Time to Rethink Refugee and Migrant Health in Europe: Moving from Emergency Response to Integrated and Individualized Health Care Provision for Migrants and Refugees

 , ,
, , 
{kind=link}
Abstract
:1. Introduction
2. R&M Health in the European Context
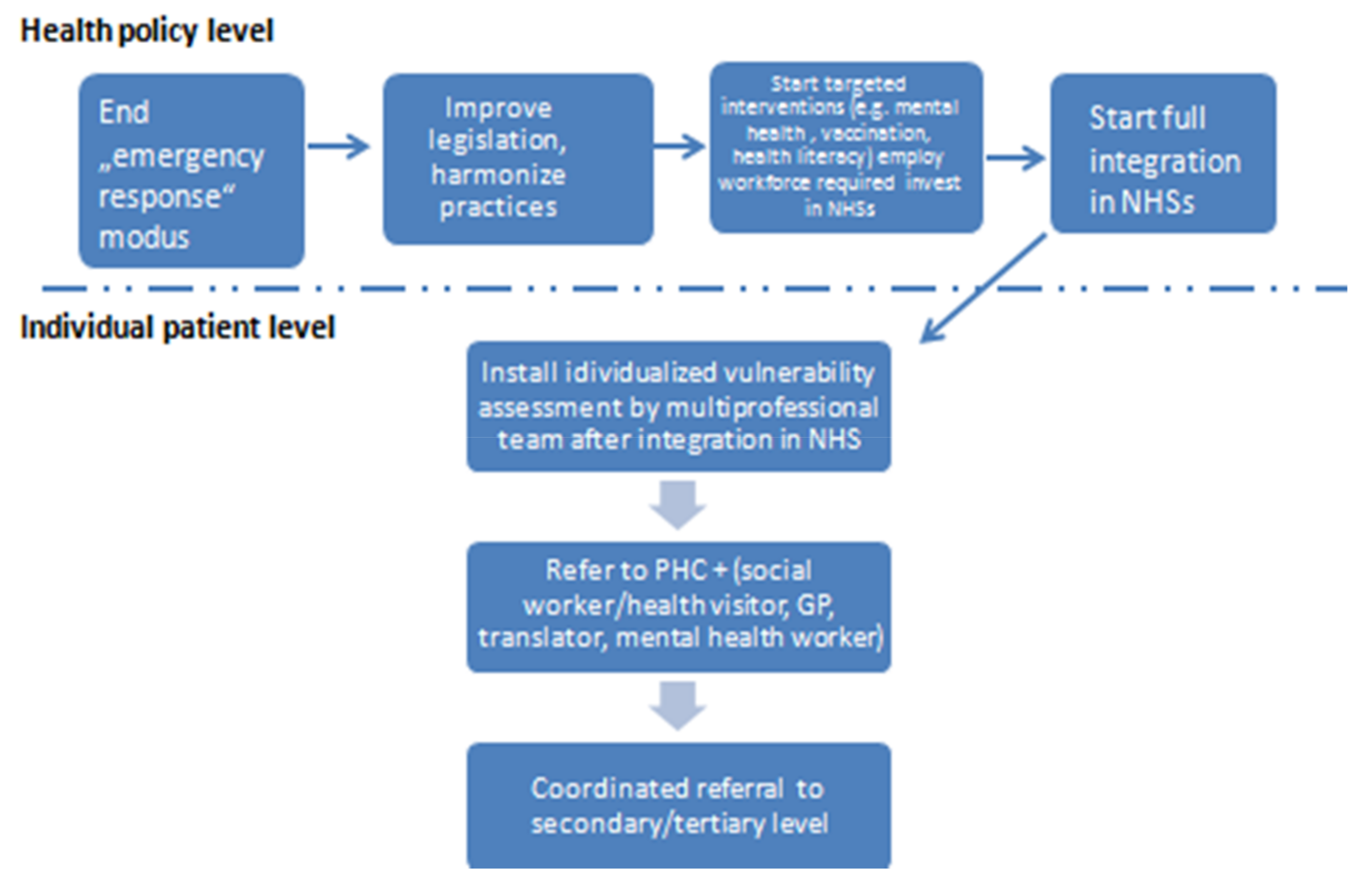
3. The Need to Move from Emergency Response to Integrated and Individualized Health Care Provision for Migrants and Refugees
4. Conclusions
Author Contributions
Conflicts of Interest
References
- World Health Organization (WHO). Promoting the Health of Refugees and Migrants—Draft Framework of Priorities and Guiding Principles to Promote the Health of Refugees and Migrants; World Health Assembly, A70/24, Provisional Agenda Item 13.7; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Keely, C.; Reed, H.; Waldman, R. Understanding Mortality Patterns in Complex Humanitarian Emergencies. In Forced Migration & Mortality; Reed, H.E., Keely, C.B., Eds.; Commission on Behavioral and Social Sciences and Education National Research Council; National Academy Press: Washington, DC, USA, 2001; pp. 1–51. [Google Scholar]
- Levecque, K.; Lodewyckx, I.; Vranken, J. Depression and generalised anxiety in the general population in Belgium: A comparison between native and immigrant groups. J. Affect. Disord. 2007, 97, 229–239. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health; Final Report of the Commission on Social Determinants of Health; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Tinghog, P.; Hemmingsson, T.; Lundberg, I. To what extent may the association between immigrant status and mental illness be explained by socioeconomic factors? Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Fleischman, Y.; Willen, S.S.; Davidovitch, N.; Mor, Z. Migration as a social determinant of health for irregular migrants: Israel as case study. Soc. Sci. Med. 2015, 147, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, C.; Kiss, L.; Hossain, M. Migration and health: A framework for 21st century policy-making. PLoS Med. 2011, 8, e1001034. [Google Scholar] [CrossRef] [PubMed]
- UNHCR. Meditterenean Situation Sea Arrivals. 2018. Available online: https://data2.unhcr.org/en/situations/mediterranean (accessed on 13 April 2018).
- United Nations DoEaSA, Population Division; International Migration Report; United Nations: New York, NY, USA, 2017.
- Strandell, H.; Wolff, P. The EU in the World, 2016 ed.; Eurostat: Brussels, Belgium, 2016; pp. 77–90. [Google Scholar]
- Freedman, J. Sexual and gender-based violence against refugee women: A hidden aspect of the refugee “crisis”. Reprod. Health Matters 2016, 24, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.; Haeghebaert, S.; Merlin, B.; Antona, D.; Simon, N.; Elmouden, M.; Battist, F.; Janssens, M.; Wyndels, K.; Chaud, P. Measles outbreak in a refugee settlement in Calais, France: January to February 2016. Euro Surveill. 2016, 21, 30167. [Google Scholar] [CrossRef] [PubMed]
- Mellou, K.; Chrisostomou, A.; Sideroglou, T.; Georgakopoulou, T.; Kyritsi, M.; Hadjichristodoulou, C.; Tsiodras, S. Hepatitis A among refugees, asylum seekers and migrants living in hosting facilities, Greece, April to December 2016. Euro Surveill. 2017, 22, 30448. [Google Scholar] [CrossRef] [PubMed]
- Vairo, F.; Di Bari, V.; Panella, V.; Quintavalle, G.; Torchia, S.; Serra, M.C.; Sinopoli, M.T.; Lopalco, M.; Ceccarelli, G.; Ferraro, F.; et al. An outbreak of chickenpox in an asylum seeker centre in Italy: Outbreak investigation and validity of reported chickenpox history, December 2015–May 2016. Euro Surveill. 2017, 22. [Google Scholar] [CrossRef] [PubMed]
- Blitz, B.K.; d’Angelo, A.; Kofman, E.; Montagna, N. Health Challenges in Refugee Reception: Dateline Europe 2016. Int. J. Environ. Res. Public Health 2017, 14, 1484. [Google Scholar] [CrossRef] [PubMed]
- Anagnostopoulos, D.C.; Giannakopoulos, G.; Christodoulou, N.G. A Compounding Mental Health Crisis: Reflections from the Greek Experience with Syrian Refugees. Am. J. Psychiatry 2016, 173, 1081–1082. [Google Scholar] [CrossRef] [PubMed]
- Jefee-Bahloul, H.; Bajbouj, M.; Alabdullah, J.; Hassan, G.; Barkil-Oteo, A. Mental health in Europe’s Syrian refugee crisis. Lancet Psychiatry 2016, 3, 315–317. [Google Scholar] [CrossRef]
- Sijbrandij, M.; Acarturk, C.; Bird, M.; Bryant, R.A.; Burchert, S.; Carswell, K.; de Jong, J.; Dinesen, C.; Dawson, K.S.; el Chammay, R.; et al. Strengthening mental health care systems for Syrian refugees in Europe and the Middle East: Integrating scalable psychological interventions in eight countries. Eur. J. Psychotraumatol. 2017, 8, 1388102. [Google Scholar] [CrossRef] [PubMed]
- Bozorgmehr, K.; Razum, O. Effect of Restricting Access to Health Care on Health Expenditures among Asylum-Seekers and Refugees: A Quasi-Experimental Study in Germany, 1994–2013. PLoS ONE 2015, 10, e0131483. [Google Scholar] [CrossRef] [PubMed]
- Gray, B.H.; van Ginneken, E. Health care for undocumented migrants: European approaches. Issue Brief. 2012, 33, 1–12. [Google Scholar] [PubMed]
- Médecins du Monde. European Network to Reduce Vulnerabilities in Health-Observatory Reports; Legal Report on Access to Healthcare in 16 European Countries; Médecins du Monde: Paris, France, 2017. [Google Scholar]
- EWSI Editorial Team EC. Migrant Health across Europe: Little Structural Policies, Many Encouraging Practices. 2018. Available online: https://ec.europa.eu/migrant-integration/feature/migrant-health-across-europe (accessed on 12 April 2018).
- Eurostat Monitoring Report. How Has the EU Progressed towards the Sustainable Development Goals? 2017. Available online: http://ec.europa.eu/eurostat/documents/2995521/8462309/8-20112017-AP-EN.pdf/f5e04614-0595-47ce-b17f-0f87648ddcd5 (accessed on 20 November 2017).
- European Commission. Proposal for a Directive of the European Parliament and of the Council Laying Down Standards for the Reception of Applicants for International Protection (Recast) COM (2016) 465 Final; European Commission: Brussels, Belgium, 2016. [Google Scholar]

© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puchner, K.; Karamagioli, E.; Pikouli, A.; Tsiamis, C.; Kalogeropoulos, A.; Kakalou, E.; Pavlidou, E.; Pikoulis, E. Time to Rethink Refugee and Migrant Health in Europe: Moving from Emergency Response to Integrated and Individualized Health Care Provision for Migrants and Refugees. Int. J. Environ. Res. Public Health 2018, 15, 1100. https://doi.org/10.3390/ijerph15061100
Puchner K, Karamagioli E, Pikouli A, Tsiamis C, Kalogeropoulos A, Kakalou E, Pavlidou E, Pikoulis E. Time to Rethink Refugee and Migrant Health in Europe: Moving from Emergency Response to Integrated and Individualized Health Care Provision for Migrants and Refugees. International Journal of Environmental Research and Public Health. 2018; 15(6):1100. https://doi.org/10.3390/ijerph15061100
Chicago/Turabian StylePuchner, Karl, Evika Karamagioli, Anastasia Pikouli, Costas Tsiamis, Athanasios Kalogeropoulos, Eleni Kakalou, Elena Pavlidou, and Emmanouil Pikoulis. 2018. "Time to Rethink Refugee and Migrant Health in Europe: Moving from Emergency Response to Integrated and Individualized Health Care Provision for Migrants and Refugees" International Journal of Environmental Research and Public Health 15, no. 6: 1100. https://doi.org/10.3390/ijerph15061100
APA StylePuchner, K., Karamagioli, E., Pikouli, A., Tsiamis, C., Kalogeropoulos, A., Kakalou, E., Pavlidou, E., & Pikoulis, E. (2018). Time to Rethink Refugee and Migrant Health in Europe: Moving from Emergency Response to Integrated and Individualized Health Care Provision for Migrants and Refugees. International Journal of Environmental Research and Public Health, 15(6), 1100. https://doi.org/10.3390/ijerph15061100