; Goldberg, M.S.; Wheeler, A.J.; Plante, C.; Valois, M.-F.; Mallach, G.; Kauri, L.M.; Shutt, R.; Bartlett, S.; Raphoz, M.; et al. Associations between personal exposure to air pollutants and lung function tests and cardiovascular indices among children with asthma living near an industrial complex and petroleum refineries. Environ. Res. 2014, 132, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.L.; Coates, A.L.; To, T. Exposure to industrial air pollutant emissions and lung function in children: Canadian health measures survey, 2007 to 2011. Health Rep. 2016, 27, 3. [Google Scholar] [PubMed]
- Kurt, O.K.; Zhang, J.; Pinkerton, K.E. Pulmonary health effects of air pollution. Curr. Opin. Pulm. Med. 2016, 22, 138. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.-S.; Lee, S.-H.; Yang, M.-S.; Lee, S.-M.; Kim, S.-H.; Kim, D.-I.; Sohn, S.-W.; Park, C.-H.; Park, H.-W.; Kim, S.-S.; et al. Correlation between the Korean version of asthma control test and health-related quality of life in adult asthmatics. J. Korean Med. Sci. 2008, 23, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-T.; Kim, H.; Song, H.; Hong, Y.-C.; Cho, Y.-S.; Shin, S.-Y.; Hyun, Y.-J.; Kim, Y.-S. Air pollution and asthma among children in Seoul, Korea. Epidemiology 2002, 13, 481–484. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pollutant | Gwangyang (n = 277) | Yeosu (n = 209) | Total (n = 486) | Legal Limit ∮ | Unit | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Exposed † (n = 138) | Control ‡ (n = 139) | p-Value | Exposed † (n = 140) | Control ‡ (n = 69) | p-Value | Exposed † (n = 278) | Control ‡ (n = 208) | p-Value | |||||||||||||||
| n | AM | SD | n | AM | SD | n | AM | SD | n | AM | SD | n | AM | SD | n | AM | SD | ||||||
| SO2 (n = 97) | 27 | 0.011 | 0.003 | 28 | 0.005 | 0.001 | 0.01 * | 28 | 0.013 | 0.004 | 14 | 0.008 | 0.003 | 0.01 * | 55 | 0.012 | 0.004 | 42 | 0.006 | 0.003 | 0.01 * | 0.05 | ppm |
| CO (n = 97) | 28 | 0.739 | 0.249 | 27 | 0.443 | 0.112 | 0.00 * | 28 | 0.557 | 0.233 | 14 | 0.535 | 0.198 | 0.77 | 56 | 0.648 | 0.256 | 41 | 0.478 | 0.151 | 0.00 * | 9 | ppm |
| NO2 (n = 98) | 28 | 0.020 | 0.005 | 28 | 0.012 | 0.004 | 0.00 * | 28 | 0.020 | 0.005 | 14 | 0.016 | 0.005 | 0.22 | 56 | 0.020 | 0.005 | 42 | 0.014 | 0.005 | 0.03 * | 0.06 | ppm |
| O3 (n = 97) | 27 | 0.034 | 0.009 | 28 | 0.009 | 0.008 | 0.03 * | 28 | 0.033 | 0.007 | 14 | 0.007 | 0.008 | 0.02 * | 55 | 0.034 | 0.008 | 42 | 0.008 | 0.008 | 0.02 * | 0.06 | ppm |
| PM10 (n = 97) | 28 | 39.39 | 7.20 | 28 | 36.50 | 11.74 | 0.27 | 28 | 46.75 | 13.00 | 13 | 35.31 | 12.05 | 0.00 * | 56 | 43.07 | 11.06 | 41 | 36.12 | 11.70 | 0.00 * | 100 | μg/m3 |
| Variable | Gwangyang (n = 974) (%) | Yeosu (n = 989) (%) | Total (n = 1963) (%) |
|---|---|---|---|
| Sex | |||
| Male | 438 (45.0) | 361 (36.5) | 799 (40.7) |
| Female | 536 (55.0) | 628 (63.5) | 1164 (59.3) |
| Age | |||
| <9 | 18 (1.8) | 49 (5.0) | 67 (3.4) |
| 10–19 | 325 (33.4) | 314 (31.7) | 639 (32.6) |
| 20–39 | 70 (7.2) | 87 (8.8) | 157 (8.0) |
| 40–59 | 308 (31.6) | 193 (19.5) | 501 (25.5) |
| >60 | 253 (26.0) | 346 (35.0) | 599 (30.5) |
| Distance from industrial complexes | |||
| ≤5 km † | 674 (69.2) | 813 (82.2) | 1487 (75.8) |
| >10 km ‡ | 300 (30.8) | 176 (17.8) | 476 (24.2) |
| BMI | |||
| <18.5 | 169 (17.4) | 224 (22.6) | 393 (20.0) |
| 18.5–22.9 | 593 (60.9) | 555 (56.1) | 1148 (58.5) |
| 23–24.9 | 190 (19.5) | 183 (18.5) | 373 (19.0) |
| >25 | 22 (2.3) | 27 (2.7) | 49 (2.5) |
| Alcohol * | |||
| No | 607 (62.3) | 618 (62.5) | 1225 (62.4) |
| Yes | 303 (31.1) | 233 (23.6) | 536 (27.3) |
| Smoking * | |||
| No | 684 (70.2) | 696 (70.4) | 1380 (70.3) |
| Yes | 150 (15.4) | 79 (8.0) | 229 (11.7) |
| Secondhand smoke * | |||
| No | 426 (43.7) | 372 (37.6) | 798 (40.7) |
| Yes | 356 (36.6) | 366 (37.0) | 722 (36.8) |
| Variable | Gwangyang (n = 974) | Yeosu (n = 989) | Total (n = 1963) | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | FEV1 | FVC | FEV1/FVC | n | FEV1 | FVC | FEV1/FVC | n | FEV1 | FVC | FEV1/FVC | ||||||||||
| AM | SD | AM | SD | AM | SD | AM | SD | AM | SD | AM | SD | AM | SD | AM | SD | AM | SD | ||||
| Total | 974 | 101.10 | 23.30 | 98.49 | 19.42 | 81.27 | 9.27 | 989 | 107.08 | 23.68 | 100.74 | 19.27 | 83.26 | 9.62 | 1963 | 104.91 | 24.83 | 101.60 | 20.82 | 81.80 | 9.84 |
| Sex | |||||||||||||||||||||
| Male | 438 | 99.35 | 21.15 | 99.64 | 19.29 | 80.37 | 9.10 | 361 | 103.38 | 20.78 | 101.64 | 17.30 | 81.56 | 10.55 | 799 | 101.26 | 21.26 | 100.58 | 18.36 | 80.98 | 9.79 |
| Female | 536 | 102.55 | 24.91 | 97.56 | 19.52 | 81.59 | 9.35 | 628 | 109.21 | 24.96 | 100.22 | 20.30 | 84.24 | 8.91 | 1164 | 105.67 | 24.84 | 99.76 | 20.18 | 82.79 | 9.16 |
| p-value | 0.03 * | 0.10 | 0.23 | 0.01 * | 0.26 | 0.01 * | 0.01 * | 0.35 | 0.14 | ||||||||||||
| Distance from industrial complexes | |||||||||||||||||||||
| >10 km † | 300 | 105.47 | 25.05 | 101.91 | 20.26 | 81.41 | 8.48 | 176 | 107.26 | 24.47 | 102.85 | 18.24 | 83.67 | 9.65 | 476 | 107.25 | 28.33 | 104.89 | 22.90 | 81.10 | 10.14 |
| ≤5 km ‡ | 674 | 99.17 | 22.29 | 96.98 | 18.86 | 80.97 | 9.59 | 813 | 107.05 | 23.52 | 100.28 | 19.46 | 83.17 | 9.62 | 1487 | 103.95 | 23.17 | 100.23 | 19.74 | 82.09 | 9.70 |
| p-value | 0.01 * | 0.01 * | 0.11 | 0.92 | 0.10 | 0.54 | 0.03 * | 0.01 * | 0.40 | ||||||||||||
| BMI (kg/m2) | |||||||||||||||||||||
| <18.5 | 169 | 89.77 | 17.62 | 94.06 | 16.57 | 84.37 | 8.87 | 224 | 95.40 | 17.68 | 96.79 | 17.16 | 86.23 | 9.42 | 393 | 92.34 | 17.64 | 95.26 | 16.97 | 85.46 | 9.12 |
| 18.5–22.9 | 593 | 102.88 | 23.78 | 99.36 | 19.60 | 80.59 | 9.76 | 555 | 109.71 | 24.76 | 101.49 | 18.97 | 82.52 | 9.83 | 1148 | 105.69 | 24.19 | 100.69 | 19.10 | 81.34 | 9.79 |
| 23–24.9 | 190 | 105.66 | 23.75 | 99.65 | 20.09 | 80.67 | 7.46 | 183 | 112.41 | 22.30 | 102.24 | 19.49 | 82.33 | 8.54 | 373 | 107.97 | 23.06 | 101.26 | 19.74 | 81.46 | 8.04 |
| >25 | 22 | 101.38 | 20.78 | 99.29 | 25.05 | 81.14 | 8.61 | 27 | 113.87 | 23.09 | 107.69 | 32.18 | 80.24 | 9.21 | 49 | 108.46 | 21.97 | 103.45 | 28.95 | 80.68 | 8.89 |
| p-value | 0.01 * | 0.01 * | 0.01 * | 0.01 * | 0.01 * | 0.01 * | 0.01 * | 0.01 * | 0.01 * | ||||||||||||
| Alcohol | |||||||||||||||||||||
| No | 607 | 102.34 | 22.15 | 98.99 | 20.87 | 81.82 | 9.50 | 618 | 109.79 | 23.66 | 100.67 | 20.05 | 83.78 | 9.28 | 1225 | 105.54 | 21.24 | 99.46 | 20.43 | 81.41 | 9.42 |
| Yes | 303 | 100.47 | 24.22 | 98.06 | 18.91 | 79.95 | 8.63 | 233 | 107.52 | 23.74 | 100.99 | 19.34 | 81.37 | 10.69 | 536 | 103.76 | 22.63 | 99.68 | 19.04 | 80.57 | 9.56 |
| p-value | 0.24 | 0.50 | 0.01 * | 0.22 | 0.83 | 0.01 * | 0.01 * | 0.78 | 0.55 | ||||||||||||
| Smoking | |||||||||||||||||||||
| No | 684 | 101.16 | 22.01 | 99.18 | 20.04 | 79.17 | 9.19 | 696 | 109.09 | 24.45 | 101.56 | 16.41 | 78.69 | 11.39 | 1380 | 105.36 | 23.16 | 100.23 | 18.64 | 78.98 | 10.46 |
| Yes | 150 | 100.98 | 24.21 | 98.30 | 19.91 | 81.41 | 9.35 | 79 | 107.28 | 21.80 | 100.86 | 19.81 | 83.77 | 9.47 | 229 | 104.14 | 22.33 | 99.84 | 21.42 | 82.59 | 9.41 |
| p-value | 0.93 | 0.63 | 0.01 * | 0.49 | 0.73 | 0.01 * | 0.36 | 0.43 | 0.01 * | ||||||||||||
| Secondhand Smoke | |||||||||||||||||||||
| No | 356 | 105.48 | 25.26 | 99.42 | 20.25 | 80.39 | 9.97 | 372 | 112.09 | 26.52 | 98.93 | 20.39 | 81.15 | 9.42 | 728 | 108.59 | 25.10 | 99.12 | 20.31 | 80.98 | 9.79 |
| Yes | 426 | 97.25 | 22.44 | 98.53 | 19.88 | 81.77 | 8.86 | 366 | 105.29 | 21.08 | 102.43 | 18.64 | 83.16 | 10.05 | 792 | 103.46 | 21.89 | 100.21 | 19.26 | 82.36 | 9.58 |
| p-value | 0.01 * | 0.54 | 0.04 * | 0.01 * | 0.16 | 0.45 | 0.01 * | 0.39 | 0.17 | ||||||||||||
| Variable | Gwangyang (n = 974) | Yeosu (n = 989) | Total (n = 1963) | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | FEV1 | FVC | FEV1/FVC | n | FEV1 | FVC | FEV1/FVC | n | FEV1 | FVC | FEV1/FVC | ||||||||||
| AM | SD | AM | SD | AM | SD | AM | SD | AM | SD | AM | SD | AM | SD | AM | SD | AM | SD | ||||
| Within a radius of 5 km from industrial complexes | |||||||||||||||||||||
| <9 | 18 | 98.50 | 12.01 | 102.72 | 12.76 | 86.59 | 7.97 | 38 | 96.84 | 12.48 | 99.32 | 13.16 | 87.80 | 7.88 | 56 | 97.38 | 12.24 | 100.41 | 13.02 | 87.41 | 7.64 |
| 10–19 | 218 | 89.54 | 15.23 | 97.14 | 16.05 | 84.56 | 7.77 | 238 | 96.49 | 15.23 | 100.70 | 17.16 | 85.59 | 8.87 | 456 | 93.17 | 15.61 | 99.00 | 16.71 | 85.10 | 8.37 |
| 20–39 | 41 | 100.87 | 20.19 | 97.85 | 21.33 | 82.47 | 8.40 | 84 | 100.54 | 15.54 | 95.26 | 13.84 | 83.94 | 6.69 | 125 | 100.65 | 17.18 | 96.11 | 16.63 | 83.46 | 7.30 |
| 40–59 | 224 | 105.85 | 19.32 | 98.63 | 16.16 | 80.69 | 7.71 | 161 | 111.99 | 20.40 | 102.96 | 22.02 | 82.35 | 9.08 | 385 | 108.42 | 19.98 | 100.44 | 18.93 | 81.49 | 8.33 |
| >60 | 173 | 102.33 | 29.52 | 93.82 | 24.28 | 75.63 | 11.63 | 292 | 116.13 | 28.69 | 100.02 | 21.50 | 80.84 | 10.74 | 465 | 110.99 | 29.73 | 97.71 | 22.74 | 78.90 | 11.34 |
| Over a radius of 10 km from industrial complexes | |||||||||||||||||||||
| <9 | - | - | - | - | - | - | - | 11 | 90.82 | 8.82 | 93.91 | 10.01 | 86.65 | 7.62 | 11 | 90.82 | 8.83 | 93.91 | 10.01 | 86.65 | 7.62 |
| 10–19 | 107 | 92.89 | 17.37 | 100.03 | 18.86 | 83.58 | 8.54 | 79 | 97.26 | 15.44 | 101.41 | 13.85 | 87.45 | 7.56 | 183 | 94.71 | 16.69 | 100.60 | 16.94 | 85.18 | 8.35 |
| 20–39 | 29 | 100.40 | 18.89 | 94.54 | 15.31 | 84.63 | 8.36 | 3 | 118.67 | 17.93 | 111.67 | 9.50 | 82.87 | 7.18 | 32 | 102.07 | 19.00 | 97.53 | 17.98 | 83.29 | 7.41 |
| 40–59 | 84 | 112.11 | 23.55 | 104.55 | 18.58 | 81.52 | 6.71 | 32 | 119.13 | 18.27 | 107.81 | 15.26 | 82.24 | 5.28 | 116 | 114.05 | 22.37 | 105.45 | 17.72 | 81.72 | 6.34 |
| >60 | 80 | 117.17 | 29.19 | 104.33 | 24.32 | 79.24 | 9.40 | 54 | 117.00 | 32.07 | 103.26 | 25.08 | 78.63 | 12.16 | 134 | 117.11 | 30.27 | 103.89 | 24.54 | 78.99 | 10.56 |
| Total | |||||||||||||||||||||
| <9 | 18 | 98.50 | 12.01 | 102.72 | 12.76 | 86.59 | 7.97 | 49 | 95.49 | 11.94 | 98.10 | 12.64 | 87.54 | 7.51 | 67 | 96.30 | 11.95 | 99.34 | 12.74 | 87.29 | 7.58 |
| 10–19 | 325 | 90.65 | 16.02 | 98.09 | 17.05 | 84.24 | 8.03 | 314 | 96.68 | 15.27 | 100.87 | 16.40 | 86.04 | 8.59 | 639 | 93.60 | 15.93 | 99.46 | 16.78 | 85.12 | 8.35 |
| 20–39 | 70 | 100.68 | 19.52 | 96.48 | 19.01 | 83.37 | 8.40 | 87 | 101.17 | 15.95 | 95.83 | 14.01 | 83.90 | 6.67 | 157 | 100.95 | 17.58 | 96.12 | 16.37 | 83.66 | 7.47 |
| 40–59 | 308 | 107.56 | 20.71 | 100.25 | 17.03 | 81.06 | 7.45 | 193 | 113.18 | 20.19 | 103.77 | 21.10 | 82.33 | 8.56 | 501 | 109.72 | 20.68 | 101.60 | 18.76 | 81.55 | 7.91 |
| >60 | 253 | 107.02 | 30.16 | 97.14 | 24.74 | 76.77 | 10.11 | 346 | 116.26 | 29.19 | 100.53 | 22.09 | 80.50 | 10.98 | 599 | 112.36 | 29.93 | 99.09 | 23.28 | 78.92 | 11.17 |
| p-value | 0.00 * | 0.24 | 0.00 * | 0.00 * | 0.02 * | 0.00 * | 0.00 * | 0.03 * | 0.00 * | ||||||||||||
| Variable | Total (n = 1963) | ||||
|---|---|---|---|---|---|
| n | Abnormal Pulmonary Functions | Adjusted OR † | 95% CI | ||
| Yes | No | ||||
| Sex | |||||
| Female | 799 | 101 | 698 | Reference | - |
| Male | 1164 | 145 | 1019 | 0.79 | 0.54–1.17 |
| Distance from industrial complexes | |||||
| >10 km | 476 | 59 | 417 | Reference | - |
| ≤5 km | 1487 | 187 | 1300 | 1.24 | 0.71–1.96 |
| Distance from the streets | |||||
| >100 m | 1222 | 128 | 1094 | Reference | - |
| ≤100 m | 332 | 42 | 290 | 1.15 | 0.63–1.84 |
| Alcohol | |||||
| No | 1225 | 167 | 1058 | Reference | - |
| Yes | 536 | 54 | 482 | 1.02 | 0.62–1.61 |
| Smoking | |||||
| No | 1380 | 175 | 1205 | Reference | - |
| Yes | 229 | 29 | 200 | 0.92 | 0.49–1.72 |
| Secondhand smoke | |||||
| No | 728 | 84 | 644 | Reference | - |
| Yes | 792 | 110 | 682 | 1.12 | 0.73–1.71 |
| Pollutant | Gwangyang (n = 974) | Yeosu (n = 989) | Total (n = 1963) | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FEV1 (r2 = 0.65) | FVC (r2 = 0.61) | FEV1/FVC (r2 = 0.15) | FEV1 (r2 = 0.33) | FVC (r2 = 0.34) | FEV1/FVC (r2 = 0.13) | FEV1 (r2 = 0.48) | FVC (r2 = 0.48) | FEV1/FVC (r2 = 0.12) | |||||||||||||||||||
| β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | |
| SO2 | −22.63 | 5.17 | 0.00 * | −28.54 | 6.25 | 0.00 * | −18.27 | 7.07 | 0.03 * | −18.85 | 4.94 | 0.00 * | −20.12 | 5.84 | 0.00 * | −10.82 | 8.32 | 0.47 | −17.43 | 3.44 | 0.00 * | −20.80 | 4.14 | 0.00 * | −12.73 | 6.85 | 0.04 * |
| CO | −0.27 | 0.10 | 0.01 * | −0.35 | 0.12 | 0.02 * | −0.17 | 1.46 | 0.91 | −0.12 | 0.09 | 0.20 | −0.18 | 0.11 | 0.10 | −0.04 | 1.26 | 0.50 | −0.15 | 0.07 | 0.02 * | −0.23 | 0.08 | 0.00 * | −0.08 | 1.07 | 0.48 |
| NO2 | 5.49 | 4.77 | 0.25 | 7.68 | 5.76 | 0.18 | 8.23 | 9.64 | 0.92 | 2.78 | 4.47 | 0.54 | 2.54 | 5.28 | 0.63 | 5.69 | 7.44 | 0.48 | 5.27 | 3.08 | 0.09 | 6.06 | 3.72 | 0.08 | 7.82 | 5.10 | 0.73 |
| O3 | −43.00 | 2.21 | 0.00 * | −46.89 | 2.81 | 0.00 * | −21.19 | 4.04 | 0.00 * | −16.42 | 2.17 | 0.01 * | −19.73 | 2.62 | 0.01 * | −13.49 | 3.68 | 0.02 * | −24.91 | 1.53 | 0.00 * | −24.85 | 2.75 | 0.00 * | −17.87 | 2.54 | 0.04 * |
| PM10 | −0.04 | 0.03 | 0.35 | −0.01 | 0.02 | 0.03 * | −0.02 | 0.03 | 0.48 | 0.01 | 0.02 | 0.61 | 0.01 | 0.02 | 0.62 | 0.01 | 0.03 | 0.70 | 0.02 | 0.01 | 0.17 | 0.03 | 0.01 | 0.16 | −0.01 | 0.02 | 0.96 |
| Pollutant | Within a Radius of 5 km (Exposed) (n = 1487) | Over a Radius of 10 km (Control) (n = 476) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FEV1 (r2 = 0.50) | FVC (r2 = 0.48) | FEV1/FVC (r2 = 0.12) | FEV1 (r2 = 0.51) | FVC (r2 = 0.51) | FEV1/FVC (r2 = 0.11) | |||||||||||||
| β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | |
| SO2 | −18.17 | 4.07 | 0.00 * | −22.53 | 4.93 | 0.00 * | −19.33 | 7.02 | 0.04 * | −16.45 | 6.29 | 0.01 * | −17.48 | 7.47 | 0.02 * | −11.11 | 9.55 | 0.59 |
| CO | −0.19 | 0.08 | 0.01 * | −0.30 | 0.09 | 0.00 * | −0.15 | 1.30 | 0.26 | −0.06 | 0.12 | 0.61 | −0.06 | 0.15 | 0.71 | −0.14 | 0.19 | 0.55 |
| NO2 | 7.25 | 3.55 | 0.04 * | 7.64 | 4.30 | 0.05 * | 7.07 | 6.13 | 0.27 | 2.37 | 6.14 | 0.70 | 0.61 | 7.29 | 0.93 | −1.29 | 9.32 | 0.67 |
| O3 | −17.43 | 1.78 | 0.00 * | −20.57 | 2.16 | 0.00 * | −45.95 | 3.07 | 0.00 * | −20.62 | 2.99 | 0.00 * | −22.56 | 3.55 | 0.00 * | −19.42 | 4.54 | 0.17 |
| PM10 | −0.02 | 0.01 | 0.02 * | −0.01 | 0.01 | 0.02 * | −0.02 | 0.02 | 0.24 | 0.01 | 0.01 | 0.34 | 0.01 | 0.02 | 0.34 | −0.01 | 0.04 | 0.85 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, E.; Lee, S.; Kim, G.-B.; Kim, T.-J.; Kim, H.-W.; Lee, K.; Son, B.-S. Effects of Environmental Air Pollution on Pulmonary Function Level of Residents in Korean Industrial Complexes. Int. J. Environ. Res. Public Health 2018, 15, 834. https://doi.org/10.3390/ijerph15050834
Hong E, Lee S, Kim G-B, Kim T-J, Kim H-W, Lee K, Son B-S. Effects of Environmental Air Pollution on Pulmonary Function Level of Residents in Korean Industrial Complexes. International Journal of Environmental Research and Public Health. 2018; 15(5):834. https://doi.org/10.3390/ijerph15050834
Chicago/Turabian StyleHong, Eunju, Seokwon Lee, Geun-Bae Kim, Tae-Jong Kim, Hyoung-Wook Kim, Kyoungho Lee, and Bu-Soon Son. 2018. "Effects of Environmental Air Pollution on Pulmonary Function Level of Residents in Korean Industrial Complexes" International Journal of Environmental Research and Public Health 15, no. 5: 834. https://doi.org/10.3390/ijerph15050834
APA StyleHong, E., Lee, S., Kim, G. -B., Kim, T. -J., Kim, H. -W., Lee, K., & Son, B. -S. (2018). Effects of Environmental Air Pollution on Pulmonary Function Level of Residents in Korean Industrial Complexes. International Journal of Environmental Research and Public Health, 15(5), 834. https://doi.org/10.3390/ijerph15050834