Differentiating Medicated Patients Suffering from Major Depressive Disorder from Healthy Controls by Spot Urine Measurement of Monoamines and Steroid Hormones

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Healthy Controls
2.2. Measurement of Monoamines and Steroid Hormones in Spot Urine
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Patients and Healthy Controls
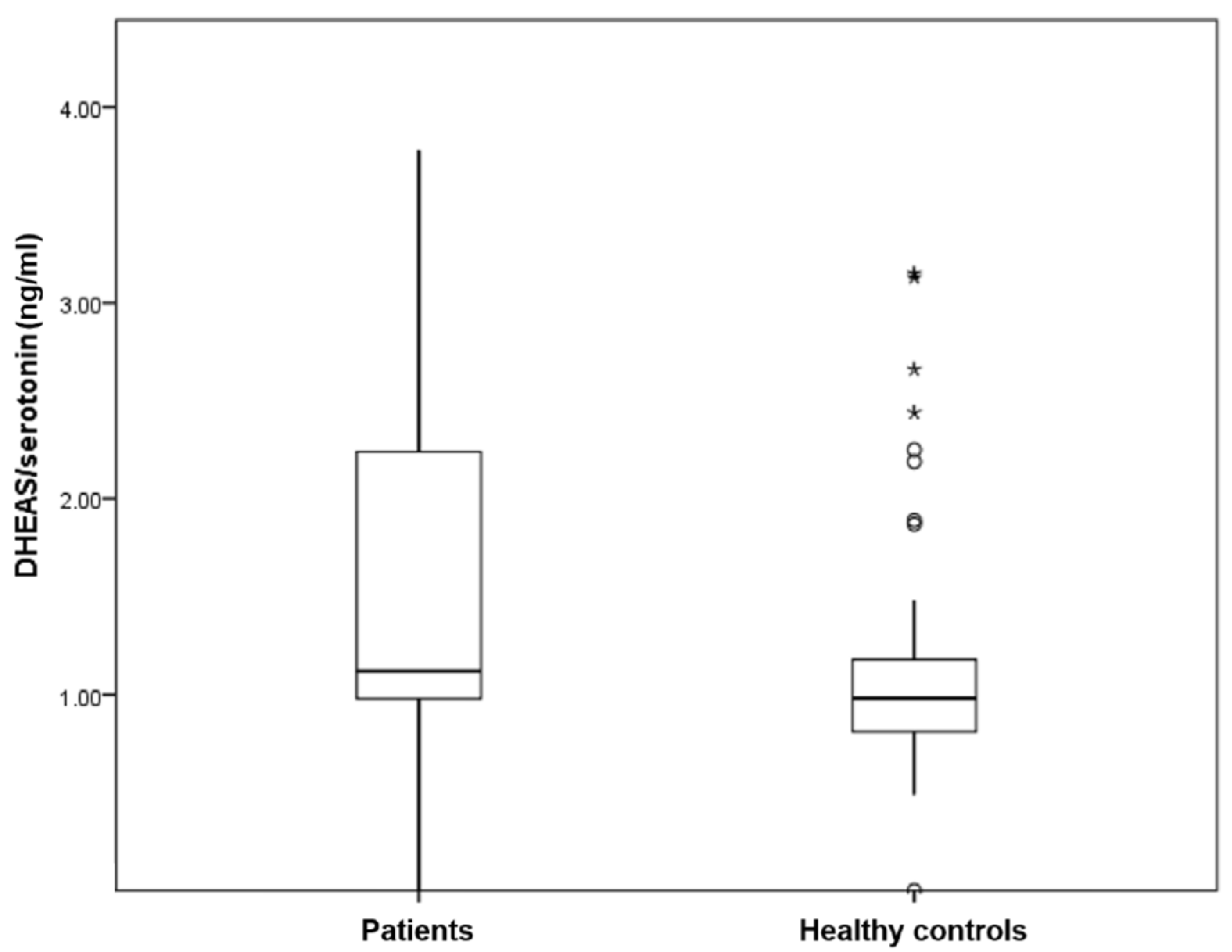
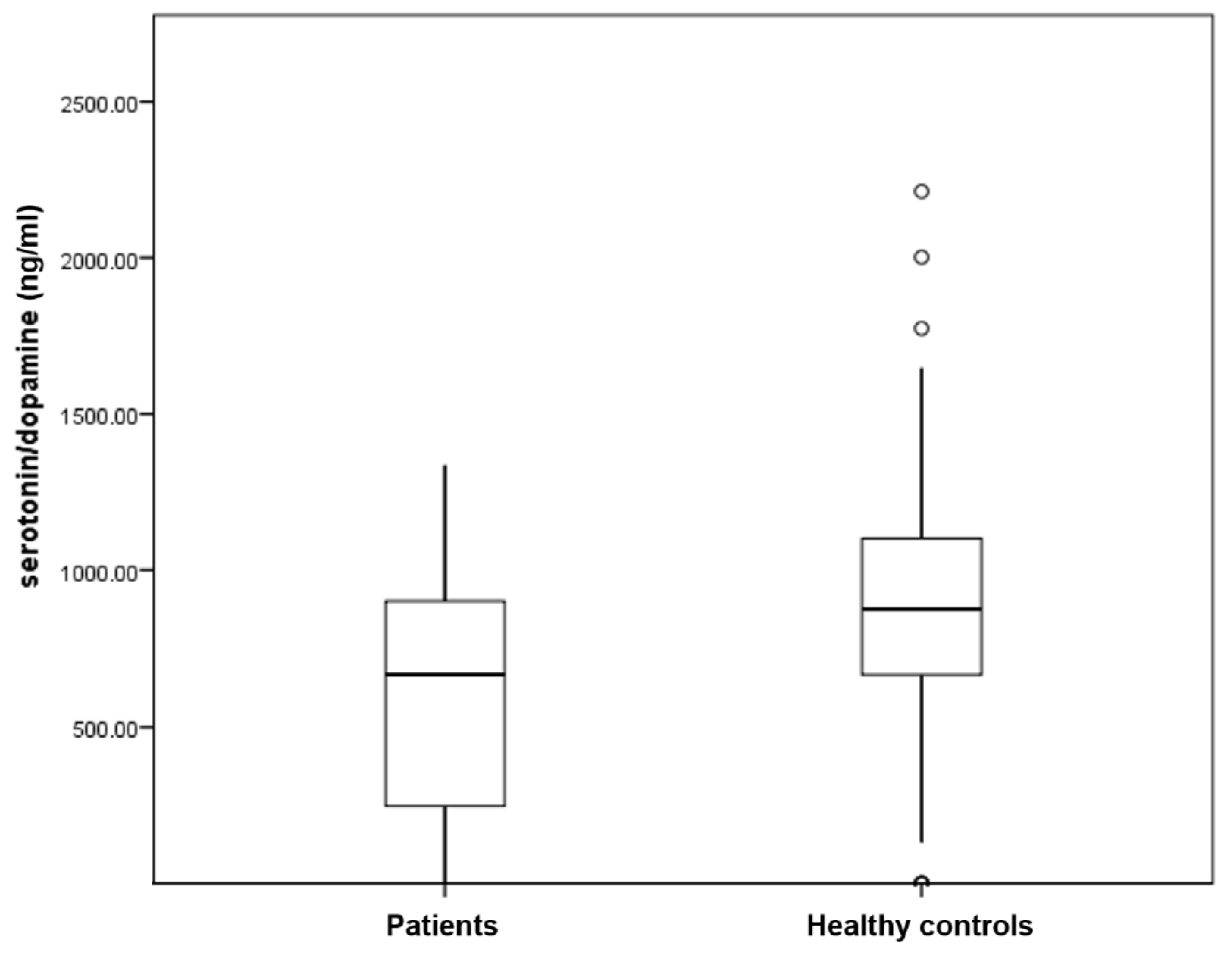
3.2. Levels of Catecholamine and Steroid Hormone in Spot Urine
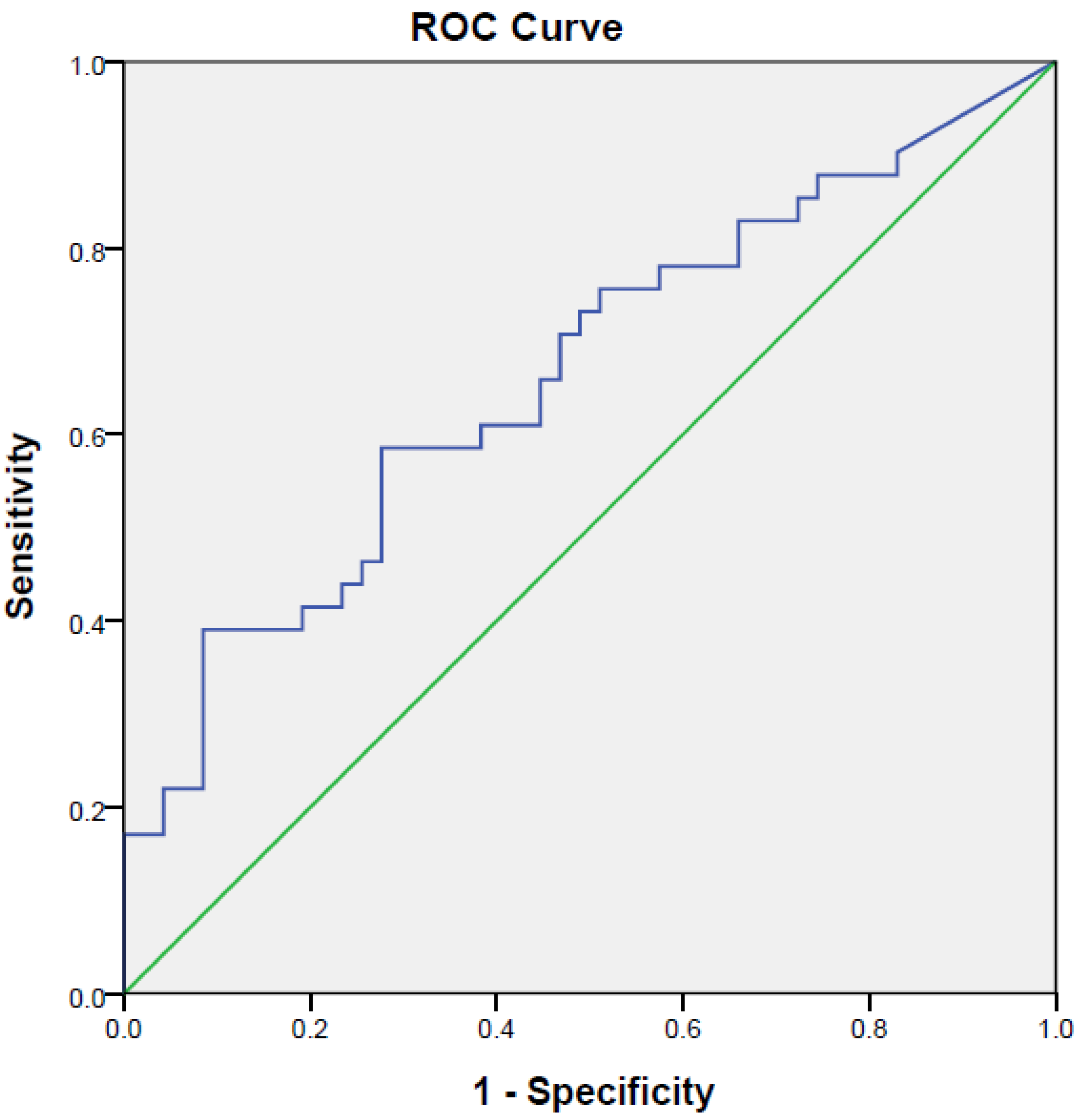
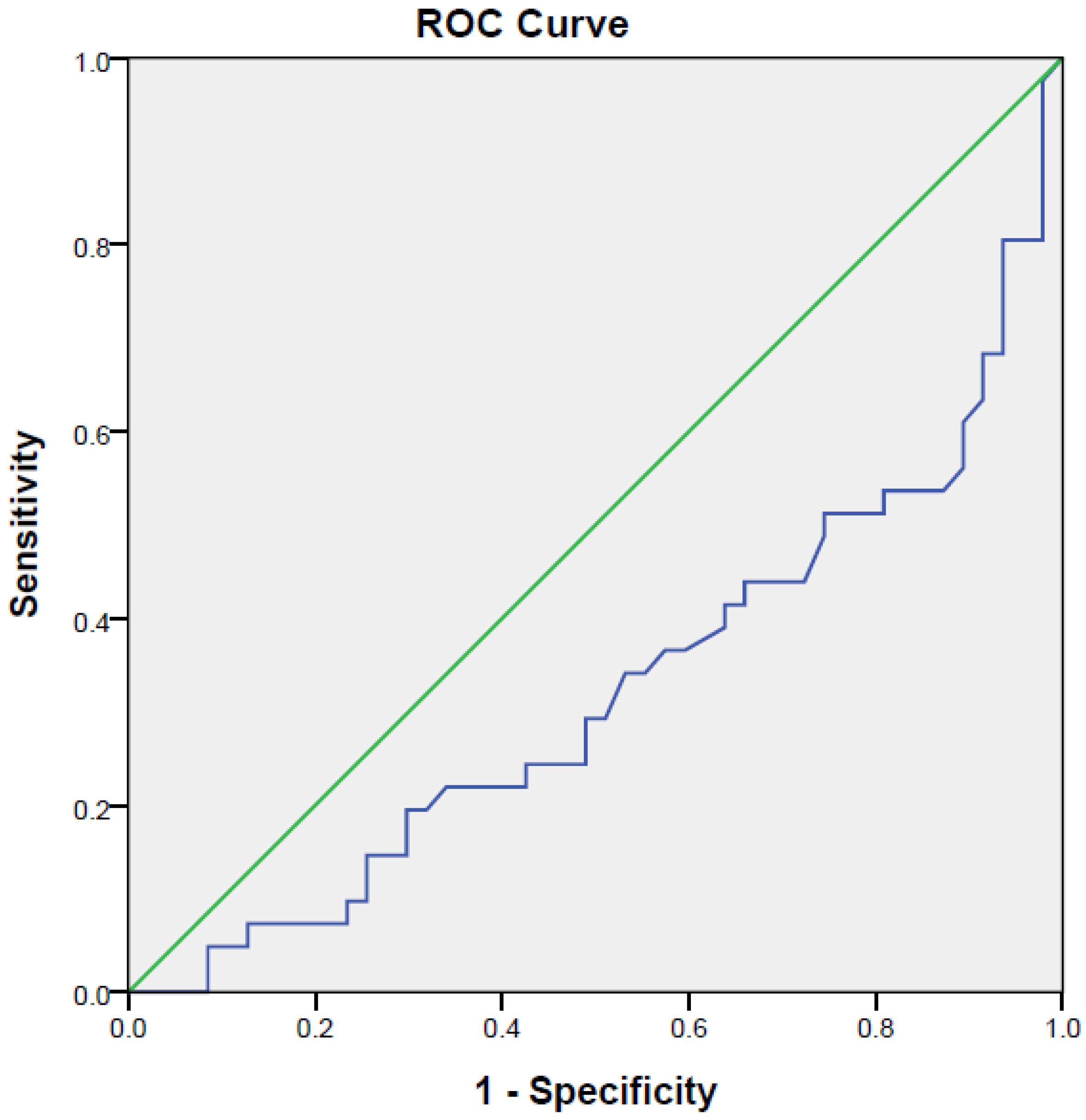
3.3. Discrimination of Medicated Patients Suffering from MDD and Healthy Controls
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Puri, B.; Hall, A.; Ho, R. Revision Notes in Psychiatry; CRC Press: Boca Raton, FL, USA, 2014. [Google Scholar]
- Yeo, S.N.; Zainal, H.; Tang, C.S.; Tong, E.M.; Ho, C.S.; Ho, R.C. Success/failure condition influences attribution of control, negative affect, and shame among patients with depression in Singapore. BMC Psychiatry 2017, 17, 285. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Tang, C.; Liow, C.S.; Ng, W.W.; Ho, C.S.; Ho, R.C. A regressional analysis of maladaptive rumination, illness perception and negative emotional outcomes in Asian patients suffering from depressive disorder. Asian J. Psychiatry 2014, 12, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.H.; Tang, C.; Ng, W.W.; Ho, C.S.; Ho, R.C. Determining the quality of life of depressed patients in Singapore through a multiple mediation framework. Asian J. Psychiatry 2015, 18, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Ho, R.C.; Mak, K.K.; Chua, A.N.; Ho, C.S.; Mak, A. The effect of severity of depressive disorder on economic burden in a university hospital in Singapore. Expert Rev. Pharmacoecon. Outcomes Res. 2013, 13, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Ho, R.C.; Zhang, M.W. Ketamine as a rapid antidepressant: The debate and implications. BJPsych Adv. 2016, 22, 222–233. [Google Scholar] [CrossRef]
- Ho, C.S.; Zhang, M.W.; Ho, R.C. Optical Topography in Psychiatry: A Chip off the Old Block or a New Look beyond the Mind-Brain Frontiers? Front. Psychiatry 2016, 7, 74. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.Y.; Ho, C.S.; Lim, C.R.; Ho, R.C. Functional near-infrared spectroscopy in psychiatry. BJPsych Adv. 2017, 23, 324–330. [Google Scholar] [CrossRef]
- Zheng, P.; Wang, Y.; Chen, L.; Yang, D.; Meng, H.; Zhou, D.; Zhong, J.; Lei, Y.; Melgiri, N.D.; Xie, P. Identification and validation of urinary metabolite biomarkers for major depressive disorder. Mol. Cell. Proteom. 2013, 12, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Chen, X.M.; Liu, R.H. Novel urinary metabolite signature for diagnosing postpartum depression. Neuropsychiatr. Dis. Treat. 2017, 13, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Zhang, X.A. A Novel Urinary Metabolite Signature for Non-invasive Post-stroke Depression Diagnosis. Cell Biochem. Biophys. 2015, 72, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.N.; Choi, Y.H.; Lim, Y.H.; Hong, Y.C. Urinary phthalate metabolites and depression in an elderly population: National Health and Nutrition Examination Survey 2005–2012. Environ. Res. 2016, 145, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.S.; Zhang, M.W.; Mak, A.; Ho, R.C. Metabolic syndrome in psychiatry: Advances in understanding and management. Adv. Psychiatr. Treat. 2014, 20, 101–112. [Google Scholar] [CrossRef]
- Yang, J.L.; Liu, X.; Jiang, H.; Pan, F.; Ho, C.S.; Ho, R.C. The Effects of High-fat-diet Combined with Chronic Unpredictable Mild Stress on Depression-like Behavior and Leptin/LepRb in Male Rats. Sci. Rep. 2016, 6, 35239. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Ho, R.C.; Mak, A. Interleukin (IL)-6, tumour necrosis factor alpha (TNF-alpha) and soluble interleukin-2 receptors (sIL-2R) are elevated in patients with major depressive disorder: A meta-analysis and meta-regression. J. Affect. Disord. 2012, 139, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Whyatt, R.M.; Perzanowski, M.S.; Just, A.C.; Rundle, A.G.; Donohue, K.M.; Calafat, A.M.; Hoepner, L.A.; Perera, F.P.; Miller, R.L. Asthma in inner-city children at 5–11 years of age and prenatal exposure to phthalates: The Columbia Center for Children’s Environmental Health Cohort. Environ. Health Perspect. 2014, 122, 1141–1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, Y.; Van Bever, H.P.; Lim, T.K.; Kuan, W.S.; Goh, D.Y.; Mahadevan, M.; Sim, T.B.; Ho, R.; Larbi, A.; Ng, T.P. Obesity, asthma prevalence and IL-4: Roles of inflammatory cytokines, adiponectin and neuropeptide Y. Pediatr. Allergy Immunol. 2015, 26, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Ho, R.C. An association between neuropeptide Y levels and leukocyte subsets in stress-exacerbated asthmatic mice. Neuropeptides 2016, 57, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Park, H.Y.; Kim, J.H.; Lim, Y.H.; Bae, S.; Hong, Y.C. Influence of genetic polymorphisms on the association between phthalate exposure and pulmonary function in the elderly. Environ. Res. 2013, 122, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.W.; Ho, R.C.; Cheung, M.W.; Fu, E.; Mak, A. Prevalence of depressive symptoms in patients with chronic obstructive pulmonary disease: A systematic review, meta-analysis and meta-regression. Gen. Hosp. Psychiatry 2011, 33, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Lind, P.M.; Roos, V.; Rönn, M.; Johansson, L.; Ahlström, H.; Kullberg, J.; Lind, L. Serum concentrations of phthalate metabolites are related to abdominal fat distribution two years later in elderly women. Environ. Health 2012, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Quek, Y.H.; Tam, W.W.S.; Zhang, M.W.B.; Ho, R.C.M. Exploring the association between childhood and adolescent obesity and depression: A meta-analysis. Obes. Rev. 2017, 18, 742–754. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.P.; Schmidt, D.; Stein, C.M.; Morrow, J.D.; Salomon, R.M. Increased oxidative stress in patients with depression and its relationship to treatment. Psychiatry Res. 2013, 206, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.J.; Zhou, C.J.; Liu, Z.; Fu, Y.Y.; Zheng, P.; Yang, D.Y.; Li, Q.; Mu, J.; Wei, Y.D.; Zhou, J.J.; et al. Divergent Urinary Metabolic Phenotypes between Major Depressive Disorder and Bipolar Disorder Identified by a Combined GC-MS and NMR Spectroscopic Metabonomic Approach. J. Proteome Res. 2015, 14, 3382–3389. [Google Scholar] [CrossRef] [PubMed]
- Rosado, B.; Garcia-Belenguer, S.; Leon, M.; Chacon, G.; Villegas, A.; Palacio, J. Effect of fluoxetine on blood concentrations of serotonin, cortisol and dehydroepiandrosterone in canine aggression. J. Vet. Pharmacol. Ther. 2011, 34, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Oei, T.P.; Dingle, G.A.; McCarthy, M. Urinary catecholamine levels and response to group cognitive behaviour therapy in depression. Behav. Cognit.Psychother. 2010, 38, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Nichkova, M.I.; Huisman, H.; Wynveen, P.M.; Marc, D.T.; Olson, K.L.; Kellermann, G.H. Evaluation of a novel ELISA for serotonin: Urinary serotonin as a potential biomarker for depression. Anal. Bioanal. Chem. 2012, 402, 1593–1600. [Google Scholar] [CrossRef] [PubMed]
- Komiyama, Y.; Kurosaki, M.; Nakanishi, H.; Takahashi, Y.; Itakura, J.; Yasui, Y.; Tamaki, N.; Takada, H.; Higuchi, M.; Gotou, T.; et al. Prediction of diuretic response to tolvaptan by a simple, readily available spot urine Na/K ratio. PLoS ONE 2017, 12, e0174649. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, S.; Lovibond, P. Manual for the depression anxiety stress scales. Sydney: Psychology Foundation; 1995. Hum. Reprod. 1999, 14, 3126–3132. [Google Scholar]
- Grossman, F.; Potter, W.Z. Catecholamines in depression: A cumulative study of urinary norepinephrine and its major metabolites in unipolar and bipolar depressed patients versus healthy volunteers at the NIMH. Psychiatry Res. 1999, 87, 21–27. [Google Scholar] [CrossRef]
- Herr, N.; Bode, C.; Duerschmied, C. The effects of Serotonin in immune cells. Front. Cardiovasc. Med. 2017, 4, 48. [Google Scholar] [CrossRef] [PubMed]
- Ritsner, M.; Gibel, A.; Maayan, R.; Ratner, Y.; Ram, E.; Biadsy, H.; Modai, I.; Weizman, A. Cortisol/dehydroepiandrosterone ratio and responses to antipsychotic treatment in schizophrenia. Neuropsychopharmacology 2005, 30, 1913–1922. [Google Scholar] [CrossRef] [PubMed]
- Takizawa, R.; Fukuda, M.; Kawasaki, S.; Kasai, K.; Mimura, M.; Pu, S.; Noda, T.; Niwa, S.I.; Okazaki, Y.; Joint Project for Psychiatric Application of Near-Infrared Spectroscopy (JPSY-NIRS) Group. Neuroimaging-aided differential diagnosis of the depressive state. NeuroImage 2014, 85 Pt 1, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Ho, R.C.M.; Cheung, M.W.L.; Fu, E.; Win, H.H.; Zaw, M.H.; Ng, A.; Mak, A. Is high homocysteine level a risk factor for cognitive decline in elderly? A systematic review, meta-analysis, and meta-regression. Am. J. Geriatr. Psychiatry. 2011, 19, 607–617. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medicated Patients with MDD (n = 47) | Healthy Controls (n = 41) | Statistical Test | p-Value | |
|---|---|---|---|---|
| Age | t-test | 0.104 | ||
| Mean ± SD | 40.65 ± 10.94 | 44.6 ± 11.28 | ||
| Median (min–max) | 42.5 (21–61) | 47 (23–62) | ||
| Gender | Fisher’s exact | 0.276 | ||
| Male | 15 (31.9%) | 18 (43.9%) | ||
| Female | 32 (68.1%) | 23 (56.1%) | ||
| Ethnicity | Chi square | 0.453 | ||
| Chinese | 36 (76.6%) | 34 (82.9%) | ||
| Malay | 3 (6.4%) | 1 (2.4%) | ||
| Indian | 6 (12.8%) | 2 (4.9%) | ||
| Eurasian | 1 (2.1%) | 1 (2.4%) | ||
| Others | 1 (2.1%) | 3 (7.3%) | ||
| Depression score | Mann–Whitney U | <0.001 ** | ||
| Mean ± SD | 19.29 ± 12.79 | 2.29 ± 3.24 | ||
| Median (min–max) | 18 (0–42) | 0 (0–12) | ||
| Anxiety score | Mann–Whitney U | <0.001 ** | ||
| Mean ± SD | 18.86 ± 10.03 | 2.93 ± 2.69 | ||
| Median (min–max) | 20 (0–42) | 2 (0–8) | ||
| Stress score | Mann–Whitney U | <0.001 ** | ||
| Mean ± SD | 21.26 ± 10.38 | 5.29 ± 4.57 | ||
| Median (min–max) | 21 (0–42) | 4.67 (0–18) | ||
| Depression | Chi square | <0.001 ** | ||
| Normal (0–9) | 14 (29.8%) | 39 (95.1%) | ||
| Mild (10–13) | 5 (10.6%) | 2 (4.9%) | ||
| Moderate (14–20) | 7 (14.9%) | 0 | ||
| Severe (21–27) | 5 (10.6%) | 0 | ||
| Extremely severe (≥28) | 16 (34.0%) | 0 | ||
| Anxiety | Chi square | <0.001 ** | ||
| Normal (0–7) | 6 (12.8%) | 36 (87.8%) | ||
| Mild (8–9) | 4 (8.5%) | 5 (12.2%) | ||
| Moderate (10–14) | 7 (14.9%) | 0 | ||
| Severe (15–19) | 6 (12.8%) | 0 | ||
| Extremely severe (≥20) | 24(51.1%) | 0 | ||
| Stress | Chi square | <0.001 | ||
| Normal (0–14) | 16 (34.0%) | 40 (97.6%) | ||
| Mild (15–18) | 5 (10.6%) | 1 (2.4%) | ||
| Moderate (19–25) | 10 (21.3%) | 0 | ||
| Severe (26–33) | 9 (19.1%) | 0 | ||
| Extremely severe (≥34) | 7 (14.9%) | 0 |
| Normal | Mild | Moderate | Severe | Extremely Severe | p-Value | |
|---|---|---|---|---|---|---|
| Depression | ||||||
| n | 14 | 5 | 7 | 5 | 16 | |
| Cortisol | 152.39 (50.58–409.35) | 114.18 (67.91–298.55) | 127.63 (0–354.45) | 63.84 (50.88–224.60) | 137.49 (0–331.20) | 0.606 |
| DHEAS | 401.62 (90.89–764.85) | 154.50 (73.09–338.3) | 303.20 (117.63–599.03) | 98.21 (63.67–565.93) | 229.14 (82.95–735.40) | 0.259 |
| Serotonin | 194.24 (70.58–495.73) | 133.15 (75.58–321.35) | 200.20 (0–387.98) | 89.18 (66.60–229.90) | 174.58 (66.83–350.25) | 0.409 |
| Dopamine | 263.22 (0–494.58) | 204.95 (0–447.05) | 272.45 (0–478.35) | 461.13 (0–1723.25) | 193.00 (0–626.93) | 0.422 |
| Anxiety | ||||||
| n | 6 | 4 | 7 | 6 | 24 | |
| Cortisol | 151.52 (84.80–221.88) | 138.53 (108–182.65) | 162.53 (73.22–298.55) | 188.90 (63.84–409.35) | 104.37 (0–331.20) | 0.289 |
| DHEAS | 393.63 (147.18–764.85) | 410.92 (110.41–588.80) | 331.58 (117.63–625.10) | 318.57 (89.81–593.18) | 205.90 (63.67–599.03) | 0.280 |
| Serotonin | 171.63 (132.77–350.25) | 186.48 (133.15–243.00) | 237.40 (108.03–379.78) | 200.29 (89.18–495.73) | 123.23 (0–315.95) | 0.205 |
| Dopamine | 278.07 (186.65–388.53) | 349.165 (204.95–461.13) | 242.78 (0–380.73) | 486.47 (140.10–1723.25) | 184.80 (0–626.93) | 0.093 |
| Stress | ||||||
| n | 16 | 5 | 10 | 9 | 7 | |
| Cortisol | 162.71 (50.58–409.35) | 106.35 (63.84–354.45) | 148.90 (0–298.55) | 99.29 (50.88–142.15) | 97.67 (0–331.20) | 0.119 |
| DHEAS | 293.74 (90.89–764.85) | 154.50 (73.09–333.93) | 408.22 (117.63–599.03) | 132.88 (63.67–590.90) | 164.55 (82.95–292.18) | 0.030 * |
| Serotonin | 230.34 (70.58–495.73) | 123.73 (75.58–387.98) | 177.28 (0–321.35) | 121.70 (66.66–200.20) | 112.98 (66.83–315.95) | 0.106 |
| Dopamine | 280.03 (0–626.93) | 478.35 (0–1723.25) | 235.13 (0–461.13) | 182.90 (0–393.15) | 191.75 (129.30–497.70) | 0.585 |
| Medicated Patients with MDD (n = 47) | Healthy Controls (n = 41) | Statistical Test | p-Value | |
|---|---|---|---|---|
| Cortisol (ng/mL) | Mann–Whitney U | 0.533 | ||
| Mean ± SD | 148.56 ± 87.50 | 172.47 ± 117.90 | ||
| Median (min–max) | 142.15 (0–409.35) | 128.45 (0–604.50) | ||
| DHEAS (ng/mL) | Mann–Whitney U | 0.607 | ||
| Mean ± SD | 298.32 ± 203.63 | 247.05 ± 149.86 | ||
| Median (min–max) | 244.00 (63.67–764.85) | 229.00 (0–757.63) | ||
| Serotonin (ng/mL) | Mann–Whitney U | 0.281 | ||
| Mean ± SD | 187.10 ± 102.48 | 236.83 ± 210.55 | ||
| Median (min–max) | 170.68 (0–495.73) | 168.55 (0–1315.25) | ||
| Dopamine (pg/mL) | Mann–Whitney U | 0.682 | ||
| Mean ± SD | 277.70 ± 271.97 | 280.19 ± 251.81 | ||
| Median (min–max) | 242.98 (0–1723.25) | 216.10 (0–1348.83) | ||
| Cortisol/DHEAS | Mann–Whitney U | 0.252 | ||
| Mean ± SD | 0.603 ± 0.310 | 0.700 ± 0.282 | ||
| Median (min–max) | 0.670 (0–1.18) | 0.620 (0–1.32) | ||
| Cortisol/Serotonin | Mann–Whitney U | 0.116 | ||
| Mean ± SD | 0.771 ± 0.200 | 0.876 ± 0.639 | ||
| Median (min–max) | 0.7800 (0–1.10) | 0.610 (0–2.25) | ||
| Cortisol/Dopamine | Mann–Whitney U | 0.171 | ||
| Mean ± SD | 463.95 ± 315.04 | 729.86 ± 646.77 | ||
| Median (min–max) | 492.63 (0–1084.22) | 575.01 (0–3126.00) | ||
| DHEAS/Serotonin | Mann–Whitney U | 0.004 * | ||
| Mean ± SD | 1.56 ± 0.864 | 1.19 ± 0.702 | ||
| Median (min–max) | 1.12 (0–3.78) | 0.980 (0–3.15) | ||
| DHEAS/Dopamine | Mann–Whitney U | 0.363 | ||
| Mean ± SD | 972.71 ± 903.73 | 1047.86 ± 806.38 | ||
| Median (min–max) | 709.99 (0–4057.54) | 885.03 (0–3986.73) | ||
| Serotonin/Dopamine | Mann–Whitney U | 0.008 * | ||
| Mean ± SD | 599.71 ± 394.56 | 888.60 ± 528.75 | ||
| Median (min–max) | 665.39 (0–1335.20) | 875.89 (0–2212.59) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wijaya, C.S.; Lee, J.J.Z.; Husain, S.F.; Ho, C.S.H.; McIntyre, R.S.; Tam, W.W.; Ho, R.C.M. Differentiating Medicated Patients Suffering from Major Depressive Disorder from Healthy Controls by Spot Urine Measurement of Monoamines and Steroid Hormones. Int. J. Environ. Res. Public Health 2018, 15, 865. https://doi.org/10.3390/ijerph15050865
Wijaya CS, Lee JJZ, Husain SF, Ho CSH, McIntyre RS, Tam WW, Ho RCM. Differentiating Medicated Patients Suffering from Major Depressive Disorder from Healthy Controls by Spot Urine Measurement of Monoamines and Steroid Hormones. International Journal of Environmental Research and Public Health. 2018; 15(5):865. https://doi.org/10.3390/ijerph15050865
Chicago/Turabian StyleWijaya, Chandra S., Jovia J. Z. Lee, Syeda F. Husain, Cyrus S. H. Ho, Roger S. McIntyre, Wilson W. Tam, and Roger C. M. Ho. 2018. "Differentiating Medicated Patients Suffering from Major Depressive Disorder from Healthy Controls by Spot Urine Measurement of Monoamines and Steroid Hormones" International Journal of Environmental Research and Public Health 15, no. 5: 865. https://doi.org/10.3390/ijerph15050865
APA StyleWijaya, C. S., Lee, J. J. Z., Husain, S. F., Ho, C. S. H., McIntyre, R. S., Tam, W. W., & Ho, R. C. M. (2018). Differentiating Medicated Patients Suffering from Major Depressive Disorder from Healthy Controls by Spot Urine Measurement of Monoamines and Steroid Hormones. International Journal of Environmental Research and Public Health, 15(5), 865. https://doi.org/10.3390/ijerph15050865