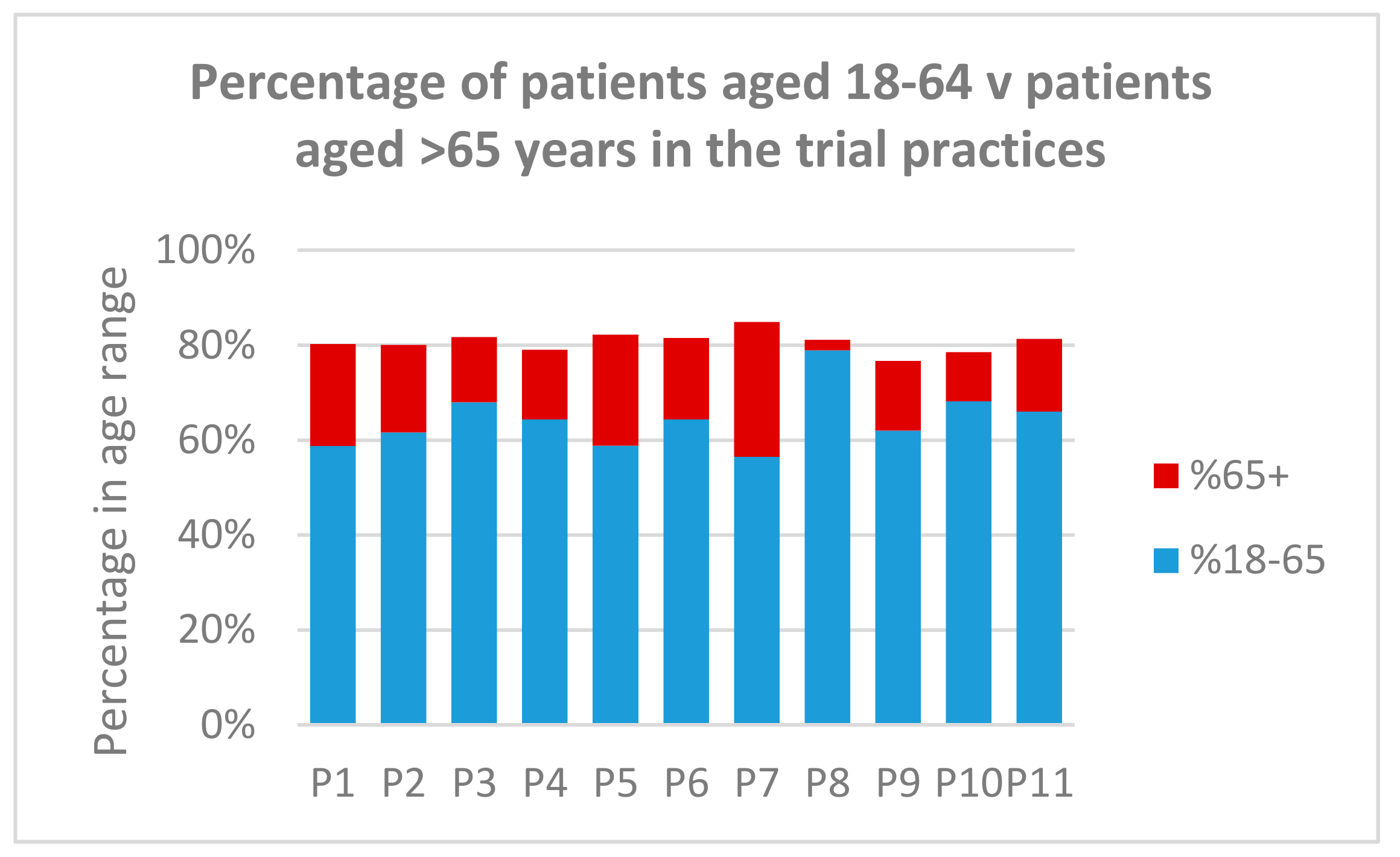
Eleven GP practices across four Scottish NHS boards participated in the evaluation. GP practices were spread across a mix of urban/rural areas. One urban practice served a predominantly younger age group (50.5% under 25) and one rural practice had a slightly older age profile (28.1% aged 65+), while most had a reasonably evenly spread age distribution. Two practices had a high proportion of registered patients residing in the most deprived (bottom 15%) areas of Scotland, as defined by their Scottish Index of Multiple Deprivation (SIMD) codes [
22]. Semi-structured interviews (
n = 44) and a focus group (1 group of 4 staff) were used to collect qualitative data, along with analysis of free-text comments from patient surveys (
n = 291, 6.5% response rate). The complement and number of staff at each practice are detailed in
Table 1 below.
3.2. Patient Opinion and Surgery Staff’s Perceived Patient Opinion of eConsult
Patient surveys were complete by 6.5% of eConsult users. Patient survey data indicated strong satisfaction with eConsult (91.4%), with 91.5% of respondents likely to recommend eConsult to others. Patient survey free text comments were combined with the data arising from the GP staff interviews and using a thematic framework approach the following key themes emerged from the data:
• Flexibility around eConsult use
There was consensus around the flexibility gained from eConsult use, with patients greatly appreciating how the service could fit around them and their lifestyle.
“As someone who works 9–5 it is very convenient service. It is trustworthy and reliable which makes it even better.”
(Patient)
“Sometimes you see it through the night, like, when they’ve finished work, seven o’clock or eight o’clock at night you can see the times, we get them the next morning so when they finish their work that’s when they’re doing the eConsults.”
(P6_Admin)
“…sometimes you can be on the phone twenty plus minutes waiting to get through on the triage line because it is so busy, so it certainly saves a lot of people some time, especially people who are at work who maybe can’t necessarily do a phone call but can quickly jump on the internet and submit an eConsult online.”
(P4_PM)
• Flexibility around how to communicate with GP
Patients and GP staff commented on the benefits of providing individuals with different means of communicating with their GP. This flexibility was felt to ensure that patients felt they had a means of communicating in a way that suited them and they were comfortable with:
“Don’t feel rushed or that I am bothering a GP with maybe trivia. Able to get the point across especially if one can tend to be ‘long-winded’”
(Patient)
“It was to do with depression or something, the clinician felt that the eConsult had actually helped because they didn’t feel that the patient would’ve come in for a face to face consultation…”
(P7_Admin)
“… is you know, how d’you book your holiday and how d’you do your shopping, and then it shows you a picture of a GP surgery in the early twentieth century and a GP surgery at the start of the 21st century and it’s the same, it’s just a pile of folk sitting in seats waiting to be seen by the doctor and that’s true. So I get the fact that this is another way of consulting”
(P9_GP)
“People maybe prefer that interaction with a human being…and people may have difficulty in describing what’s wrong with them, you know, putting that down on paper when perhaps it’s easier for them to verbalise it”
(P7_Admin)
• Issues concerning when eConsult is appropriate to use
There were some concerns raised around when eConsult should be used and when other means of communication were more appropriate. It was felt that given the length of time taken to enter the required details for an eConsult, more clarity should be provided as to whether the eConsult was appropriate to complete for the patient’s current need.
“For some people they might just think ‘four pages cause I’ve got hay fever, it’ll be easier, I’ll just go and get an appointment at the doctor’”
(P2_PM)
“Using the system for the first time, found it a bit frustrating repeating answers to some of the questions.”
(Patient)
However, such comments were balanced out by patients who felt the service suited their needs and sat well with existing services:
“The response was very quick, the advice I was given was what I was looking for and although I felt I didn’t need a face to face appointment, I had one as requested by the doctor. It is a good service to have especially if you feel you don’t want to waste time taking a valuable appointment when it may not be necessary to see someone face to face”
(Patient)
3.3. Impact of eConsult on GP Surgery and Staff
The data arising from the semi-structured interviews and focus group were coded and analysed. The following themes around the impact of eConsult on the surgery and its staff were identified:
• Clinical decision making
GPs interviewed were very confident in patients using eConsult and did not feel that its use posed any risk to patients.
“Yeah we had a look at it clinically before we sort of went into it really and looked at a few, we did the test site so you could look at that, so yeah it seemed quite sensible and appropriate red flags and things like that. So we haven’t any particular clinical concerns about it.”
(P5_GP)
In addition, they felt it complemented the existing services offered, and in some cases, enhanced the face-to-face consultation through provision of information prior to meeting with the patient.
“There’s a definite benefit to seeing information all in one go rather than hearing it on a phone call of course you’re trying to remember what people are saying and you’re taking notes at the same time and you’re trying to think what you’re going to ask them and all that, and that can be a bit confusing.”
(P1_GP1)
“There was one who had a works medical examination and something wasn’t quite right with some of the blood tests that they did and so he sent an eConsult to say ‘they told me this, can you give me some advice on it?’ and the advice was ‘obviously that gives us a bit of a head start, I’ll write you a form to get some other bloods done just to further investigate that and then we can discuss the results at a later date’ so that helped the process.”
(P6_GP)
• Issues with fitting eConsults into existing practice processes
Each practice adopted slightly different ways of embedding eConsults into daily practice, some more successfully than others. As the number of eConsults each practice received per week was relatively low, there were concerns raised around eConsultations overlooked, or not being dealt with in a time-appropriate manner.
“the one that was particularly unfavourable for us was one who was distressed that we didn’t get back in the time span and we didn’t give them what they wanted etc., however it was one of those that didn’t pick up the phone and we had emailed them, but they hadn’t got back to us sort of thing”
(P8_PM)
“like one today, like a UTI, one of the doctors says ‘it’s a UTI, needs prescription’ but because, like, from a Friday morning we don’t have to reply until end of Monday but she’ll need medication today, you know what I mean, so if we didn’t hurry things through, like, we normally say ‘oh an eConsult’s come, we better deal with it now’, if we did just follow the timescale she’d be all weekend without a prescription.”
(P1_Admin)
“I was jumping from one thing to the next that I could be just about ready to go home and think ‘oh my goodness there was three eConsults today and I’ve not emailed them back’, so I didn’t like that, maybe I’m just a bit forgetful but I just felt that it wasn’t safe.”
(P9_GP)
At the current low volume in most practices, there had been little need to consider how to fully integrate eConsults into current processes and this had led in some cases to a perception of eConsults creating extra work. However, this was counterbalanced by the recognition that an eConsult would have been replaced by an alternative type of contact, with the same outcome. Perceptions of whether eConsult added or reduced the administrative workload were often closely related to the systems in place for dealing with submissions. Where these differed little from normal processes for booking appointments or dealing with other clinical processes, the potential for reducing the volume and length of telephone calls was clearly recognised.
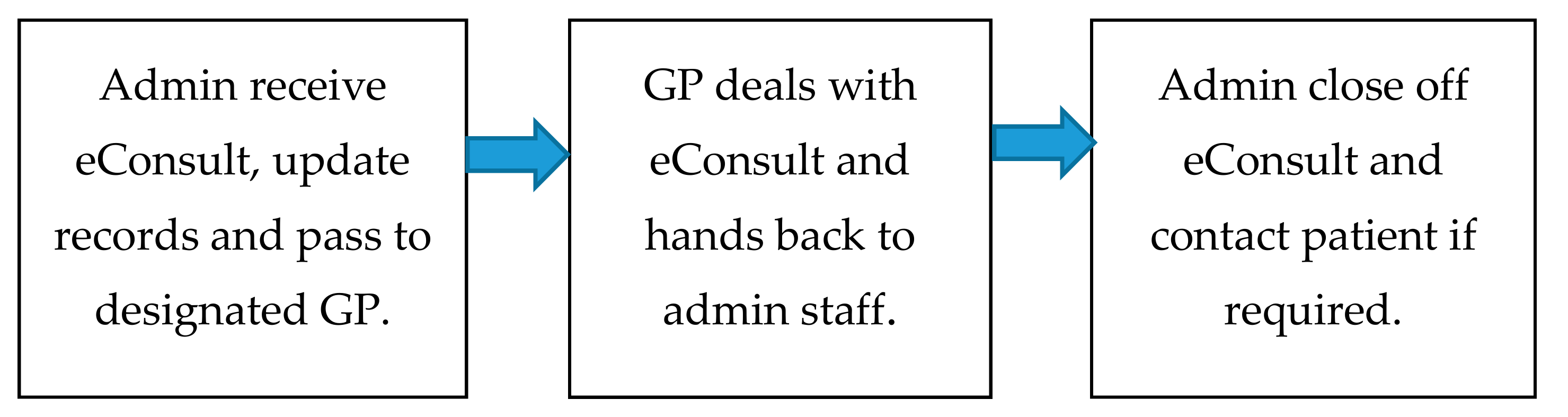
One of the most significant impacts on the administrative workload in the implementation of eConsult is contacting patients to inform them of the outcome of the consultation, in particular to ask them to arrange an appointment. Most practices appeared to make at least three attempts to phone the patient, frequently reporting that contact could not be made. Some expressed a concern that patients would not respond to a withheld number, despite the notification on eConsult that calls may be made on such a number. This differed from processes in place to manage telephone consultations, where patients could be given a close estimate of the time they would be called and expressly informed that it would be from an unavailable number. While some practices had evolved methods to facilitate email contact, there remained a degree of concern about data security, particularly around shared mobile phones and email addresses. As a result, little more than basic information was transmitted.
Concerns were also expressed around integration of eConsults into the appointment system, and whether they may impact on the availability of urgent appointments for other patients. This was often perceived as “skipping the queue”, an impression that was reinforced by some of the eConsult marketing material.
3.4. Time Implications Associated with eConsult
A variation in processes between practices, and the way in which eConsults were handled resulted in significant variation regarding time spent on eConsults by different staff. In addition, there was further variability in assessment of the time spent on an eConsult in comparison to taking a phone call. Consensus was that a straightforward phone call simply requesting an appointment could be handled quickly and in less time than processing an eConsult. There was recognition, however, that where receptionists needed to assess whether an urgent or routine appointment was required, phone calls could take more time than an eConsult.
Similarly, there was no fixed pattern in terms of time impacts for GPs. Most practices operate on the basis of 10-min face-to-face appointments and five minutes for telephone consultations where these are offered. Where eConsults were slotted into appointment times, they generally replaced a five-minute telephone consultation. One of the practices with a relatively high volume of eConsults had calculated that each eConsult took approximately 2.5 min to assess and thus, two eConsults could be fitted into the time allocated for telephone consultations, thus potentially offering a significant time-saving.
Estimates were made for the time required for administrative staff to complete their normal booking and eConsult tasks (see
Table 2). Time estimates were also made for GP eConsult processing times (see
Table 2). These estimates were based on times provided in the interviews. The main variation in eConsult processing timings was due to the amount of patients’ notes consultations required. Estimates have been made based on half of eConsults requiring detailed use of patients’ notes and half requiring minimal use of notes.
Timings for administrative and GP time were estimated for a range of types of eConsult (see
Table 3). These were weighted by the likelihood of that type of eConsult. The weights were based on eConsult data analysis provided by practice P2 which indicated that 43% of eConsults resulted in a further appointment (GP consultation; GP phone consultation or an appointment with a nurse/ANP), 27% of eConsults were administrative, and the remaining eConsults either required a prescription or no further action from the GP. The data provided by Practice 2 did not give precise percentages for type of appointment, administrative task, etc., but these were estimated from information provided in the interviews. The resulting timings are shown in the bottom row of
Table 3.
eConsult submissions can either result in a GP appointment, replace a GP appointment or be the type of query that would be dealt with by administrative staff (e.g., a change of details). The pilots in England and Scotland have not collected sufficiently detailed information for accurate estimates of these types of queries. However, the pilot in England estimated that one eConsult would save 0.6 of a conventional GP appointment. This was based on 40% of eConsults generating a further face-to-face appointment with the GP [
25].
The current evaluation found that practice in Scotland appears to be different. The categories of eConsult which would have previously required a GP appointment are: fit note; GP no action (e.g., follow-up); GP prescription; other appointment e.g., bloods; and GP phone back. These are estimated to account for 73% of the eConsults submitted. In addition, some patients who submitted eConsults would not have sought help if eConsult had not been available. This is estimated to be up to 8% of patients surveyed in England [
25]. Hence, it can be assumed that between 67% and 73% (67% = 73% × 92%) of conventional appointments could be saved by using eConsult.
3.5. Cost/Effectiveness of eConsult
eConsult was not perceived as adding to existing surgery costs, as marketing and implementation costs were covered by the pilot programme. However, at the current levels of submissions, there was a general consensus that eConsult did not offer cost savings, as it was not possible to assess whether it was having any beneficial impact on reducing the number of face-to-face appointments or other services. As such, there would be little economic impetus to adopt the service in the short term.
“at the moment it’s a service that a small number of patients are using and it’s an avenue for them and it’s not huge numbers, it’s picking up but it’s maybe one a day or two a day or something, you know, so for us it’s not saving us much time at the moment, you know, so there’d be no... in us investing in it, we wouldn’t get much back for it. It’s more like a... as things in time it might become more useful and more of an added bonus but right now it’d be hard to think how we would, how we could justify paying for it when it’s not giving us much back.”
(P1_GP2)
A cost analysis was conducted to address potential savings associated with eConsult use. Costs of £95.08 per hour for GP time and £17.82 per hour for administrator time have been used in this evaluation. A detailed derivation of these costs is provided in
Appendix B. Using these costs and the eConsult time estimates presented in
Table 3, it is possible to calculate the total cost savings per eConsult submitted.
Table 4 shows the cost savings, assuming different percentage savings of GP appointments per eConsult submitted.
It has been estimated that an eConsult will save somewhere between 0.6 and 0.74 of a GP appointment. This figure was established from data collected in this trial and is similar to the data collected in the English pilot [
11]. As an eConsult takes more administrative time than a traditional appointment, the cost saving may be negative (Column 2,
Table 4). However, as the GP time for dealing with an eConsult is on average less than that for a traditional appointment, there will be a GP cost saving per eConsult submitted (Column 3,
Table 4). As the GP cost saving is greater than the additional administrative cost, there will be a net cost saving per eConsult submitted (Column 4,
Table 4). This cost saving has then been compared to the annual charge per patient likely to be charged (by the Hurley Group [
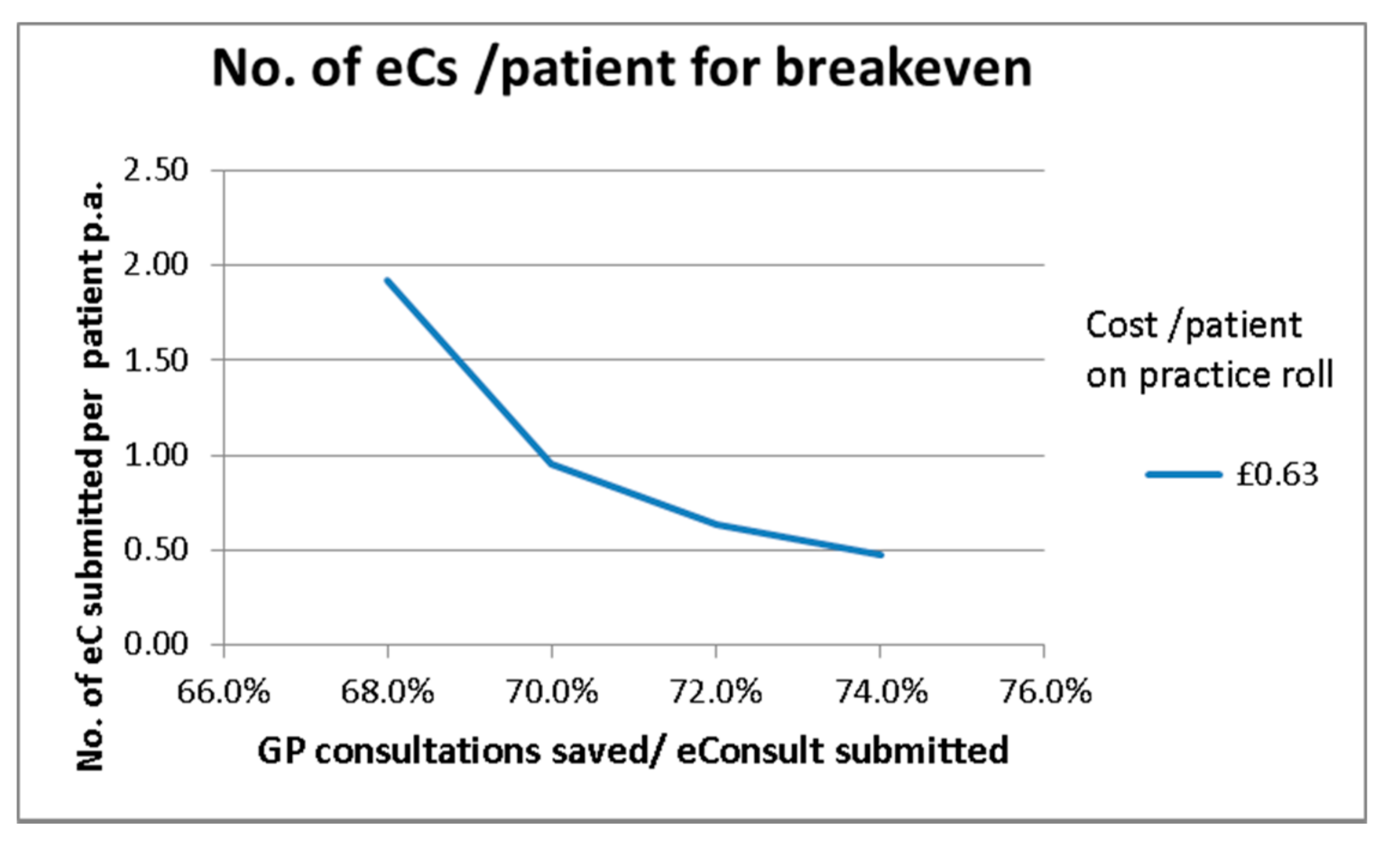
12]) for using the eConsult service. Hence, the number of eConsults submitted per patient that would be required to generate sufficient savings to cover the annual eConsult charge per patient can be calculated; this is shown in
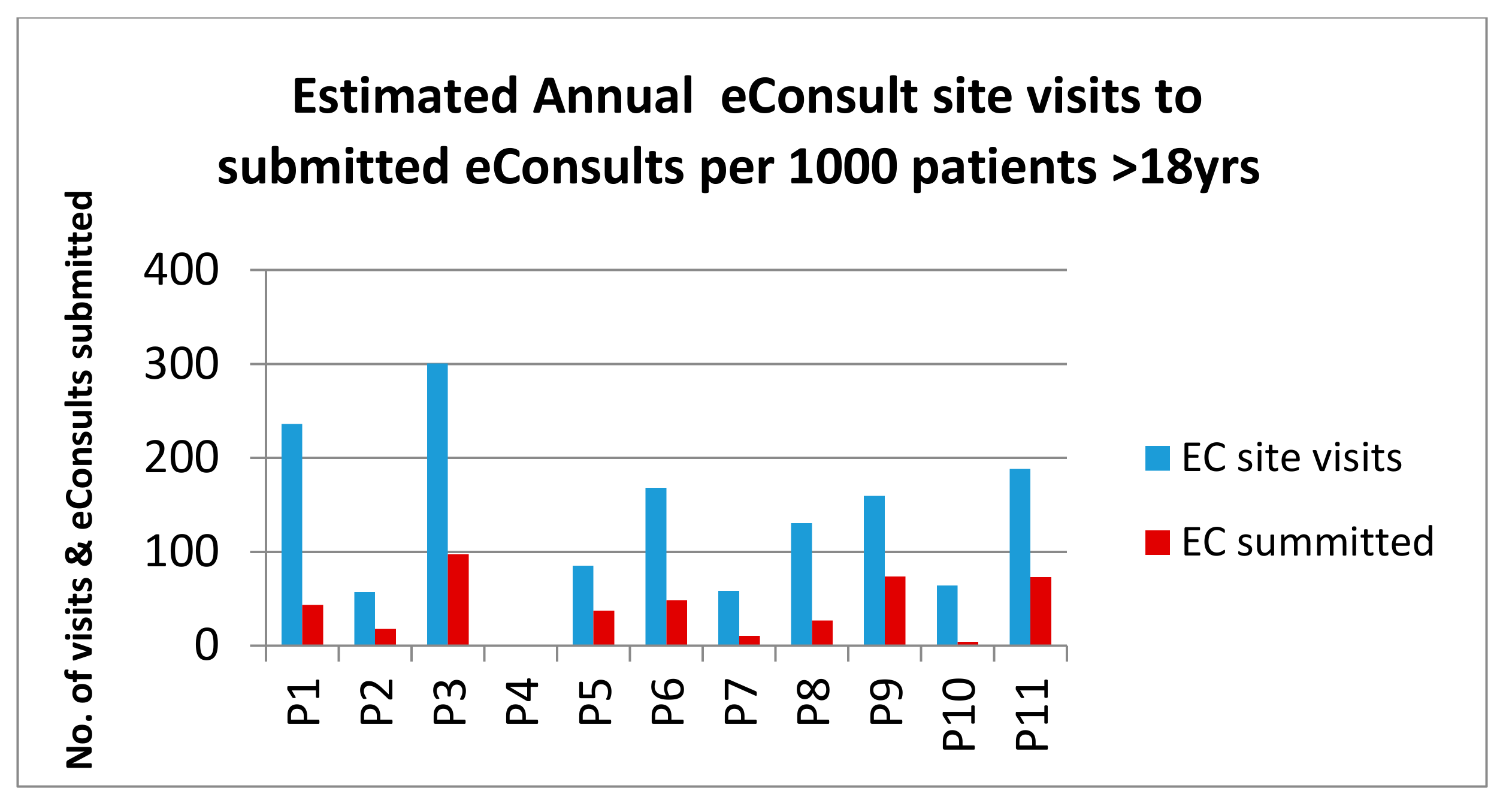
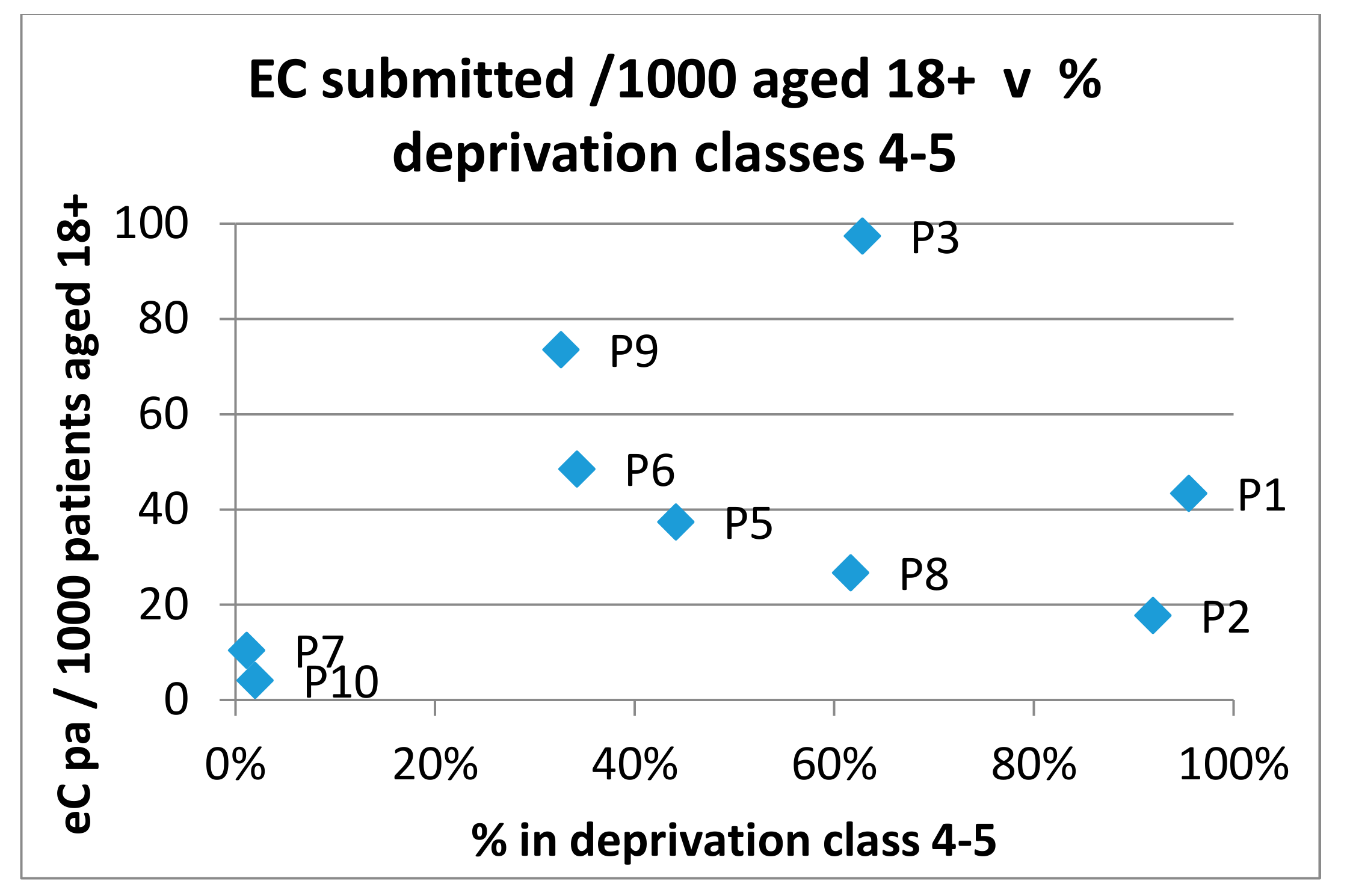
Figure 10. If a cost of £0.63 per patient per year is used, a maximum 73% of GP consultations can be saved per eConsult submitted, then a submission rate of just over 0.5 eConsults per annum per patient is required for breakeven (the average submission rate in the Scottish pilot was 0.05 per patient with a maximum rate of 0.13 being recorded at practice P3 in August 2017, see
Appendix C). If the percentage of GP appointments saved is lower, then higher submission rates are required for breakeven.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}










