Young-Adult Polycystic Kidney Disease is Associated with Major Cardiovascular Complications


 ,
,
Abstract
:1. Background
2. Materials and Methods
2.1. Data Source
2.2. Data Availability Statement
2.3. Ethics Statement
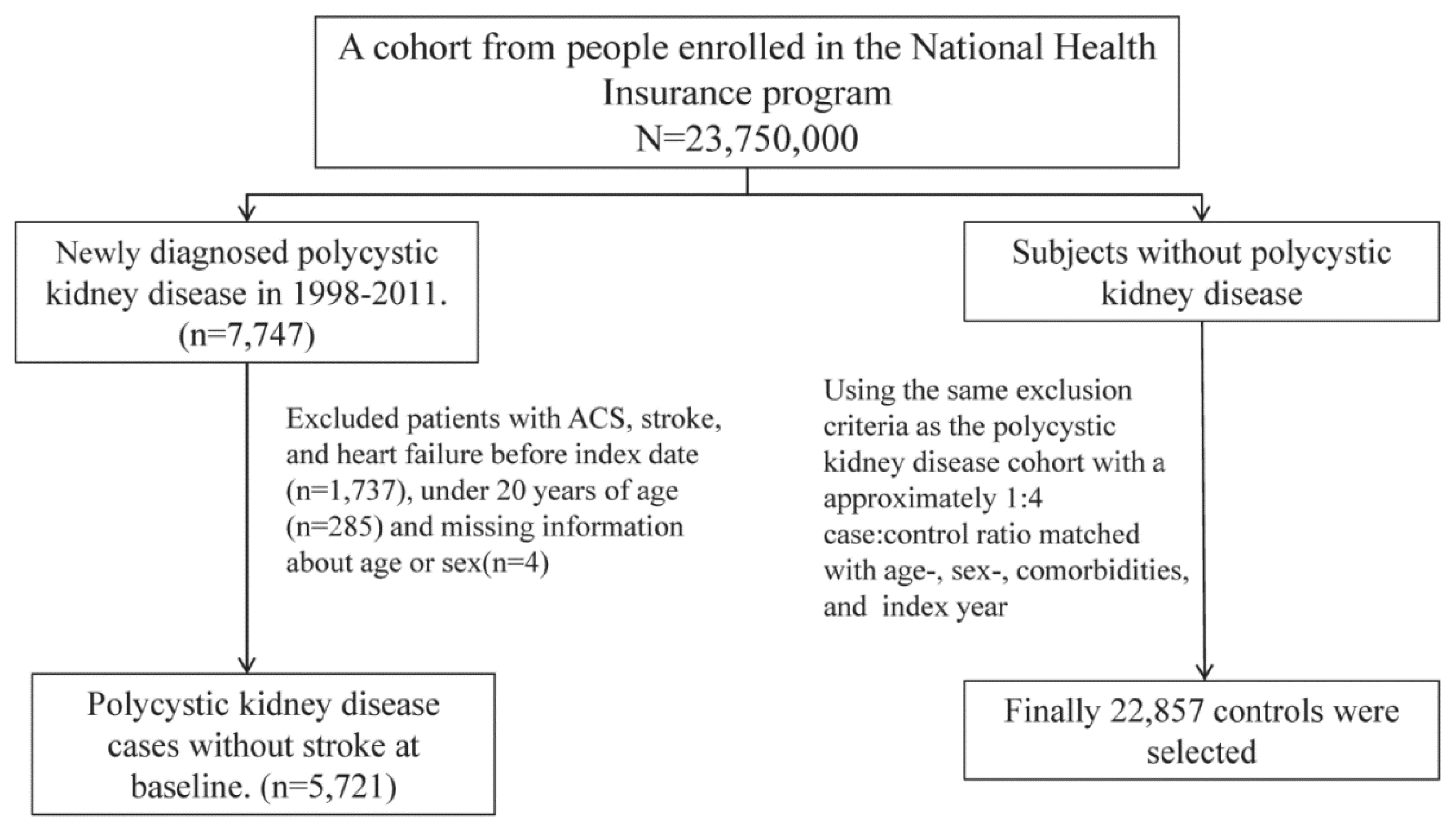
2.4. Study Patients
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Reference
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| PKD | polycystic kidney disease |
| ACS | acute coronary syndrome |
| CHF | congestive heart failure |
| CI | confidence interval |
| VSMC | vascular smooth muscle cells |
| NHIRD | National Health Insurance Research Database |
| ICD-9-CM | International Classification of Diseases, Ninth Revision, Clinical Modification |
| HR | hazard ratio |
References
- Kurschat, C.E.; Muller, R.U.; Franke, M.; Maintz, D.; Schermer, B.; Benzing, T. An approach to cystic kidney diseases: The clinician’s view. Nat. Rev. Nephrol. 2014, 10, 687–699. [Google Scholar] [CrossRef] [PubMed]
- Torres, V.E.; Harris, P.C.; Pirson, Y. Autosomal dominant polycystic kidney disease. Lancet 2007, 369, 1287–1301. [Google Scholar] [CrossRef]
- Bichet, D.; Peters, D.; Patel, A.J.; Delmas, P.; Honore, E. Cardiovascular polycystins: Insights from autosomal dominant polycystic kidney disease and transgenic animal models. Trends Cardiovasc. Med. 2006, 16, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Boulter, C.; Mulroy, S.; Webb, S.; Fleming, S.; Brindle, K.; Sandford, R. Cardiovascular, skeletal, and renal defects in mice with a targeted disruption of the PKD1 gene. Proc. Natl. Acad. Sci. USA 2001, 98, 12174–12179. [Google Scholar] [CrossRef] [PubMed]
- Torres, V.E.; Cai, Y.; Chen, X.; Wu, G.Q.; Geng, L.; Cleghorn, K.A.; Johnson, C.M.; Somlo, S. Vascular expression of polycystin-2. J. Am. Soc. Nephrol. 2001, 12, 1–9. [Google Scholar] [PubMed]
- Griffin, M.D.; Torres, V.E.; Grande, J.P.; Kumar, R. Vascular expression of polycystin. J. Am. Soc. Nephrol. 1997, 8, 616–626. [Google Scholar] [PubMed]
- Kip, S.N.; Hunter, L.W.; Ren, Q.; Harris, P.C.; Somlo, S.; Torres, V.E.; Sieck, G.C.; Qian, Q. [Ca2+]i reduction increases cellular proliferation and apoptosis in vascular smooth muscle cells: Relevance to the ADPKD phenotype. Circ. Res. 2005, 96, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Marx, S.O.; Jayaraman, T.; Go, L.O.; Marks, A.R. Rapamycin-FKBP inhibits cell cycle regulators of proliferation in vascular smooth muscle cells. Circ. Res. 1995, 76, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Martin, K.A.; Rzucidlo, E.M.; Merenick, B.L.; Fingar, D.C.; Brown, D.J.; Wagner, R.J.; Powell, R.J. The mTOR/p70 S6K1 pathway regulates vascular smooth muscle cell differentiation. Am. J. Physiol. Cell Physiol. 2004, 286, C507–C517. [Google Scholar] [CrossRef] [PubMed]
- Morice, M.C.; Serruys, P.W.; Sousa, J.E.; Fajadet, J.; Ban Hayashi, E.; Perin, M.; Colombo, A.; Schuler, G.; Barragan, P.; Guagliumi, G.; et al. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N. Engl. J. Med. 2002, 346, 1773–1780. [Google Scholar] [CrossRef] [PubMed]
- Gallo, R.; Padurean, A.; Jayaraman, T.; Marx, S.; Roque, M.; Adelman, S.; Chesebro, J.; Fallon, J.; Fuster, V.; Marks, A.; et al. Inhibition of intimal thickening after balloon angioplasty in porcine coronary arteries by targeting regulators of the cell cycle. Circulation 1999, 99, 2164–2170. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.C.; Torres, V.E. Genetic mechanisms and signaling pathways in autosomal dominant polycystic kidney disease. J. Clin. Investig. 2014, 124, 2315–2324. [Google Scholar] [CrossRef] [PubMed]
- Lieberthal, W.; Levine, J.S. The role of the mammalian target of rapamycin (mTOR) in renal disease. J. Am. Soc. Nephrol. 2009, 20, 2493–2502. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.; Kim, J.; Schrier, R.W.; Edelstein, C.L. Rapamycin markedly slows disease progression in a rat model of polycystic kidney disease. J. Am. Soc. Nephrol. 2005, 16, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Shillingford, J.M.; Murcia, N.S.; Larson, C.H.; Low, S.H.; Hedgepeth, R.; Brown, N.; Flask, C.A.; Novick, A.C.; Goldfarb, D.A.; Kramer-Zucker, A.; et al. The mTOR pathway is regulated by polycystin-1, and its inhibition reverses renal cystogenesis in polycystic kidney disease. Proc. Natl. Acad. Sci. USA 2006, 103, 5466–5471. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.M.; Chuang, Y.W.; Yu, M.C.; Huang, S.T.; Chou, C.Y.; Lin, C.L.; Chiu, C.C.; Kao, C.H. New-onset Atrial Fibrillation is Associated With Polycystic Kidney Disease: A Nationwide Population-based Cohort Study. Medicine (Baltimore) 2016, 95, e2623. [Google Scholar] [CrossRef] [PubMed]
- Irazabal, M.V.; Huston, J., 3rd; Kubly, V.; Rossetti, S.; Sundsbak, J.L.; Hogan, M.C.; Harris, P.C.; Brown, R.D., Jr.; Torres, V.E. Extended follow-up of unruptured intracranial aneurysms detected by presymptomatic screening in patients with autosomal dominant polycystic kidney disease. Clin. J. Am. Soc. Nephrol. 2011, 6, 1274–1285. [Google Scholar] [CrossRef] [PubMed]
- Fick, G.M.; Johnson, A.M.; Hammond, W.S.; Gabow, P.A. Causes of death in autosomal dominant polycystic kidney disease. J. Am. Soc. Nephrol. 1995, 5, 2048–2056. [Google Scholar] [PubMed]
- Ecder, T.; Schrier, R.W. Cardiovascular abnormalities in autosomal-dominant polycystic kidney disease. Nat. Rev. Nephrol. 2009, 5, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Fine, J.P.; Gray, R.J. A proportional hazards model for the subdistribution of a competing risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Ecder, T.; Schrier, R.W. Hypertension in autosomal-dominant polycystic kidney disease: Early occurrence and unique aspects. J. Am. Soc. Nephrol. 2001, 12, 194–200. [Google Scholar] [PubMed]
- Alfonso, F.; Paulo, M.; Gonzalo, N.; Dutary, J.; Jimenez-Quevedo, P.; Lennie, V.; Escaned, J.; Bañuelos, C.; Hernandez, R.; Macaya, C. Diagnosis of spontaneous coronary artery dissection by optical coherence tomography. J. Am. Coll. Cardiol. 2012, 59, 1073–1079. [Google Scholar] [CrossRef] [PubMed]
- Hadimeri, H.; Lamm, C.; Nyberg, G. Coronary aneurysms in patients with autosomal dominant polycystic kidney disease. J. Am. Soc. Nephrol. 1998, 9, 837–841. [Google Scholar] [PubMed]
- Itty, C.T.; Farshid, A.; Talaulikar, G. Spontaneous coronary artery dissection in a woman with polycystic kidney disease. Am. J. Kidney Dis. 2009, 53, 518–521. [Google Scholar] [CrossRef] [PubMed]
- Magadle, R.; Weiner, P.; Rabner, M.; Mizrahi-Reuveni, M.; Davidovich, A. Polycystic kidney disease as a new risk factor for coronary events. Isr. Med. Assoc. J. 2002, 4, 21–23. [Google Scholar] [PubMed]
- Qian, Q.; Li, M.; Cai, Y.; Ward, C.J.; Somlo, S.; Harris, P.C.; Torres, V.E. Analysis of the polycystins in aortic vascular smooth muscle cells. J. Am. Soc. Nephrol. 2003, 14, 2280–2287. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Markowitz, G.S.; Li, L.; D’Agati, V.D.; Factor, S.M.; Geng, L.; Tibara, S.; Tuchman, J.; Cai, Y.; Park, J.H.; et al. Cardiac defects and renal failure in mice with targeted mutations in PKD2. Nat. Genet. 2000, 24, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.M.; Lin, C.L.; Chang, S.N.; Sung, F.C.; Kao, C.H. Increased risk of stroke in patients with chronic kidney disease after recurrent hypoglycemia. Neurology 2014, 83, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Vrints, C.J. Spontaneous coronary artery dissection. Heart 2010, 96, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, K.H.; Thuesen, L.; Kristensen, I.B.; Christiansen, E.H. Spontaneous coronary artery dissection: A Western Denmark Heart Registry study. Catheter. Cardiovasc. Interv. 2009, 74, 710–717. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age, Year | Polycystic Kidney Disease | p-Value | |||
|---|---|---|---|---|---|
| Yes | No | ||||
| (N = 5721) | (N = 22,857) | ||||
| N | % | N | % | ||
| 0.99 | |||||
| 20–49 | 2080 | 36.4 | 8308 | 36.4 | |
| 50–64 | 1676 | 29.3 | 6695 | 29.3 | |
| ≥65 | 1965 | 34.4 | 7854 | 34.4 | |
| Median (IQR) # | 56.0 | (45.1–70.3) | 56.1 | (45.1–70.5) | 0.76 |
| Gender | 0.98 | ||||
| Female | 2250 | 44.6 | 10,192 | 44.6 | |
| Male | 3171 | 55.4 | 12,665 | 55.4 | |
| Comorbidity | |||||
| Hypertension | 2504 | 43.8 | 10,006 | 43.8 | 0.99 |
| Diabetes | 610 | 10.7 | 2432 | 10.6 | 0.96 |
| Hyperlipidemia | 236 | 4.13 | 933 | 4.08 | 0.88 |
| COPD | 327 | 5.72 | 1293 | 5.66 | 0.86 |
| Chronic kidney disease | 1234 | 21.6 | 4915 | 21.5 | 0.91 |
| ESRD | 564 | 9.86 | 2239 | 9.80 | 0.89 |
| Variable | Polycystic Kidney Disease | Crude SHR † (95% CI) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes | No | ||||||||
| N | Event | PY | Rate # | N | Event | PY | Rate # | ||
| ACS | |||||||||
| All | 5721 | 252 | 29,323 | 8.59 | 22,857 | 790 | 128,080 | 6.17 | 1.40(1.22, 1.61) |
| Unstable angina | 58 | 1.98 | 161 | 1.26 | 1.41(1.05, 1.89) | ||||
| NSTMI | 21 | 0.72 | 77 | 0.60 | 0.94(0.59, 1.50) | ||||
| STMI | 69 | 2.35 | 238 | 1.86 | 1.14(0.88, 1.49) | ||||
| Gender | |||||||||
| Female | 2550 | 72 | 14,002 | 5.14 | 10,192 | 245 | 59,827 | 4.10 | 1.26(0.98, 1.64) |
| Male | 3171 | 180 | 15,322 | 11.8 | 12,665 | 545 | 68,253 | 7.99 | 1.47(1.24, 1.74) |
| Age, year | |||||||||
| 20–49 | 2080 | 54 | 12,584 | 4.29 | 8308 | 131 | 51,120 | 2.56 | 1.61(1.18, 2.21) |
| 50–64 | 1676 | 84 | 8865 | 9.48 | 6695 | 216 | 38,289 | 5.64 | 1.67(1.30, 2.15) |
| ≥65 | 1965 | 114 | 7874 | 14.5 | 7854 | 443 | 38,671 | 11.5 | 1.28(1.04, 1.57) |
| Comorbidity § | |||||||||
| No | 37 | 2 | 268 | 7.47 | 148 | 7 | 1101 | 6.36 | 1.11(0.23, 5.24) |
| Yes | 5684 | 250 | 29,055 | 8.60 | 22,709 | 783 | 126,978 | 6.17 | 1.40(1.22, 1.61) |
| Stroke | |||||||||
| All | 5721 | 609 | 28,395 | 21.5 | 22,857 | 2002 | 124,216 | 16.1 | 1.40(1.28, 1.53) |
| Hemorrhagic stroke | 175 | 28,396 | 6.16 | 369 | 124,216 | 2.97 | 2.12(1.78, 2.53) | ||
| Ischemic stroke | 434 | 28,396 | 15.3 | 1633 | 124,216 | 13.2 | 1.20(1.08, 1.33) | ||
| Gender | |||||||||
| Female | 2550 | 237 | 13,533 | 17.5 | 10,192 | 677 | 58,390 | 11.6 | 1.62(1.40, 1.88) |
| Male | 3171 | 372 | 14,863 | 25.0 | 12,665 | 1325 | 65,826 | 20.1 | 1.29(1.15, 1.45) |
| Age, year | |||||||||
| 20–49 | 2080 | 108 | 12,419 | 8.70 | 8308 | 265 | 50,742 | 5.22 | 1.65(1.32, 2.07) |
| 50–64 | 1676 | 176 | 8628 | 20.4 | 6695 | 537 | 37,243 | 14.4 | 1.41(1.19, 1.67) |
| ≥65 | 1965 | 325 | 7349 | 44.2 | 7854 | 1200 | 36,231 | 33.1 | 1.35(1.19, 1.52) |
| Comorbidity § | |||||||||
| No | 37 | 4 | 254 | 15.7 | 148 | 17 | 1060 | 16.0 | 0.98(0.33, 2.89) |
| Yes | 5684 | 605 | 28,142 | 21.5 | 22,709 | 1985 | 123,156 | 16.1 | 1.41(1.28, 1.54) |
| Congestive heart failure | |||||||||
| All | 5721 | 471 | 28,987 | 16.3 | 22,857 | 1410 | 126,905 | 11.1 | 1.49(1.34, 1.65) |
| Gender | |||||||||
| Female | 2550 | 171 | 13,806 | 12.4 | 10,192 | 531 | 59,153 | 8.98 | 1.43(1.21, 1.69) |
| Male | 3171 | 300 | 15,181 | 19.8 | 12,665 | 879 | 67,751 | 13.0 | 1.52(1.34, 1.73) |
| Age, year | |||||||||
| 20–49 | 2080 | 69 | 12,585 | 5.48 | 8308 | 150 | 51,123 | 2.93 | 1.82(1.37, 2.42) |
| 50–64 | 1676 | 116 | 8866 | 13.1 | 6695 | 336 | 37,950 | 8.85 | 1.46(1.18, 1.80) |
| ≥65 | 1965 | 286 | 7537 | 38.0 | 7854 | 924 | 37,832 | 24.4 | 1.57(1.38, 1.80) |
| Comorbidity § | |||||||||
| No | 37 | 0 | 276 | 0.00 | 148 | 7 | 1107 | 6.32 | - |
| Yes | 5684 | 471 | 28,711 | 16.4 | 22,709 | 1403 | 125,798 | 11.2 | 1.50(1.35, 1.66) |
| Variable | Polycystic Kidney Disease | Crude HR † (95% CI) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes | No | ||||||||
| N | Event | PY | Rate # | N | Event | PY | Rate # | ||
| All | 5721 | 1217 | 30,045 | 40.5 | 22,857 | 3218 | 130,270 | 24.7 | 1.64(1.53, 1.75) |
| Gender | |||||||||
| Female | 2550 | 416 | 14,224 | 29.3 | 10,192 | 1012 | 60,548 | 16.7 | 1.75(1.57, 1.97) |
| Male | 3171 | 801 | 15,822 | 50.6 | 12,665 | 2206 | 69,721 | 31.6 | 1.60(1.47, 1.73) |
| Age, year | |||||||||
| 20–49 | 2080 | 191 | 12,778 | 15.0 | 8308 | 421 | 51,648 | 8.15 | 1.84(1.55, 2.18) |
| 50–64 | 1676 | 347 | 9154 | 37.9 | 6695 | 875 | 38,931 | 22.5 | 1.69(1.50, 1.92) |
| ≥65 | 1965 | 679 | 8113 | 83.7 | 7854 | 1922 | 39,690 | 48.4 | 1.73(1.59, 1.89) |
| Comorbidity § | |||||||||
| No | 37 | 7 | 276 | 25.3 | 148 | 13 | 1122 | 11.6 | 2.14(0.86, 5.38) |
| Yes | 5684 | 1210 | 29,769 | 40.7 | 22,709 | 3205 | 129,148 | 24.8 | 1.64(1.53, 1.75) |
| Variable | ACS | Stroke | Congestive Heart Failure | Mortality | ||||
|---|---|---|---|---|---|---|---|---|
| Crude SHR † (95% CI) | Adjusted SHR ‡ (95% CI) | Crude SHR † (95% CI) | Adjusted SHR ‡ (95% CI) | Crude SHR † (95% CI) | Adjusted SHR ‡ (95% CI) | Crude HR † (95% CI) | Adjusted HR ‡ (95% CI) | |
| PKD | 1.40(1.22, 1.61) | 1.40(1.22, 1.62) | 1.40(1.28, 1.53) | 1.39(1.27, 1.52) | 1.49(1.34, 1.65) | 1.51(1.36, 1.68) | 1.64(1.53, 1.75) | 1.71(1.60, 1.83) |
| Gender (Men vs. women) | 1.58(1.39, 1.79) | 1.55(1.36, 1.77) | 1.30(1.20, 1.40) | 1.27(1.17, 1.38) | 1.07(0.98,1.17) | 1.03(0.94, 1.13) | 1.84(1.73, 1.96) | 1.42(1.33, 1.51) |
| Age, years | ||||||||
| 20–49 | 1(Reference) | 1(Reference) | 1(Reference) | 1(Reference) | 1(Reference) | 1(Reference) | 1(Reference) | 1(Reference) |
| 50–64 | 1.37(1.03, 1.82) | 1.19(0.89, 1.59) | 1.28(1.04, 1.57) | 1.04(0.84, 1.28) | 1.79(1.40, 2.29) | 1.45(1.13, 1.84) | 2.69(2.44, 2.96) | 2.32(2.11, 2.56) |
| ≥65 | 1.23(0.99, 1.54) | 1.08(0.87, 1.35) | 1.25(1.07, 1.46) | 1.12(0.96, 1.30) | 1.31(1.08, 1.58) | 1.10(0.91, 1.33) | 5.78(5.29, 6.32) | 5.16(4.72, 5.65) |
| Baseline comorbidities (yes vs. no) | ||||||||
| Hypertension | 1.96(1.74, 2.21) | 1.76(1.55, 1.99) | 1.61(1.49, 1.74) | 1.51(1.39, 1.63) | 1.69(1.54, 1.85) | 1.53(1.39, 1.68) | 1.69(1.59, 1.79) | 1.21(1.14, 1.28) |
| Diabetes | 2.21(1.90, 2.57) | 1.87(1.60, 2.18) | 1.79(1.62, 1.98) | 1.65(1.48, 1.83) | 2.20(1.97, 2.45) | 2.00(1.78, 2.24) | 2.07(1.92, 2.24) | 1.67(1.54, 1.81) |
| Hyperlipidemia | 2.40(1.95, 2.95) | 1.87((1.51, 2.32) | 1.41(1.20, 1.67) | 1.12(0.95, 1.33) | 1.69(1.41, 2.02) | 1.33(1.10, 1.59) | 1.07(0.93, 1.24) | 0.88(0.76, 1.02) |
| COPD | 1.37(1.10, 1.70) | 1.16(0.93, 1.44) | 1.42(1.25, 1.61) | 1.30(1.14, 1.48) | 1.72(1.50, 1.98) | 1.52(1.32, 1.76) | 2.76(2.51, 3.03) | 1.60(1.45, 1.76) |
| CKD | 2.20(1.94, 2.49) | 1.90(1.65, 2.20) | 1.73(1.60, 1.89) | 1.64(1.49, 1.81) | 2.52(2.30, 2.76) | 2.37(2.14, 2.63) | 3.36(3.17, 3.56) | 2.76(2.58, 2.95) |
| ESRD | 2.12(1.78, 2.52) | 1.32(1.07, 1.61) | 1.52(1.33, 1.73) | 1.03(0.89, 1.20) | 2.19(1.92, 2.50) | 1.29(1.11, 1.50) | 2.80(2.60, 3.02) | 1.60(1.47, 1.74) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chuang, Y.-W.; Yu, T.-M.; Huang, S.-T.; Sun, K.-T.; Lo, Y.-C.; Fu, P.-K.; Lee, B.-J.; Chen, C.-H.; Lin, C.-L.; Kao, C.-H. Young-Adult Polycystic Kidney Disease is Associated with Major Cardiovascular Complications. Int. J. Environ. Res. Public Health 2018, 15, 903. https://doi.org/10.3390/ijerph15050903
Chuang Y-W, Yu T-M, Huang S-T, Sun K-T, Lo Y-C, Fu P-K, Lee B-J, Chen C-H, Lin C-L, Kao C-H. Young-Adult Polycystic Kidney Disease is Associated with Major Cardiovascular Complications. International Journal of Environmental Research and Public Health. 2018; 15(5):903. https://doi.org/10.3390/ijerph15050903
Chicago/Turabian StyleChuang, Ya-Wen, Tung-Min Yu, Shih-Ting Huang, Kuo-Ting Sun, Ying-Chih Lo, Pin-Kuei Fu, Bor-Jen Lee, Cheng-Hsu Chen, Cheng-Li Lin, and Chia-Hung Kao. 2018. "Young-Adult Polycystic Kidney Disease is Associated with Major Cardiovascular Complications" International Journal of Environmental Research and Public Health 15, no. 5: 903. https://doi.org/10.3390/ijerph15050903
APA StyleChuang, Y. -W., Yu, T. -M., Huang, S. -T., Sun, K. -T., Lo, Y. -C., Fu, P. -K., Lee, B. -J., Chen, C. -H., Lin, C. -L., & Kao, C. -H. (2018). Young-Adult Polycystic Kidney Disease is Associated with Major Cardiovascular Complications. International Journal of Environmental Research and Public Health, 15(5), 903. https://doi.org/10.3390/ijerph15050903